Professional Documents
Culture Documents
Mehu130 - U2 - T47 - EPOC Seminario
Uploaded by
Gabriel OlivaresOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Mehu130 - U2 - T47 - EPOC Seminario
Uploaded by
Gabriel OlivaresCopyright:
Available Formats
Seminar
Chronic obstructive pulmonary disease
Klaus F Rabe, Henrik Watz
Chronic obstructive pulmonary disease (COPD) kills more than 3 million people worldwide every year. Despite Lancet 2017; 389: 1931–40
progress in the treatment of symptoms and prevention of acute exacerbations, few advances have been made to Pulmonary Research Institute
ameliorate disease progression or affect mortality. A better understanding of the complex disease mechanisms (H Watz MD), LungenClinic
Grosshansdorf (K F Rabe MD),
resulting in COPD is needed. Smoking cessation programmes, increasing physical activity, and early detection and Airway Research Centre North,
treatment of comorbidities are further key components to reduce the burden of the disease. However, without a German Centre for Lung
global political and economic effort to reduce tobacco use, to regulate environmental exposure, and to find alternatives Research, Grosshansdorf,
to the massive use of biomass fuel, COPD will remain a major health-care problem for decades to come. Germany; and Department of
Medicine, Christian Albrechts
University Kiel, Kiel, Germany
Introduction countries. This risk was similar to the lifetime risk of (K F Rabe)
Chronic obstructive pulmonary disease (COPD) is developing diabetes in Canada and much higher than the Correspondence to:
common worldwide and causes a major health-care risk of congestive heart failure.8 Prof Klaus F Rabe, LungenClinic
burden. Although COPD generally manifests at an older Regionally, there are not only differences in the Grosshansdorf, 22927
Grosshansdorf, Germany
age as part of multimorbidity, there is increasing prevalence of COPD, with the highest prevalence in the
k.f.rabe@lungenclinic.de
evidence that events early in life contribute to impaired Americas (about 15% in 2010), but also in the percentage
lung function in adults,1 which suggests that risk factors increase in COPD over the past 20 years.7 The highest
other than those already known (inhaled particles and increase between 1990 and 2010 occurred in the Eastern
gases from cigarette smoking and biomass fuel) are Mediterranean (119%) and African (102%) regions.7
important in the disease’s aetiology. One of the main difficulties in estimating the global
The term COPD might be too general, since the airway prevalence of COPD is underdiagnosis, especially in low-
abnormalities of chronic bronchitis and the peripheral income countries.9 COPD is especially underdiagnosed
loss of parenchymal lung texture in emphysema are in younger patients, never or current smokers, and
probably caused by diverse cellular and pathophysiological patients with less severe disease or lower education.9
changes with distinct genetic backgrounds. Advances in Although COPD is more common in men than in
lung imaging enable a more detailed view of airway and women,7 the increase in tobacco smoking among women
lung parenchyma abnormalities and novel endoscopic in high-income countries and the higher risk of exposure
interventions play an increasing role in the management to indoor air pollution, such as biomass fuel used for
of advanced emphysema. No drug treatment specifically cooking and heating, in low-income countries, might
targets emphysema except for the augmentation of lead to a similar prevalence in the sexes in the future.10
α1 antitrypsin in patients with emphysema associated The high susceptibility to the development of airflow
with α1 antitrypsin deficiency.2 Although the results of limitation in women compared with men will also
large clinical trials support a shift from anti-inflammatory increase the risk of COPD in women.11–13
treatment with inhaled corticosteroids towards dual The high prevalence of COPD makes it one of the
bronchodilator treatment for airway pathology,3 further leading causes of morbidity and mortality worldwide. In
prospective studies will help to clarify the role of inhaled 2015, COPD ranked third among the global age-
corticosteroid treatment in combination with dual standardised death rates for both sexes, with about
bronchodilator therapy in the prevention of exacerbations.4 3·2 million patients dying of the disease.14 The top two
