You might also like
- Coping, Stress, and Negative Childhood Experiences The Link To Psychopathology, Self-Harm, and Suicidal BehaviorDocument14 pagesCoping, Stress, and Negative Childhood Experiences The Link To Psychopathology, Self-Harm, and Suicidal BehaviorDini indrianyNo ratings yet
- Sample Final Exam Larkin AnswersDocument18 pagesSample Final Exam Larkin AnswersLovejot SinghNo ratings yet
- Week 1-12 strength and conditioning programDocument6 pagesWeek 1-12 strength and conditioning programBrian Michael CarrollNo ratings yet
- Separation Anxiety PDFDocument27 pagesSeparation Anxiety PDFDiego M LisNo ratings yet
- 10.1 PP 3 27 Phenomenology and Standard Evidence-Based Care of Anxiety Disorders in Children and AdolescentsDocument25 pages10.1 PP 3 27 Phenomenology and Standard Evidence-Based Care of Anxiety Disorders in Children and AdolescentsMarinaNo ratings yet
- Anxiety in ChildrenDocument18 pagesAnxiety in ChildrenquinhoxNo ratings yet
- Anxiety DisordersDocument12 pagesAnxiety DisordersRosy O. Hing-ngitNo ratings yet
- Neuroanatomia Funcional Machado 3 Ed 2014Document34 pagesNeuroanatomia Funcional Machado 3 Ed 2014ThiagoSoaresNo ratings yet
- Tratamiento de Fobia A Tragar: Estudio de Un Caso: January 2002Document13 pagesTratamiento de Fobia A Tragar: Estudio de Un Caso: January 2002AngelaNo ratings yet
- Vasey 2014Document18 pagesVasey 2014ABDUL FAQIMANNo ratings yet
- Clinical Features of Young Children Referred For Impairing Temper OutburstsDocument9 pagesClinical Features of Young Children Referred For Impairing Temper OutburstsRafael MartinsNo ratings yet
- transtornos del apegoDocument8 pagestranstornos del apegojamidfNo ratings yet
- Autonomic Arousal in Children of Parents With and Withou Social AnxietyDocument10 pagesAutonomic Arousal in Children of Parents With and Withou Social AnxietyNASC8No ratings yet
- Assessing and Treating Pediatric Anxiety DisordersDocument19 pagesAssessing and Treating Pediatric Anxiety Disordersayub01No ratings yet
- Fears and Phobias in Children: Phenomenology, Epidemiology, and AetiologyDocument10 pagesFears and Phobias in Children: Phenomenology, Epidemiology, and Aetiologykarin24No ratings yet
- NIH Public Access: Author ManuscriptDocument19 pagesNIH Public Access: Author ManuscriptYeremias EdwinNo ratings yet
- Childhood Separation Anxiety and Separation Events in Women With Agoraphobia With or Without Panic DisorderDocument4 pagesChildhood Separation Anxiety and Separation Events in Women With Agoraphobia With or Without Panic DisorderFabianNo ratings yet
- Facial Emotion Expression Recognition by Children at Familial Risk For DepressionDocument11 pagesFacial Emotion Expression Recognition by Children at Familial Risk For DepressionHuda ZainiNo ratings yet
- Final Draft Research Paper 2Document8 pagesFinal Draft Research Paper 2api-610037275No ratings yet
- UntitledDocument9 pagesUntitledMeghna PatraNo ratings yet
- Childhood Separation Anxiety and The Pathogenesis and Treatment of Adult AnxietyDocument10 pagesChildhood Separation Anxiety and The Pathogenesis and Treatment of Adult AnxietyyesumovsNo ratings yet
- Dismissing Child Attachment and Discordance For Subjective and Neuroendocrine Responses To VulnerabilityDocument8 pagesDismissing Child Attachment and Discordance For Subjective and Neuroendocrine Responses To VulnerabilitySupra ManNo ratings yet
- Lavalee, 2011Document8 pagesLavalee, 2011Pablo Padilla SolanoNo ratings yet
- Panic Attack Symptomatology and Anxiety Sensitivity in AdolescentsDocument10 pagesPanic Attack Symptomatology and Anxiety Sensitivity in AdolescentsBálint KapturNo ratings yet
- Developmental and Clinical Predictors of Comorbidity For Youth With OCDDocument7 pagesDevelopmental and Clinical Predictors of Comorbidity For Youth With OCDViktória Papucsek LelkesNo ratings yet
