You might also like
- Cardiology PDFDocument13 pagesCardiology PDFDeepthi DNo ratings yet
- Abdomen Engl PDFDocument51 pagesAbdomen Engl PDFShuler0071No ratings yet
- Oxygen Therapy DR RSWDocument61 pagesOxygen Therapy DR RSWdr.chotimatulhusnaNo ratings yet
- PericarditisDocument29 pagesPericarditisPavin KumarNo ratings yet
- Tuberculosis 2Document43 pagesTuberculosis 2Qii ishNo ratings yet
- 2-Pelvic Walls, Joints, Vessels & NervesDocument32 pages2-Pelvic Walls, Joints, Vessels & NervesAbdul Rafay ShaikhNo ratings yet
- Preoperative PreparationDocument53 pagesPreoperative PreparationBir Mohammad Sonet0% (1)
- Oxygen Therapy: Housemanship Training Programme Department of Anaesthesiology and Intensive CareDocument55 pagesOxygen Therapy: Housemanship Training Programme Department of Anaesthesiology and Intensive CaretorreslysNo ratings yet
- Classical Psychoanalytic TheoryDocument18 pagesClassical Psychoanalytic TheoryDelonix Cattleya RegiaNo ratings yet
- Approach To The Patient With Endocrine DisordersDocument17 pagesApproach To The Patient With Endocrine Disordersseun williamsNo ratings yet
- TuberculosisDocument28 pagesTuberculosisBir Mohammad SonetNo ratings yet
- Module 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - ClementeDocument27 pagesModule 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - Clementeelaine100% (1)
- General Surgery Sample TestDocument16 pagesGeneral Surgery Sample TestNix14No ratings yet
- Feedback Systems in The BodyDocument13 pagesFeedback Systems in The Bodymrmr92No ratings yet
- Shortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesDocument49 pagesShortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesGilbert Solomon Tantono100% (1)
- Advanced Airway Management 4th YearsDocument39 pagesAdvanced Airway Management 4th YearsAmmaarah Isaacs100% (1)
- Oxygen Therapy: Dr. Richard D. Pascua InstructorDocument91 pagesOxygen Therapy: Dr. Richard D. Pascua InstructorFranz goNo ratings yet
- Preoperative Preparation of Patient For SurgeryDocument23 pagesPreoperative Preparation of Patient For SurgeryFauzi SebunyaNo ratings yet
- IntubationDocument41 pagesIntubationNice YouNo ratings yet
- Endotracheal Intubation: Oleh: Dr. Natalia Rasta M Pembimbing: Dr. Eko Widya, Sp. EMDocument22 pagesEndotracheal Intubation: Oleh: Dr. Natalia Rasta M Pembimbing: Dr. Eko Widya, Sp. EMNatalia RastaNo ratings yet
- ICU TriageDocument27 pagesICU TriageAkmal FahrezzyNo ratings yet
- Mechanical VentilationDocument33 pagesMechanical VentilationSalman KhanNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Suture and Suturing PDFDocument165 pagesSuture and Suturing PDFcj bariasNo ratings yet
- ORTHOSIS - and ProthesisDocument112 pagesORTHOSIS - and Prothesismanjukumard2007100% (1)
- Analysis and Interpretation of Assessment ResultsDocument84 pagesAnalysis and Interpretation of Assessment ResultsAlyanna Clarisse Padilla CamposNo ratings yet
- How To Heal Faster From A BreakupDocument285 pagesHow To Heal Faster From A BreakupRebecca OmojuwaNo ratings yet
- Perioperative ManagementDocument3 pagesPerioperative ManagementRaymond De GulaNo ratings yet
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995No ratings yet
- The Preoperative EvaluationDocument25 pagesThe Preoperative Evaluationnormie littlemonsterNo ratings yet
- Click On 1 4 Leaflet PDFDocument88 pagesClick On 1 4 Leaflet PDFEseniya TishkinaNo ratings yet
- LAS Q2-WEEK 1-2-TVL-FBS NC II - Grade 12Document15 pagesLAS Q2-WEEK 1-2-TVL-FBS NC II - Grade 12Xian Julz PaezNo ratings yet
- Evaluation of Acute AbdomenDocument38 pagesEvaluation of Acute Abdomenأبو عبيدةNo ratings yet
- Diagnoses and Management Acute Headache Emergency DepartmentDocument37 pagesDiagnoses and Management Acute Headache Emergency DepartmentBendy Dwi IrawanNo ratings yet