By contrast with asthma, there is little hope that COPD- causes of death are ischaemic heart disease and cerebro
specific biological therapies can be developed. vascular disease.14 However, considering that a third of
patients with COPD die of cardiovascular diseases,15,16 and
Epidemiology and causes a third of patients with cardiovascular disease have airflow
The global prevalence of COPD is difficult to estimate limitation,17 global mortality rates attributable to COPD
because of the different approaches used to calculate might be further underestimated. The global mortality
prevalence (eg, spirometry-confirmed airflow limitation
or surveys).5 The Global Burden of Disease Study 2015
estimated the global prevalence of COPD at about Search strategy and selection criteria
174 million cases.6 In 2010, Adeloye and colleagues7 We searched Medline and online publications on COPD and
estimated a global prevalence of 384 million cases on the tobacco use worldwide (eg, WHO) using the terms COPD,
basis of spirometric criteria of fixed airflow limitation emphysema, tobacco use, epidemiology, cause, emphysema,
applied in several epidemiological cohorts. In Canada, comorbidities, lung cancer, treatment, pulmonary
the overall risk of developing COPD by the age of 80 years rehabilitation, physical activity, and exacerbation. We focused
has been calculated to be 28%, according to population- on recent publications in English up to 2016 that might be of
based health administrative data.8 These data might help interest for a general readership.
to estimate the burden of COPD in high-income
www.thelancet.com Vol 389 May 13, 2017 1931
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
Early life events Risk factors for Escalation of treatment Clinical phenotypes of severe COPD
incidence and progress
Consider
emphysema
intervention
Consider
non-invasive
ventilation
Smoking cessation
• Genes
• Lung function at Physical activity
adolescence and adulthood Vaccination
• Exposure to other pollutants Bronchodilatation Oxygen
• Infections Palliative care
Diagnosis and treatment
• Amount of cigarettes
of comorbidities
• Physical
inactivity Pulmonary
rehabilitition
Consider inhaled
corticosteroids
Consider roflumilast
Consider macrolides
Figure 1: Life course of COPD and the effect of different factors including early life events that might affect disease incidence and disease severity along with
the treatments according to different clinical phenotypes once COPD is established and becomes severe
Patients with the so-called pink-puffer phenotype of COPD (right upper corner) are primarily affected by emphysema, whereas those with the so-called blue bloater
phenotype (right lower corner) predominantly have chronic bronchitis. Credit: Eddie Lawrence/Science Photo Library; Hindustan Times/Getty; Dr P Marazzi/Science
Photo Library; Science Photo Library. COPD=chronic obstructive pulmonary disease.
rate of COPD increased between 2005 and 2015, mainly Pathophysiology
because of an ageing population,14,18 while age-specific Clinical treatment guidelines issued by global
death rates decreased.18 Correspondingly, patients with professional societies tend to oversimplify the definition
disability increased by 16% during the same period.6 of COPD, which in fact is a heterogeneous and complex
Almost 90% of deaths due to COPD occur in low-income disease.24 Furthermore, most (if not all) knowledge about
and middle-income countries.10 Therefore, any success in the pathophysiology of the disease is derived from
combating the excessive mortality from COPD can only studies of former or current tobacco smokers. However,
be made if future global disease programmes put a COPD caused by biomass fuel exposure, for example,
greater emphasis on these countries. might be substantially different from COPD caused by
Tobacco smoking is the main cause of COPD globally.19 tobacco smoking in terms of phenotype, comorbidities,
Even though the proportion of people who smoke declined and progression of the disease.23,25
between 1990 and 2015 (by 28% in men and 29% in COPD is an often progressive inflammatory disease of
women)20 1·1 billion people still smoked tobacco in 2015.21 the airways, the alveoli, and the microvasculature; which
Smoking is most common in males aged 15 years or older of these aspects are preventable and treatable is debated.
