You might also like
- Rotator Cuff Injury RehabilitationDocument29 pagesRotator Cuff Injury RehabilitationArko duttaNo ratings yet
- Subluxation and Dislocation of Ac JointDocument26 pagesSubluxation and Dislocation of Ac JointGan Quan FuNo ratings yet
- Trochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTrochanteric Bursitis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Physiotherapy TalkDocument23 pagesPhysiotherapy Talkphysiovipin100% (1)
- Biomechanics of The ElbowDocument16 pagesBiomechanics of The ElbowAsmaa Ahmad SharawyNo ratings yet
- Joint Mobilization To The Elbow, Wrist and Hand2Document43 pagesJoint Mobilization To The Elbow, Wrist and Hand2Tripty Khanna Karwal100% (1)
- Lumbar Disc HerniationDocument19 pagesLumbar Disc HerniationRabie'ahBahananNo ratings yet
- Lower Limb Orthosis Types and UsesDocument44 pagesLower Limb Orthosis Types and UsesRakesh shahNo ratings yet
- Subacrominal Impingement JNR PT EditedDocument38 pagesSubacrominal Impingement JNR PT EditedAndrew Foster100% (1)
- Design of A Hand OrthosisDocument251 pagesDesign of A Hand OrthosisIsrael BlancoNo ratings yet
- Walking AidsDocument38 pagesWalking AidsMurad KurdiNo ratings yet
- Chest Physiotherapy ProcedureDocument9 pagesChest Physiotherapy ProcedureLuqmanul HakimNo ratings yet
- Lec 3 Definition of PhysioDocument18 pagesLec 3 Definition of PhysioBhargav100% (1)
- HMP (Hot Moist Pack W. Fluido Therapy)Document17 pagesHMP (Hot Moist Pack W. Fluido Therapy)yamhtur_17100% (1)
- Low Back PainDocument8 pagesLow Back PainLev KalikaNo ratings yet
- Physiotherapy For Shoulder InjuriesDocument2 pagesPhysiotherapy For Shoulder InjuriesenadNo ratings yet
- Reducing Hypertonia in Stroke PatientsDocument3 pagesReducing Hypertonia in Stroke PatientsKhageswar SamalNo ratings yet
- CMP Exam 2015Document6 pagesCMP Exam 2015MansiNo ratings yet
- Clinical Biomechanics of Gait: OutlineDocument7 pagesClinical Biomechanics of Gait: Outlinechacho1971100% (1)
- Cervical PainDocument15 pagesCervical Painsteffiecruz06No ratings yet
- Rehab Advances for Spinal Cord InjuriesDocument45 pagesRehab Advances for Spinal Cord InjurieskaushikawebNo ratings yet
- Hip Joint Complex: Aneena Alex MPT Ist Year MtimsDocument38 pagesHip Joint Complex: Aneena Alex MPT Ist Year MtimsNaroashNo ratings yet
- Shoulder Dislocation Rehab ExerciseDocument5 pagesShoulder Dislocation Rehab ExerciseThar GyiNo ratings yet
- Computer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray ImagesDocument45 pagesComputer Aided Diagnosis System For Lumbar Spinal Stenosis Using X-Ray Imagesroky100% (1)
- Shoulder Dislocation DraftDocument26 pagesShoulder Dislocation Drafthusnajihah18No ratings yet
- GAIT 2 - Clinical Gait Analysis - HandoutDocument32 pagesGAIT 2 - Clinical Gait Analysis - Handoutj100% (1)
- Soft tissue injury treatmentDocument2 pagesSoft tissue injury treatmentThiruNo ratings yet
- Acute Anterior Shoulder Dislocation Physical Therapy ProtocolDocument4 pagesAcute Anterior Shoulder Dislocation Physical Therapy Protocolgermano87No ratings yet
- Disorders of The Spinal CordDocument9 pagesDisorders of The Spinal CordIsnawan WidyayantoNo ratings yet
- Adult Physiatric History and ExaminationDocument11 pagesAdult Physiatric History and Examinationsylschebe22gmailNo ratings yet
- Human Anatomy & PhysiologyDocument72 pagesHuman Anatomy & PhysiologyJoie UrsalNo ratings yet
- Biomechanics of The Shoulder ComplexDocument83 pagesBiomechanics of The Shoulder ComplexpiciliviNo ratings yet
- Hipbiomechanics 131109064817 Phpapp02Document37 pagesHipbiomechanics 131109064817 Phpapp02Arshad AliNo ratings yet
- The Wrist Complex: Vanita A Pathare PG-1Document54 pagesThe Wrist Complex: Vanita A Pathare PG-1vanita pathareNo ratings yet
- Acute Spinal Cord CompressionDocument13 pagesAcute Spinal Cord CompressionWhoNo ratings yet