- Attachment and Psychosomatic Medicine: Developmental Contributions To Stress and DiseaseDocument12 pagesAttachment and Psychosomatic Medicine: Developmental Contributions To Stress and DiseaseJFFNo ratings yet
- Somatic Symptoms in Children and Adolescents With Anxiety DisordersDocument9 pagesSomatic Symptoms in Children and Adolescents With Anxiety DisordersDũng HồNo ratings yet
- Artículo Tema 4 Tratamiento para La Depresión en Niños y PreescolaresDocument5 pagesArtículo Tema 4 Tratamiento para La Depresión en Niños y PreescolaresMariaAn DominguezNo ratings yet
- En V80n2sa05Document7 pagesEn V80n2sa05Imtiaz KhanNo ratings yet
- 16 de Septiembre ArticuloDocument12 pages16 de Septiembre ArticuloLina María MoncadaNo ratings yet
- TCC para Niños Con Síntomas DepresivosDocument15 pagesTCC para Niños Con Síntomas DepresivosKevin CaperaNo ratings yet
- Links Between Childhood Experiences andDocument16 pagesLinks Between Childhood Experiences andgica.bucicNo ratings yet
- Battaglia 2016 Id 5357 PDFDocument8 pagesBattaglia 2016 Id 5357 PDFLucia ButcovanNo ratings yet
- Fear of Speaking: Chronic Anxiety and Stammering: Ashley Craig & Yvonne TranDocument6 pagesFear of Speaking: Chronic Anxiety and Stammering: Ashley Craig & Yvonne TrannigoNo ratings yet
- Mendle 2014 Child Development PerspectivesDocument5 pagesMendle 2014 Child Development PerspectivesChristeeba F MNo ratings yet
- Early Stages in The Development of Bipolar Disorder - 2010Document9 pagesEarly Stages in The Development of Bipolar Disorder - 2010cesia leivaNo ratings yet
- Anxiety in Adolescents With Asperger Syndrome: Negative Thoughts, Behavioral Problems, and Life InterferenceDocument12 pagesAnxiety in Adolescents With Asperger Syndrome: Negative Thoughts, Behavioral Problems, and Life InterferenceHerdiko ShalatinNo ratings yet
- HHS Public Access: A Longitudinal Study of Fathers' and Young Children's Depressive SymptomsDocument25 pagesHHS Public Access: A Longitudinal Study of Fathers' and Young Children's Depressive SymptomsPawan MishraNo ratings yet
- Attachment Theory in Adolescence and AdulthoodDocument6 pagesAttachment Theory in Adolescence and AdulthoodsimuNo ratings yet
- შფოთვაDocument13 pagesშფოთვაNatia ChochuaNo ratings yet
- OCD in Children and Adolescents: Causes, Symptoms, and TreatmentsDocument10 pagesOCD in Children and Adolescents: Causes, Symptoms, and TreatmentsFaris Aziz PridiantoNo ratings yet
- Pablo PadillaDocument7 pagesPablo PadillaPablo Padilla SolanoNo ratings yet
- CentreforMentalHealth MissedOpportunitiesDocument120 pagesCentreforMentalHealth MissedOpportunitiesMahmood ArafatNo ratings yet
- Children Who Are Anxious in Silent - A Review of Selective MutismDocument19 pagesChildren Who Are Anxious in Silent - A Review of Selective MutismNicole WilliamsNo ratings yet
- Egger Angold 2006emot Behav Problems in PreschoolerDocument25 pagesEgger Angold 2006emot Behav Problems in PreschoolerccarmogarciaNo ratings yet
- Aust N Z J Psychiatry 2013 Marnane 12 5Document5 pagesAust N Z J Psychiatry 2013 Marnane 12 5KThreopusNo ratings yet
- Schizophrenia Research: Felipe V. Gomes, Xiyu Zhu, Anthony A. GraceDocument7 pagesSchizophrenia Research: Felipe V. Gomes, Xiyu Zhu, Anthony A. GraceAntu ChumpitazNo ratings yet
- Empirically Supported Treatments For Children With Phobic and Anxiety Disorders Current StatusDocument13 pagesEmpirically Supported Treatments For Children With Phobic and Anxiety Disorders Current StatusJust a GirlNo ratings yet
- Brumariu y Kerns, 2010Document28 pagesBrumariu y Kerns, 2010DeniseNo ratings yet
- Separation Anxiety ResearchDocument7 pagesSeparation Anxiety ResearchMary Rose HaglerNo ratings yet
- Somatic Complaints and Symptoms of AnxieDocument18 pagesSomatic Complaints and Symptoms of AnxieSalomon Verhelst MontenegroNo ratings yet
- Estimating The Impact of Transmitted and Non-Transmitted Psychiatric and Neurodevelopmental Polygenic Scores On Youth Emotional ProblemsDocument10 pagesEstimating The Impact of Transmitted and Non-Transmitted Psychiatric and Neurodevelopmental Polygenic Scores On Youth Emotional Problemssherifgamea911No ratings yet