- Rhino SinusitisDocument57 pagesRhino SinusitisArif MohammedNo ratings yet
- Co PDFDocument4 pagesCo PDFReginaJacobNo ratings yet
- CHPT 70 Respiratory Part 2Document56 pagesCHPT 70 Respiratory Part 2helen brockNo ratings yet
- OSCEDocument23 pagesOSCEGaurav Singh100% (1)
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadishemanthshah2801No ratings yet
- Neurological ExaminationDocument71 pagesNeurological ExaminationSiti Nursuhada binti Mohd AminNo ratings yet
- Acute Abdomen The "Black Hole" of MedicineDocument99 pagesAcute Abdomen The "Black Hole" of MedicinedebarajuNo ratings yet
- Cardiac ExaminationDocument23 pagesCardiac ExaminationAreza Eka PermanaNo ratings yet
- Kuliah SuturingDocument69 pagesKuliah SuturingiqiqiqiqiqNo ratings yet
- Far Eastern University - Nicanor Reyes Medical FoundationDocument4 pagesFar Eastern University - Nicanor Reyes Medical FoundationMikee MeladNo ratings yet
- Chest IntubationDocument42 pagesChest IntubationdrusmanjamilhcmdNo ratings yet
- IM 3A PE Cardiology Dr. JumangitDocument12 pagesIM 3A PE Cardiology Dr. JumangitCzara DyNo ratings yet
- The Management of Acute Respiratory Distress SyndromeDocument48 pagesThe Management of Acute Respiratory Distress SyndromeLauraAlvarezMulettNo ratings yet
- Fluid and Electrolyte Management of The Surgical PatientDocument26 pagesFluid and Electrolyte Management of The Surgical PatientYudhi Leo PrimaNo ratings yet
- Seminar On Fluids and Electrolyte ImbalanceDocument69 pagesSeminar On Fluids and Electrolyte ImbalanceShib Shankar Roy100% (4)
- Peptic Ulcers: DR Yotham Phiri Mmed (Surg)Document46 pagesPeptic Ulcers: DR Yotham Phiri Mmed (Surg)Emmanuel MukukaNo ratings yet
- Abdominal Swelling + AscitesDocument29 pagesAbdominal Swelling + AscitesDevina CiayadiNo ratings yet
- Approach To Unconscious PatientDocument23 pagesApproach To Unconscious Patienttantw880% (1)
- Mechanism of Drug Action PDFDocument1 pageMechanism of Drug Action PDFraviomjNo ratings yet
- Tracheobronchial Tree (TBT) : by DR HottorDocument33 pagesTracheobronchial Tree (TBT) : by DR HottorChris ZantiraNo ratings yet
- AnatomageDocument12 pagesAnatomageapi-446183922No ratings yet
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdBilly PeterNo ratings yet
- Emergency DrugsDocument10 pagesEmergency DrugsnieacatleyaNo ratings yet
- Shock: Rose Ann J. Raquiza-Perante Post Graduate InternDocument53 pagesShock: Rose Ann J. Raquiza-Perante Post Graduate InternRose Ann RaquizaNo ratings yet
- Interpretation of CBCDocument35 pagesInterpretation of CBCnth1992No ratings yet
- Pediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIDocument27 pagesPediatric Pharmacology: Dr. Putrya Hawa, M.Biomed Faculty of Medicine, UIIAfied Fitrah100% (1)
- 2021-11 Jenny's PARDS PresentationDocument33 pages2021-11 Jenny's PARDS PresentationJenny WoodruffNo ratings yet
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuNo ratings yet
- Newborn EmergenciesDocument83 pagesNewborn EmergencieshwelpNo ratings yet
- Drugs in ObstetricsDocument95 pagesDrugs in ObstetricsPriya jNo ratings yet
- Lower Airway DiseasesDocument70 pagesLower Airway DiseasesAavash PradhanNo ratings yet
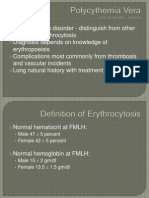
- Polycythemia VeraDocument22 pagesPolycythemia VeraMelisande Rae CiruelaNo ratings yet
- IV CalculationsDocument31 pagesIV CalculationschanaNo ratings yet
- Shock CorrectedDocument70 pagesShock CorrectedrajevikramNo ratings yet
- Antiemetic Prophylaxis For CINV NEJM 2016Document12 pagesAntiemetic Prophylaxis For CINV NEJM 2016tcd_usaNo ratings yet
- Principles of FracturesDocument79 pagesPrinciples of FracturesBir Mohammad SonetNo ratings yet
- Who Offices in CountriesDocument8 pagesWho Offices in CountriesBir Mohammad SonetNo ratings yet
- Body FluidDocument37 pagesBody FluidBir Mohammad SonetNo ratings yet