- Co-Ordination: Prepared by Ahmed Shawky AliDocument59 pagesCo-Ordination: Prepared by Ahmed Shawky Alivenkata ramakrishnaiahNo ratings yet
- Overuse Knee InjuriesDocument4 pagesOveruse Knee InjuriesThe HomieNo ratings yet
- Anatomy and Pathoanatomic of Lumbosacral PlexusDocument33 pagesAnatomy and Pathoanatomic of Lumbosacral PlexusRachmad FaisalNo ratings yet
- Physiotherapy For Plantar Fasciitis - A UK Wide Survey of Current PracticeDocument29 pagesPhysiotherapy For Plantar Fasciitis - A UK Wide Survey of Current PracticeCambriaChicoNo ratings yet
- Orthopaedics PT AssessmentDocument9 pagesOrthopaedics PT AssessmentRajeev Tiwari100% (2)
- Physical therapists' role in fighting diabetes epidemicDocument24 pagesPhysical therapists' role in fighting diabetes epidemicdwi astutiNo ratings yet
- Kegel ExercisesDocument3 pagesKegel ExercisesfynneroNo ratings yet
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDocument172 pagesClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryNo ratings yet
- Walking Aids KinesiologyDocument26 pagesWalking Aids Kinesiologyfarwafurqan1No ratings yet
- Biomechanics of SpineDocument49 pagesBiomechanics of SpineDheerajJonnalagaddaNo ratings yet
- Notes For PTA NPTEFFDocument19 pagesNotes For PTA NPTEFFFarhana Rashena100% (1)
- IvdpDocument89 pagesIvdpFelix SabuNo ratings yet
- The Challenge of Managing Mid-Foot Pain: BackgroundDocument6 pagesThe Challenge of Managing Mid-Foot Pain: BackgroundIsha WuNo ratings yet
- What Is PolymyositisDocument24 pagesWhat Is PolymyositisAshraf MobyNo ratings yet
- Chest PhysiotherapyDocument2 pagesChest PhysiotherapyCarmela Dawn MarcoNo ratings yet
- Median Nerve Gliding Exercises ExplainedDocument2 pagesMedian Nerve Gliding Exercises ExplainedDavid PalashNo ratings yet
- Wrist Complex1Document25 pagesWrist Complex1bpt2100% (1)
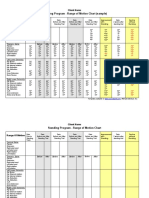
- Standing Program - Range of Motion Chart (Sample) : Client NameDocument2 pagesStanding Program - Range of Motion Chart (Sample) : Client NameNorMan Albaytar PerezNo ratings yet
- Bio Mechanic of Elbow JointDocument35 pagesBio Mechanic of Elbow Jointdeepuphysio100% (1)
- Thoracic Segment KpsDocument77 pagesThoracic Segment Kpskrishna bptNo ratings yet
- Low Back Pain Presentation IMPDocument114 pagesLow Back Pain Presentation IMPrapannika100% (3)
- Physiotheray Management of Shoulder DislocationDocument8 pagesPhysiotheray Management of Shoulder DislocationMonica StephenieNo ratings yet
- Anterior Shoulder InstabilityDocument19 pagesAnterior Shoulder InstabilitySiti Nur JannahNo ratings yet
- The Shoulder: Understanding The Science Behind Both Movement and Dysfunction by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMSDocument9 pagesThe Shoulder: Understanding The Science Behind Both Movement and Dysfunction by Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, AMSChrisGellertNo ratings yet
- Functional Assessment in Physiotherapy. A Literature Review: Europa Medicophysica January 2008Document18 pagesFunctional Assessment in Physiotherapy. A Literature Review: Europa Medicophysica January 2008Yeshvi sNo ratings yet
- PTJ Effect of Virtual Reality TrainingDocument14 pagesPTJ Effect of Virtual Reality TrainingYeshvi sNo ratings yet
- RGUHS IV Year B.P.T.April 2014Document5 pagesRGUHS IV Year B.P.T.April 2014Yeshvi sNo ratings yet
- Carcinoma Breast GuideDocument8 pagesCarcinoma Breast GuideYeshvi s100% (1)
- NEUROLOGY AND NEUROSURGERYDocument5 pagesNEUROLOGY AND NEUROSURGERYYeshvi sNo ratings yet
- Orthopedic Jayant JoshiDocument2,371 pagesOrthopedic Jayant JoshiYeshvi s86% (28)
- (Donna Frownfelter PT DPT MA CCS RRT FCCP, ElDocument827 pages(Donna Frownfelter PT DPT MA CCS RRT FCCP, ElJeffery Samuel89% (9)
- Physical Therapy Management of Rotator Cuff TearDocument8 pagesPhysical Therapy Management of Rotator Cuff TearYeshvi sNo ratings yet