- Representations of The Caregiver-Child Relationship and of The Self, and Emotion Regulation in The Narratives of Young Children Whose Mothers Have BPDDocument20 pagesRepresentations of The Caregiver-Child Relationship and of The Self, and Emotion Regulation in The Narratives of Young Children Whose Mothers Have BPDme13No ratings yet
- Current Trends in The Understanding and Treatment of Social Phobia inDocument14 pagesCurrent Trends in The Understanding and Treatment of Social Phobia inDenise Nuñez0% (1)
- Journal of A Ffective Disorders: Julia C. Poole, Keith S. Dobson, Dennis PuschDocument9 pagesJournal of A Ffective Disorders: Julia C. Poole, Keith S. Dobson, Dennis PuschArouetNo ratings yet
- Anxiety and Depression Are Risk Factors Rather Than Consequences of Functional Somatic Symptoms in A General Population of Adolescents - The TRAILS StudyDocument9 pagesAnxiety and Depression Are Risk Factors Rather Than Consequences of Functional Somatic Symptoms in A General Population of Adolescents - The TRAILS StudyJPCP 2014No ratings yet
- Journal of Anxiety Disorders: Ann E. Layne, Debra H. Bernat, Andrea M. Victor, Gail A. BernsteinDocument7 pagesJournal of Anxiety Disorders: Ann E. Layne, Debra H. Bernat, Andrea M. Victor, Gail A. BernsteinMelina Defita SariNo ratings yet
- The Etiology of Social Anxiety Disorder - An Evidence-Based ModelDocument3 pagesThe Etiology of Social Anxiety Disorder - An Evidence-Based ModelEvy Sulfiani KomalaNo ratings yet
- Pediatric AnxietyDocument26 pagesPediatric AnxietyYunisa astiaraniNo ratings yet
- Behavioural, Emotional and Social Development of Children Who StutterDocument10 pagesBehavioural, Emotional and Social Development of Children Who StutterMagaliNo ratings yet
- Psychological assessment in pediatric rehabilitationDocument27 pagesPsychological assessment in pediatric rehabilitationRicardo BulnesNo ratings yet
- Hunger: Mentalization-based Treatments for Eating DisordersFrom EverandHunger: Mentalization-based Treatments for Eating DisordersRating: 1 out of 5 stars1/5 (1)
- Applicationofimaging Technologiesinthe InvestigationofdrugaddictionDocument16 pagesApplicationofimaging Technologiesinthe Investigationofdrugaddictionstein godoy pachecoNo ratings yet
- Marijuana: Billyr - Martin Williaml - Dewey VincenzodimarzoDocument14 pagesMarijuana: Billyr - Martin Williaml - Dewey Vincenzodimarzostein godoy pachecoNo ratings yet
- Currentandexperimental Therapeuticsforthe TreatmentofopioidaddictionDocument12 pagesCurrentandexperimental Therapeuticsforthe Treatmentofopioidaddictionstein godoy pachecoNo ratings yet
- Physiology of WDDocument16 pagesPhysiology of WDphungoNo ratings yet
- C102 1461-1474 PDFDocument14 pagesC102 1461-1474 PDFstein godoy pachecoNo ratings yet
- Currentandexperimental TherapeuticsofinsomniaDocument14 pagesCurrentandexperimental Therapeuticsofinsomniastein godoy pachecoNo ratings yet
- C134 1945-1960 PDFDocument16 pagesC134 1945-1960 PDFstein godoy pachecoNo ratings yet
- Basicmechanismsofsedative/ Hypnotics: Theories of Hypnotic ActionDocument8 pagesBasicmechanismsofsedative/ Hypnotics: Theories of Hypnotic Actionstein godoy pachecoNo ratings yet
- C134 1945-1960 PDFDocument16 pagesC134 1945-1960 PDFstein godoy pachecoNo ratings yet
- SUBSTANCE USE DISORDERSDocument2 pagesSUBSTANCE USE DISORDERSAbhishek KaushikNo ratings yet
- Basicmechanismsofsedative/ Hypnotics: Theories of Hypnotic ActionDocument8 pagesBasicmechanismsofsedative/ Hypnotics: Theories of Hypnotic Actionstein godoy pachecoNo ratings yet
- Currentandexperimental TherapeuticsofinsomniaDocument14 pagesCurrentandexperimental Therapeuticsofinsomniastein godoy pachecoNo ratings yet
- Movementdisordersand Proxysmaldisorders: Carola - TammingaDocument2 pagesMovementdisordersand Proxysmaldisorders: Carola - Tammingastein godoy pachecoNo ratings yet