- Principles of FracturesDocument79 pagesPrinciples of FracturesBir Mohammad SonetNo ratings yet
- Surgical InfectionDocument75 pagesSurgical InfectionBir Mohammad SonetNo ratings yet
- Stomach & DuodenumDocument25 pagesStomach & DuodenumBir Mohammad SonetNo ratings yet
- RabiesDocument28 pagesRabiesBir Mohammad SonetNo ratings yet
- Forensic Viva QuestionsDocument1 pageForensic Viva QuestionsBir Mohammad SonetNo ratings yet
- WHO Report - April 23Document12 pagesWHO Report - April 23CityNewsTorontoNo ratings yet
- Pathology Item CardDocument2 pagesPathology Item CardBir Mohammad SonetNo ratings yet
- Basic Circuit Laws: Georg Ohm Kirchhoff's LawsDocument4 pagesBasic Circuit Laws: Georg Ohm Kirchhoff's LawsrezhabloNo ratings yet
- Design and Development of Alternative Delivery SystemDocument3 pagesDesign and Development of Alternative Delivery Systemfredie unggayNo ratings yet
- Fomrhi 060Document40 pagesFomrhi 060rodolfoNo ratings yet
- Literature Review On Investment DecisionsDocument5 pagesLiterature Review On Investment Decisionsc5t0jsyn100% (1)
- Victims and Perpetrators Testimony of Young Khmer Rouge ComradesDocument83 pagesVictims and Perpetrators Testimony of Young Khmer Rouge Comradesagarratecatalina100% (2)
- Indefinite and Definite ArticlesDocument11 pagesIndefinite and Definite ArticlesRahela FoltNo ratings yet
- 12A & 80G ProcedureDocument4 pages12A & 80G ProcedurekshripalNo ratings yet
- Title Eight Crimes Against Persons: Article 246. ParricideDocument27 pagesTitle Eight Crimes Against Persons: Article 246. ParricideJeric RealNo ratings yet
- BIR Job Aid TP Guide - Enrollment, Login, Change User InfoDocument30 pagesBIR Job Aid TP Guide - Enrollment, Login, Change User InfoMaricor TambalNo ratings yet
- World History Midterm Study GuideDocument2 pagesWorld History Midterm Study GuideMark JacksonNo ratings yet
- González-Rey, F.L. (2018) - Subjectivity and Discourse - Complementary Topics For A Critical PsychologyDocument17 pagesGonzález-Rey, F.L. (2018) - Subjectivity and Discourse - Complementary Topics For A Critical PsychologyFernando AVNo ratings yet
- Whats The Weather LikeDocument3 pagesWhats The Weather Likechristian sosaNo ratings yet
- David Miano - Why Ancient History Matters v02Document16 pagesDavid Miano - Why Ancient History Matters v02Esteban LVNo ratings yet
- Economics of Pohela BoishakhDocument3 pagesEconomics of Pohela BoishakhMohammad Shahjahan SiddiquiNo ratings yet
- BS EN 12596 - Dynamic Viscosity by Vacuum CapillaryDocument22 pagesBS EN 12596 - Dynamic Viscosity by Vacuum CapillaryCraig LongNo ratings yet
- O Level Travel and Tourism 7096 Syllabus 2008 Unit 5 - Marketing and Promotion Recommended Prior KnowledgeDocument7 pagesO Level Travel and Tourism 7096 Syllabus 2008 Unit 5 - Marketing and Promotion Recommended Prior Knowledgemstudy123456No ratings yet
- Prediction of One Repetition Maximal Strength From A A 5-10 Repetition - FemaleDocument6 pagesPrediction of One Repetition Maximal Strength From A A 5-10 Repetition - FemaleOz FalchiNo ratings yet
- Lecture 7 CrosstabsDocument20 pagesLecture 7 CrosstabsibmrNo ratings yet
- Zoom G2.1u English ManualDocument25 pagesZoom G2.1u English ManualKevin KerberNo ratings yet
- Fundamental of Software Engineering: Faculty of Technology Department of Computer Science Debre Tabor UniversityDocument17 pagesFundamental of Software Engineering: Faculty of Technology Department of Computer Science Debre Tabor UniversityBethelhem YetwaleNo ratings yet
- Metformin Drug StudyDocument2 pagesMetformin Drug StudyArone SebastianNo ratings yet
- Session 4 LeadingSelf - FLA Expect The BestDocument16 pagesSession 4 LeadingSelf - FLA Expect The BesthendrikaNo ratings yet
- LS1 - Idioms-WorksheetsDocument2 pagesLS1 - Idioms-WorksheetsMarbz AlsteacherNo ratings yet