- Australian Indigenous People - EditedDocument8 pagesAustralian Indigenous People - EditedApril CliffordNo ratings yet
- Nur - 100 Session 2 - SemillaDocument6 pagesNur - 100 Session 2 - SemillaVon R Semilla100% (1)
- History of Clinical PsychologyDocument2 pagesHistory of Clinical PsychologyAlfat MuizzNo ratings yet
- Liu 2017-Herbal Medicine For The Treatment of ObesityDocument17 pagesLiu 2017-Herbal Medicine For The Treatment of ObesityMas NuriNo ratings yet
- 678 FullDocument9 pages678 FullDarren WilliamNo ratings yet
- Case Study CLD 3Document18 pagesCase Study CLD 3MoonNo ratings yet
- Malmstrom Et Al - 1999 - Oral Montelukast, Inhaled Beclomethasone, and Placebo For Chronic AsthmaDocument10 pagesMalmstrom Et Al - 1999 - Oral Montelukast, Inhaled Beclomethasone, and Placebo For Chronic AsthmaRutvik ShahNo ratings yet
- Caie A2 Psychology 9990 Psychology and HealthDocument27 pagesCaie A2 Psychology 9990 Psychology and HealthAhmad Magdi Abdel-AzizNo ratings yet
- Cliques in Cms High Schools and The Consequences Final PaperDocument8 pagesCliques in Cms High Schools and The Consequences Final Paperapi-441877801No ratings yet
- FinalDocument66 pagesFinalRakshith gowdaNo ratings yet
- Chronic Inflammation Post Head InjuryDocument15 pagesChronic Inflammation Post Head InjuryErwin SumardiNo ratings yet
- The God Within - BM HegdeDocument2 pagesThe God Within - BM HegdeSini AdvNo ratings yet
- SM Lazo Medical Clinic PEME Schedule ConfirmationDocument1 pageSM Lazo Medical Clinic PEME Schedule ConfirmationMaximoNo ratings yet
- Q and AnswersDocument20 pagesQ and AnswersnehamyaNo ratings yet
- Final Oral Pathology ExamDocument5 pagesFinal Oral Pathology Examsolom islamNo ratings yet
- Approved - BSN332 Mental Health Nursing - Clinical WorkbookDocument8 pagesApproved - BSN332 Mental Health Nursing - Clinical WorkbookNada NasserNo ratings yet
- FULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF Ebookjennifer.lawver532100% (42)
- Dental Deposits: Biofilm, Calculus and Stain GuideDocument45 pagesDental Deposits: Biofilm, Calculus and Stain GuideAngie SwearingenNo ratings yet
- ImmunizationDocument30 pagesImmunizationAhmed Ali100% (1)
- Different Organs of The BodyDocument2 pagesDifferent Organs of The BodyVon Ramwel NicolasNo ratings yet
- Typhoid DiseaseDocument28 pagesTyphoid DiseaseSaba Parvin Haque100% (1)
- ANATOMY, BLOOD SUPPLY AND LYMPHATIC DRAINAGE OF THE BREASTDocument62 pagesANATOMY, BLOOD SUPPLY AND LYMPHATIC DRAINAGE OF THE BREASThussain AltaherNo ratings yet
- DAST-10 Institute PDFDocument1 pageDAST-10 Institute PDFImran KhanNo ratings yet
- J of Obstet and Gynaecol - 2021 - Demirdag - Subsequent IVF Outcomes Following Antibiotic Therapy For Chronic EndometritisDocument7 pagesJ of Obstet and Gynaecol - 2021 - Demirdag - Subsequent IVF Outcomes Following Antibiotic Therapy For Chronic EndometritisQui Nguyen MinhNo ratings yet
- Demetrio L. Valle JR., MD, MSC., FPSP, Fascp, Ifcap Anatomic and Clinical PathologistDocument26 pagesDemetrio L. Valle JR., MD, MSC., FPSP, Fascp, Ifcap Anatomic and Clinical Pathologistodin3zNo ratings yet
- Principle:: Sample Considerations and Special ProceduresDocument97 pagesPrinciple:: Sample Considerations and Special Proceduresjustine anchetaNo ratings yet
- Enzyme Brochure Gen Chem PTDocument2 pagesEnzyme Brochure Gen Chem PTAdrielNo ratings yet
- Design Considerations in RPD For Control of StressDocument7 pagesDesign Considerations in RPD For Control of StressSahana RangarajanNo ratings yet
- Recommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseDocument34 pagesRecommended Procedures For Doctors and Nurse in The Management of Kawasaki DiseaseJOSHUA DICHOSONo ratings yet
- Body temperature monitoring sheetDocument1 pageBody temperature monitoring sheetChandru CkNo ratings yet