You might also like
- A Comparative Study of Mechanical Properties of Zinc Acrylate Epoxy nanocomposites Reinforced by AL2O3 and Cloisite®30B and Their Mixture: Tensile Strength and Fracture Toughness: A Comparative Study of Mechanical Properties of Zinc Acrylate Epoxy nanocomposites Reinforced by AL2O3 and Cloisite®30B and Their Mixture: Tensile Strength and Fracture ToughnessFrom EverandA Comparative Study of Mechanical Properties of Zinc Acrylate Epoxy nanocomposites Reinforced by AL2O3 and Cloisite®30B and Their Mixture: Tensile Strength and Fracture Toughness: A Comparative Study of Mechanical Properties of Zinc Acrylate Epoxy nanocomposites Reinforced by AL2O3 and Cloisite®30B and Their Mixture: Tensile Strength and Fracture ToughnessNo ratings yet
- Heat Treatment Boosts Bond Strength and Conversion of Indirect CompositesDocument9 pagesHeat Treatment Boosts Bond Strength and Conversion of Indirect CompositesKenigal14No ratings yet
- Brunengo 2020Document13 pagesBrunengo 2020abdhossain46No ratings yet
- Sae Technical Paper Series: M.-T. Ton-That, J. Denault and K. C. ColeDocument6 pagesSae Technical Paper Series: M.-T. Ton-That, J. Denault and K. C. ColeSagar MehtaNo ratings yet
- Degree of Conversion of Three Composite PDFDocument6 pagesDegree of Conversion of Three Composite PDFFreddy GarciaNo ratings yet
- 2011 The - Impact - of - in - Vitro - Aging - On - The - MechDocument13 pages2011 The - Impact - of - in - Vitro - Aging - On - The - MechGeorgi AnaNo ratings yet
- TMP BBEADocument7 pagesTMP BBEAFrontiersNo ratings yet
- EVA Mujalrosas2011Document12 pagesEVA Mujalrosas2011Anonymous mYTaxRNo ratings yet
- Jongprateep 2015Document6 pagesJongprateep 2015kamran ullahNo ratings yet
- Polymerization Lamps and Photocuring in OrthodonticsDocument8 pagesPolymerization Lamps and Photocuring in Orthodonticsgriffone1No ratings yet
- Resin Composite Blocks Via High-Pressure High-Temperature PolymerizationDocument6 pagesResin Composite Blocks Via High-Pressure High-Temperature PolymerizationWilver MuñozNo ratings yet
- Research Article: Effect of Thermocycling, Teeth, and Polymerization Methods On Bond Strength Teeth-Denture BaseDocument6 pagesResearch Article: Effect of Thermocycling, Teeth, and Polymerization Methods On Bond Strength Teeth-Denture BaseShreyans DamadeNo ratings yet
- Repair Potential of A Laboratory-Processed Nano-Hybrid Resin CompositeDocument10 pagesRepair Potential of A Laboratory-Processed Nano-Hybrid Resin CompositeGusti Gina Permata SariNo ratings yet
- Electrodeposition of Nanostructured Bioactive Hydroxyapatite-Heparin Composite Coatings On Titanium For Dental Implant ApplicationsDocument10 pagesElectrodeposition of Nanostructured Bioactive Hydroxyapatite-Heparin Composite Coatings On Titanium For Dental Implant ApplicationsWahyu Ginanjar ArgianNo ratings yet
- Alumina Particle size-KPMDocument7 pagesAlumina Particle size-KPMrajeshayrNo ratings yet
- Influence of Softening Test and Light Activation Protocols On Resin Composite Polymer StructureDocument6 pagesInfluence of Softening Test and Light Activation Protocols On Resin Composite Polymer StructureAini Dwi HandiniNo ratings yet
- Influence of Curing Time, Overlay Material and Thickness On Three Light-Curing Composites Used For Luting Indirect Composite RestorationsDocument8 pagesInfluence of Curing Time, Overlay Material and Thickness On Three Light-Curing Composites Used For Luting Indirect Composite RestorationsAbhishek Isaac MathewNo ratings yet
- Resin CompoitesDocument7 pagesResin CompoitesShabia AzharNo ratings yet
- Resin - Resin Bonding - A New Adhesive - TechnologyDocument10 pagesResin - Resin Bonding - A New Adhesive - TechnologyComarzzoNo ratings yet
- Postes de Fibra de VidrioDocument9 pagesPostes de Fibra de VidrioNatan CastilloNo ratings yet