in the western Pacific (49%), Europe (39%), southeast The key functional feature of COPD is irreversible
Asia (32%), and the eastern Mediterranean (26%).22 Other limitation of airflow. The disease process includes
risk factors, such as inhalation of smoke from biomass remodelling of the small-airway compartment and loss
fuel or ambient particulate matter, may become more of elastic recoil by emphysematous destruction of
important, especially in low-income countries. More parenchyma resulting in a progressive decline of forced
people are exposed to smoke and particles from biomass expiratory volume in 1 s (FEV1), inadequate lung
fuel worldwide than from tobacco smoke.23 Ambient par emptying on expiration, and subsequent static and
ticulate matter pollution and occupational exposure to dynamic hyperinflation.26 Large cohort studies27,28 suggest
second-hand smoke has increased substantially over the that emphysema and airway disease are also present in a
past 25 years,20 giving rise to speculation that these factors substantial number of symptomatic smokers and former
might become a greater cause of COPD in the future. smokers even without evidence of airflow limitation. In
Currently, exposure to indoor smoke from biomass fuels is addition to environmental exposures, genetic risk factors
estimated to account for 35% of COPD cases in low- are increasingly implicated in the development of
income and middle-income countries.19 nicotine addiction, chronic bronchitis, loss of lung
1932 www.thelancet.com Vol 389 May 13, 2017
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
function, and early lung development.29,30 Furthermore,
epigenetic regulation has been implicated in the
pathogenesis of COPD.31 In patients with mild airflow Early life
events
obstruction, several compensatory and adaptive Physical
physiological mechanisms ensure that the respiratory inactivity
system fulfils its primary task of maintaining adequate Osteoporosis Depression
pulmonary gas exchange.32 However, these patients have
Age
not been studied extensively. Understanding these early Muscle
COPD Lung cancer
changes and their relation to the development of injury depletion
of small airways and alveoli could aid the development of
effective preventive treatments.
Exposure to common risk factors can lead to mucosal Cardiovascular disease
Inflammation Smoking and
and glandular inflammation, with increased mucous environment
discharge and epithelial cell hyperplasia and altered
tissue repair in small conducting airways in the case of
chronic bronchitis.33 With the widespread application
of CT in clinical care, more patients have evidence of Figure 2: Interactions between risk factors for COPD and comorbidities
usually mild bronchiectasis on CT scans that is not Shared risk factors (age, smoking, inflammation, and physical inactivity) predispose people to COPD and other
chronic diseases. COPD might further increase the risk of other chronic diseases via similar mechanisms
readily detectable on conventional chest x-rays.34 These (eg, physical inactivity and inflammation). Other chronic diseases in turn worsen morbidity and mortality of COPD.
anatomical airway abnormalities in patients with primary COPD=chronic obstructive pulmonary disease.
COPD might represent a further distinct phenotype
within the spectrum of COPD.34 However, McDonough around the small airways;42,43 this might indicate adaptive
and colleagues35 have shown that increased airway or autoimmune reactions that underlie the chronic
resistance in patients with COPD might be the result of mucosal inflammatory responses of bronchitis noted
narrowing and disappearance of small conducting years after patients with COPD have stopped smoking.33
airways and respiratory bronchioles preceding the Impaired immune regulation probably plays a major
development of emphysema. These findings are probably part in COPD, and in emphysema in particular. Normal
crucial to the understanding of early disease development ageing and pulmonary emphysema share patho
and the pathways that lead to the diverse COPD physiological features, and physiological ageing of the
phenotypes. The findings also raise the question of when lung involves enlargement of alveolar space and loss of
conducting airways disappear, which also informs elastic recoil.44,45 Cell senescence generally leads to
discussion of COPD diversity. By contrast with earlier decreased proliferation with preserved metabolic activity,
ideas, some people with COPD do not show an excess of resulting in increased inflammation, reduced cell
lung function decline over time.36 The mounting evidence regeneration, and carcinogenesis.33 This process is
that early life changes have a profound effect on the further accelerated through cigarette smoking and