- Chronobiologyandsleep Disorders: S E C T I O NDocument2 pagesChronobiologyandsleep Disorders: S E C T I O Nstein godoy pachecoNo ratings yet
- Impulsiveandcompulsive Disorders: Tion of Progress Is Unique in Including A Section On ImpulsiveDocument2 pagesImpulsiveandcompulsive Disorders: Tion of Progress Is Unique in Including A Section On Impulsivestein godoy pachecoNo ratings yet
- 2017 Essential Medicines List Published: Read MoreDocument2 pages2017 Essential Medicines List Published: Read Morestein godoy pachecoNo ratings yet
- Herbivoría y Cristales de CaOxDocument33 pagesHerbivoría y Cristales de CaOxBrain LongwoodNo ratings yet
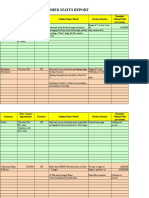
- Customer Status Update Report 27th January 2015 ColourDocument20 pagesCustomer Status Update Report 27th January 2015 ColourmaryNo ratings yet
- A Lesson Plan in English by Laurence MercadoDocument7 pagesA Lesson Plan in English by Laurence Mercadoapi-251199697No ratings yet
- Who Are The Pleiadian Emissaries of LightDocument3 pagesWho Are The Pleiadian Emissaries of LightMichelle88% (8)
- Knowledge, Attitudes and Practices of Nursing Students on Dengue FeverDocument9 pagesKnowledge, Attitudes and Practices of Nursing Students on Dengue FeverElinNo ratings yet
- ResearchDocument44 pagesResearchGwend MemoracionNo ratings yet
- Tulsi Ka Kavya Aur Samanvay Ki ChestaDocument6 pagesTulsi Ka Kavya Aur Samanvay Ki Chestaaman singhNo ratings yet
- 4147ictte384 PDFDocument6 pages4147ictte384 PDFKandasamy AsohanNo ratings yet
- The Principles Taj MahalDocument2 pagesThe Principles Taj MahalVishnuMohanNo ratings yet
- UT Dallas Syllabus For Se2370.501 05s Taught by Weichen Wong (Wew021000)Document1 pageUT Dallas Syllabus For Se2370.501 05s Taught by Weichen Wong (Wew021000)UT Dallas Provost's Technology GroupNo ratings yet
- Drewry Capability StatementDocument9 pagesDrewry Capability Statementmanis_sgsNo ratings yet
- Perspective Homework RubricDocument2 pagesPerspective Homework Rubricapi-244578825No ratings yet
- Ken Jennings' Junior Genius Guides: Maps and Geography (Excerpt)Document24 pagesKen Jennings' Junior Genius Guides: Maps and Geography (Excerpt)Simon and Schuster100% (2)
- Class of 2016 Graduate ListsDocument16 pagesClass of 2016 Graduate ListscallertimesNo ratings yet
- CSCP Module 3Document10 pagesCSCP Module 3Asher50% (2)
- Basic Encaustic Manual Author R&FDocument16 pagesBasic Encaustic Manual Author R&Fagustin arellanoNo ratings yet
- Unmas Ied Lexicon 0Document71 pagesUnmas Ied Lexicon 0Victor AryeeNo ratings yet
- Telecom Business Management Systems Net ProjectDocument68 pagesTelecom Business Management Systems Net ProjectRahul RaiNo ratings yet
- Touch-Tone Recognition: EE301 Final Project April 26, 2010 MHP 101Document20 pagesTouch-Tone Recognition: EE301 Final Project April 26, 2010 MHP 101Sheelaj BabuNo ratings yet
- Elah'Im CultureDocument60 pagesElah'Im CultureRichard David DellermanNo ratings yet
- Splices: S100 S100 S101 S101 S101 S102Document3 pagesSplices: S100 S100 S101 S101 S101 S102Albert BriceñoNo ratings yet
- Clay Brick Making Machine Mew CB 3000Document5 pagesClay Brick Making Machine Mew CB 3000Aakansh NigamNo ratings yet
- A Review of Air Filter TestDocument14 pagesA Review of Air Filter Testhussain mominNo ratings yet
- Modul Hots (Kbat) Kimia Tingkatan 5Document15 pagesModul Hots (Kbat) Kimia Tingkatan 5Hairul Razif Mohd IdrisNo ratings yet
- NES 362 Type and Production Testing of Mechanical Equipment Category 3Document36 pagesNES 362 Type and Production Testing of Mechanical Equipment Category 3JEORJENo ratings yet
- PhotosynthesisDocument30 pagesPhotosynthesisAngela CanlasNo ratings yet
- IGO Operations Manual PDFDocument2,251 pagesIGO Operations Manual PDFMardi Wirengkoso100% (1)
- Section 5: Finite Volume Methods For The Navier Stokes EquationsDocument27 pagesSection 5: Finite Volume Methods For The Navier Stokes EquationsUmutcanNo ratings yet