- Polymerization Shrinkage of Five Bulk-Fill Composite Resins in Comparison With A Conventional Composite ResinDocument10 pagesPolymerization Shrinkage of Five Bulk-Fill Composite Resins in Comparison With A Conventional Composite Resinadriana llanesNo ratings yet
- Simple and Low Coast ThermalDocument6 pagesSimple and Low Coast ThermalEDWIN MILER REISHTATTER REISHTATTERNo ratings yet
- Komposisi z350Document9 pagesKomposisi z350muchlis fauziNo ratings yet
- J Mat Sci 2011, 46, 6508 Efecto de La Organoarcilla Con Diferentes Modificadores Organicos en Las Propiedades TermoplasticasDocument10 pagesJ Mat Sci 2011, 46, 6508 Efecto de La Organoarcilla Con Diferentes Modificadores Organicos en Las Propiedades TermoplasticasDavid ContrerasNo ratings yet
- 2019 Polimerizacion Adecuada de Las BulkDocument7 pages2019 Polimerizacion Adecuada de Las BulkOskar OrtizNo ratings yet
- Mechanical properties and curing of short fiber-reinforced resin compositesDocument7 pagesMechanical properties and curing of short fiber-reinforced resin compositesPaul AlvarezNo ratings yet
- Mechanical Properties of Unsaturated Polyester Resin: International Journal of Chemtech Research October 2010Document6 pagesMechanical Properties of Unsaturated Polyester Resin: International Journal of Chemtech Research October 2010dhikaNo ratings yet
- 1678 7757 Jaos 17 04 0289Document5 pages1678 7757 Jaos 17 04 0289Percy Andree Bayona GuillermoNo ratings yet
- A.DORIGATO (2013) - Filler Aggregation As A Stiffening Mechanism in Polymer NanocompositesDocument43 pagesA.DORIGATO (2013) - Filler Aggregation As A Stiffening Mechanism in Polymer NanocompositesALDO CORDOBA GUERRERONo ratings yet
- Supervision of Ethylene Propylene Diene M-Class (EPDM) Rubber Vulcanization and Recovery Processes Using Attenuated Total Reflection Fourier Transform Infrared (ATR FT-IR) Spectroscopy and Multivariate AnalysisDocument12 pagesSupervision of Ethylene Propylene Diene M-Class (EPDM) Rubber Vulcanization and Recovery Processes Using Attenuated Total Reflection Fourier Transform Infrared (ATR FT-IR) Spectroscopy and Multivariate AnalysisFairmont Ind Quality DivisionNo ratings yet
- Saade 2010Document6 pagesSaade 2010johnNo ratings yet
- Materials 05 02960 PDFDocument21 pagesMaterials 05 02960 PDFNabihah AbdullahNo ratings yet
- Polymers-And PeekDocument13 pagesPolymers-And PeekmustafaNo ratings yet
- Indirect Resin CompositesDocument12 pagesIndirect Resin CompositesJavier Istúriz Sijot100% (1)
- Effect of Lithium Disilicate Veneers of Different Thickness On The Degree of Conversion and Microhardness of A Light-Curing and A Dual-Curing Cement.Document5 pagesEffect of Lithium Disilicate Veneers of Different Thickness On The Degree of Conversion and Microhardness of A Light-Curing and A Dual-Curing Cement.Danny Eduardo RomeroNo ratings yet
- Effect of Cervical Margin Relocation on Marginal Quality of CAD/CAM CrownsDocument8 pagesEffect of Cervical Margin Relocation on Marginal Quality of CAD/CAM CrownsIvy MedNo ratings yet
- Dewaele M. 2009 Dent. Mater. Influence of Curing Protocol On Selected Properties of Light Curing Polymers Degree of Conversion, Volume Contraction, Elastic Modulus, and Glass Transition TemperatureDocument9 pagesDewaele M. 2009 Dent. Mater. Influence of Curing Protocol On Selected Properties of Light Curing Polymers Degree of Conversion, Volume Contraction, Elastic Modulus, and Glass Transition TemperatureLilyan YamasakiNo ratings yet
- 1757 899x2F1/012040Document8 pages1757 899x2F1/012040SahasraNo ratings yet
- Modification of Dielectric Properties, After Barium Titanate Nanoparticles Sintering, From A Thermoplastic Polymer MatrixDocument6 pagesModification of Dielectric Properties, After Barium Titanate Nanoparticles Sintering, From A Thermoplastic Polymer MatrixScarlatache VladNo ratings yet