natural course of the disease through the establishment oxidative stress.46 Emphysema in COPD can be
of an individual level of lung function has challenged the interpreted as accelerated ageing of the lung, since the
concept of a single natural history of COPD (figure 1).1 disease process shows striking similarities with age-
These data might also help to clarify the somewhat associated features, such as cellular senescence,
obscure terminology around the clinical overlap of autophagy, defective mitochondrial function, stem-cell
asthma and COPD. The trajectory of a lifelong change in exhaustion, and immunosenescence.47
lung function37 is not a prerequisite for persistent asthma COPD often presents in elderly individuals as one
but is common in COPD (figure 1).38 component of multimorbidity (figure 2). The term COPD
The injury of airway epithelial cells triggers a non- may one day need correction since the genetic
specific inflammatory response through the release of background, pathophysiology, therapeutic targets, and
endogenous intracellular molecules or danger-associated disease management differ considerably in patients with
molecular patterns. These signals are identified by predominant airway abnormalities or dominant
pattern-recognition receptors, such as Toll-like receptors 4 emphysema. Major advances in lung imaging have
and 2 on epithelial cells, and result in the release of helped pave the way for a new idea of COPD diversity
cytokines such as tumour necrosis factor α and (figure 3).48,49 More detailed knowledge about the risk
interleukins 1 and 8.33 Macrophages, neutrophils, factors leading to these different endotypes and
eosinophils, and dendritic cells, recruited to the site of phenotypes is needed to better delineate therapeutic
inflammation, constitute the innate immune interventions. In this context, α1 antitrypsin deficiency
response.39–41 Proteolytic enzymes and reactive oxygen might serve as an example in which a known genetic
species contribute to tissue damage, particularly when background (endotype) with a distinct clinical appearance
no antiproteases or antioxidant factors are present.33 As of emphysema (phenotype) results in a targeted
the disease progresses, lymphoid aggregates can develop therapeutic intervention (α1 antitrypsin augmentation).2
www.thelancet.com Vol 389 May 13, 2017 1933
Illustration:
Descargado para 16TL_8529_3 Y Private
Anonymous User (n/a) en Antenor Orrego N University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
disease (a risk factor for major cardiovascular events)66 or
A B
coronary artery calcium scoring on CT scans67 might help
to identify those patients at risk; however, it needs to be
validated in prospective longitudinal studies. Results of
lung cancer screening in patients with COPD show a
doubling of lung cancer incidence, no apparent
overdiagnosis, and a more favourable stage shift compared
with smokers who do not have COPD.68 However,
mortality in this specific group of patients is unclear.
Treatment of COPD
Smoking cessation
Smoking cessation is key to reducing progressive decline
in lung function over time, as well as exacerbations and
smoking-related comorbidities (lung cancer and cardio
vascular disease), which decreases mortality in patients
with COPD.15,69,70 Reducing indoor air pollution by using a
stove instead of cooking on an open fire reduces
progressive lung function decline in a manner similar to
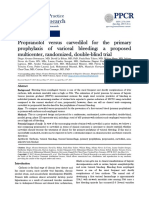
Figure 3: High-resolution CT scans of a patient with severe, bullous emphysema of centrilobular and
paraseptal phenotype
that of smoking cessation.71 Patients with COPD who
(A) axial view of the left upper lobe, (B) sagittal view of the right lung. have a high degree of tobacco dependence, and who have
comorbid depression face a major barrier to quitting
COPD and comorbidities smoking.70 Accordingly, up to 40% of patients, even
Patients with COPD are often affected by other diseases, those with severe COPD, are continuous smokers.70
such as cardiovascular disease, osteoporosis, muscle Interventions such as intensive counselling, nicotine
weakness, depression, and lung cancer.50–52 Smoking is a replacement therapy, and treatment with varenicline or
risk factor for comorbidities; others probably include bupropion increase smoking cessation and are cost-
physical inactivity and yet-to-be-identified inflammatory effective compared with counselling alone.72 However,
mechanisms (figure 2).50,51,53,54 Several pulmonary intensive smoking cessation programmes are generally
mechanisms of inflammation and oxidative stress that poorly reimbursed (if at all) by national health-care
damage DNA and result in an imbalance between tissue systems.