- Fabrication and Characterization of Tio - Epoxy NanocompositeDocument12 pagesFabrication and Characterization of Tio - Epoxy Nanocompositesur22as.aswarNo ratings yet
- Biodegradation and Abrasive Wear of Nano Restorative MaterialsDocument8 pagesBiodegradation and Abrasive Wear of Nano Restorative MaterialsLuana Silva RuizNo ratings yet
- Lab-Processed Resin Composites CharacterizationDocument7 pagesLab-Processed Resin Composites CharacterizationGeorgi AnaNo ratings yet
- Effect of Wollastonite and Talc On The Micromechanisms of Tensile Deformation in Polypropylene CompositesDocument20 pagesEffect of Wollastonite and Talc On The Micromechanisms of Tensile Deformation in Polypropylene CompositesOmarNo ratings yet
- 2010 FortunatiDocument7 pages2010 Fortunatijoan manuel MolinaNo ratings yet
- Thermo-Mechanical Chain Branching of Commercial High Density Polyethylene During ExtrusionDocument9 pagesThermo-Mechanical Chain Branching of Commercial High Density Polyethylene During ExtrusionRimaz RameezNo ratings yet
- The Effect of Different CompatibilizersDocument14 pagesThe Effect of Different CompatibilizersWellington C. de AraujoNo ratings yet
- Fracture toughness and wear resistance of indirect compositesDocument3 pagesFracture toughness and wear resistance of indirect compositesjarjar bin binxNo ratings yet
- San Thermal PropertiespdfDocument7 pagesSan Thermal Propertiespdfsukhabhukha987No ratings yet
- Effect of ZrO2-Al2O3 on Acrylic Resin PropertiesDocument7 pagesEffect of ZrO2-Al2O3 on Acrylic Resin PropertiesbrilianenoNo ratings yet
- Uretan Dimetacrilat Monomer PDFDocument12 pagesUretan Dimetacrilat Monomer PDFMirela ValeNo ratings yet
- Materials and DesignDocument10 pagesMaterials and Designsur22as.aswarNo ratings yet
- Boccardi 2015Document5 pagesBoccardi 2015Yuzar StuffNo ratings yet
- Mechanical and Biocompatible Properties of Polymer-Infiltrated-Ceramic-Network Materials For Dental RestorationDocument6 pagesMechanical and Biocompatible Properties of Polymer-Infiltrated-Ceramic-Network Materials For Dental RestorationAna-Marya RadionNo ratings yet
- Comparative Study Regarding Friction Coefficient For Three Epoxy ResinsDocument5 pagesComparative Study Regarding Friction Coefficient For Three Epoxy ResinsEdgar Arturo Gomez MeiselNo ratings yet
- Materials Science and Engineering ADocument10 pagesMaterials Science and Engineering ARushyanth KRNo ratings yet
- TMP ED08Document11 pagesTMP ED08FrontiersNo ratings yet
- Fan 2016Document25 pagesFan 2016Tejas krishnakanthNo ratings yet
- Fracture Load and Failure Types of Different Veneered Polyetheretherketone Fixed Dental ProsthesesDocument8 pagesFracture Load and Failure Types of Different Veneered Polyetheretherketone Fixed Dental ProsthesesNelson BarakatNo ratings yet
- Bonding Agents Improve Quality of Composite RepairDocument7 pagesBonding Agents Improve Quality of Composite RepairSaad LiaqatNo ratings yet
- Dynamic Mechanical and Thermal Properties of Clear Aligners After Thermoforming and AgingDocument11 pagesDynamic Mechanical and Thermal Properties of Clear Aligners After Thermoforming and AgingJ KabaniNo ratings yet
- Polymerization and Light Curing Units in Restorative DentistryDocument29 pagesPolymerization and Light Curing Units in Restorative DentistryKenny Rafael Iglesias AlvarezNo ratings yet
- Influence of Photoinitiator and Light-Curing SourcDocument7 pagesInfluence of Photoinitiator and Light-Curing SourcKenny Rafael Iglesias AlvarezNo ratings yet
- Current OptionsDocument12 pagesCurrent OptionsManuNo ratings yet
- 10 1016@j Dental 2009 11 149Document14 pages10 1016@j Dental 2009 11 149Kenny Rafael Iglesias AlvarezNo ratings yet
- Wang 2017Document27 pagesWang 2017Kenny Rafael Iglesias AlvarezNo ratings yet
- Old Wine in New Bottle PDFDocument12 pagesOld Wine in New Bottle PDFMariaNo ratings yet
- Improvement of Total Etching Dentin Bonding With SubpressureDocument9 pagesImprovement of Total Etching Dentin Bonding With SubpressureKenny Rafael Iglesias AlvarezNo ratings yet
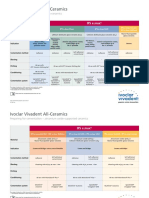
- Ivoclar Cementation GuidelinesDocument2 pagesIvoclar Cementation GuidelinesKenny Rafael Iglesias AlvarezNo ratings yet
- 03 All-Ceramic Cementation 2009-E Feb09-2 PDFDocument2 pages03 All-Ceramic Cementation 2009-E Feb09-2 PDFNaomi Uehara UyedaNo ratings yet
- Draw Lewis Structures EasilyDocument3 pagesDraw Lewis Structures EasilyclrgeekNo ratings yet
- Articulo 1 Inmovilización Alginato PDFDocument6 pagesArticulo 1 Inmovilización Alginato PDFCarolina MorenoNo ratings yet
- OxoneDocument2 pagesOxoneSha Hriyar HNo ratings yet
- Project ProposalDocument2 pagesProject ProposalHaries GarciaNo ratings yet
- Chemical Equations ExplainedDocument91 pagesChemical Equations ExplainedHenryco TibaNo ratings yet
- Colateric Cdcx-50 and CDCX-LVDocument2 pagesColateric Cdcx-50 and CDCX-LVmndmattNo ratings yet
- - (Appendix B Lennard–Jones Constants) PDFDocument2 pages- (Appendix B Lennard–Jones Constants) PDFYaiselle FelicianoNo ratings yet
- Worksheet ElectroChemistry-2Document2 pagesWorksheet ElectroChemistry-2Rishi ChatterjeeNo ratings yet
- Grevillea RobustaDocument6 pagesGrevillea RobustaJeyabalaganesh GNo ratings yet
- Study On Manures and FertilizersDocument7 pagesStudy On Manures and Fertilizersgenerlacc21No ratings yet
- Langridge Pigment RRPDocument5 pagesLangridge Pigment RRPstlukeartNo ratings yet
- BROC Mackam Dab en v1.0Document2 pagesBROC Mackam Dab en v1.0jangri1098No ratings yet
- Mole Concept PDF, Super 3000 BatchDocument29 pagesMole Concept PDF, Super 3000 BatchKaran RathodNo ratings yet
- Manual IiDocument80 pagesManual Iijast1111No ratings yet
- DDC SVC Bro 0001 - 2018Document39 pagesDDC SVC Bro 0001 - 2018David PomaNo ratings yet
- MethanolDocument1 pageMethanolRiyadi HendraNo ratings yet
- Taisox 8001Document2 pagesTaisox 8001Le Minh TuanNo ratings yet
- CS230 Consumables & Spare PartsDocument2 pagesCS230 Consumables & Spare PartsMark FieldsNo ratings yet
- Ultramarine: Ultramarine Is A Deep Blue Color Pigment Which Was OriginallyDocument11 pagesUltramarine: Ultramarine Is A Deep Blue Color Pigment Which Was Originallyengineer bilalNo ratings yet
- Course: Chemical Process Technology Lecture - 7 Topic: Pesticides Industries Course Code: SECH3071Document10 pagesCourse: Chemical Process Technology Lecture - 7 Topic: Pesticides Industries Course Code: SECH3071rutvikNo ratings yet
- Preview-9781316675496 A27454940Document121 pagesPreview-9781316675496 A27454940HendrijosphNo ratings yet
- Combined PH WorksheetsDocument9 pagesCombined PH WorksheetsNeen NaazNo ratings yet
- PPL 43Document242 pagesPPL 43Divesh GuptaNo ratings yet
- Presperse Catalog - Europe Asia 12-2011 PDFDocument13 pagesPresperse Catalog - Europe Asia 12-2011 PDFponian9338No ratings yet
- Influence of Alloying Conditions On The Properties of White Cast IronDocument6 pagesInfluence of Alloying Conditions On The Properties of White Cast IronSarvar TursunbaevNo ratings yet
- Properties of Palm Ash Concrete: P.Premalatha, K.R.Vinodh, L.Chris Anto, R.NithiyaDocument4 pagesProperties of Palm Ash Concrete: P.Premalatha, K.R.Vinodh, L.Chris Anto, R.NithiyainventionjournalsNo ratings yet
- Synthesis Paper Title: BiofuelsDocument24 pagesSynthesis Paper Title: Biofuelspati_deeps234No ratings yet
- Iso 4997Document19 pagesIso 4997Aravind BabuNo ratings yet
- Quantitative Determination of WaterDocument23 pagesQuantitative Determination of WaterApurba Sarker Apu100% (1)
- 03 Specification PDFDocument8 pages03 Specification PDFSihamaSihamNo ratings yet