repair and cell proliferation seem to promote the link
between COPD and lung cancer.55–57 Grading severity and Vaccination
identifying phenotypes of COPD also mean that patients Influenza vaccination and pneumococcal vaccination are
need to be phenotyped according to their concomitant generally recommended for patients with COPD,5 as there
diseases; most patients with COPD, particularly those is some (albeit limited) evidence for specific benefits from
with mild disease, die from other causes. Lung cancer and both vaccinations for patients with COPD, such as
cardiovascular comorbidities dominate COPD mortality reduced risk of exacerbations or hospital admission.73,74
until respiratory causes contribute to overall mortality in
the advanced stages of the disease.15,16,51 Phenotyping the Physical activity
pulmonary compartment might also be relevant for the Increasing physical activity in daily life might be equally
concomitant disease: patients with COPD who have effective as smoking cessation to prevent morbidity and
predominant emphysema have a higher risk of lung mortality in patients with COPD.75–77 However, compared
cancer than do patients with a predominant airway type with physician’s knowledge of the harmful effects of
disease.58–62 Furthermore, patients with emphysema have a continuous smoking, the consequences of continuous
higher risk for osteoporosis and loss of muscle mass than physical inactivity for COPD might still be under
do patients with a predominant airway type of COPD.52,63 estimated.78 Physical inactivity early during the course of
Patients with COPD and a concomitant metabolic the disease79 is strongly linked to hospital admission75
syndrome have a higher risk profile for cardiovascular and mortality.75,77 Counselling strategies and sustained
disease,64 whereas patients with predominant emphysema motivation for patients with COPD are being evaluated
might also have a higher risk of cardiovascular disease for their ability to overcome sedentary behaviour because
because they have increased arterial stiffness.52,65 Reducing pulmonary rehabilitation and bronchodilator treatment
the mortality of COPD will probably depend on whether might be of little help.80–83 Walking as little as 15 min
patients at risk for major cardiovascular events and lung per day is associated with a 14% reduced risk of all-cause
cancer can be identified early by simple and objective mortality in the general population,84 and increasing
diagnostic assessments. The ankle-brachial index, used to activity by 600 steps per day is associated with a reduced
identify patients with asymptomatic peripheral artery risk of hospital admission in patients with COPD.85
1934 www.thelancet.com Vol 389 May 13, 2017
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
These data suggest that even small changes might be inhaled corticosteroid and a LABA (fluticasone–
clinically meaningful for patients. salmeterol) in patients with moderate-to-severe COPD
and a history of exacerbations. Indacaterol–glyco
Pulmonary rehabilitation pyrronium was superior to fluticasone–salmeterol in
Pulmonary rehabilitation is an effective multidisciplinary preventing exacerbations.3 In light of this result, the
treatment strategy to improve dyspnoea, exercise question arises whether a further step up from LABA–
tolerance, and health-related quality of life.86 Although the LAMA to triple therapy consisting of a LABA, a LAMA,
classic exercise programme with individualised endurance and an inhaled corticosteroid would result in additional
and strength training remains the cornerstone of benefits. For most patients, stepping down therapy from
pulmonary rehabilitation,86,87 education, the promotion of a LABA, a LAMA, and an inhaled corticosteroid to a LABA
behavioural changes, and self-management are also and a LAMA is not associated with an increased risk of
considered essential for any successful intervention.86 exacerbations.96 However, according to post-hoc analyses
Pulmonary rehabilitation reduces hospital admissions of three large studies97–99 with treatment arms containing
and mortality in patients who have had a recent inhaled corticosteroids, a subgroup of patients with
exacerbation.88 It has also been shown to be cost-effective.89 higher blood eosinophil counts seemed to benefit from
Despite the substantial benefits, this treatment is continuous inhaled corticosteroids in addition to mono or
underutilised worldwide because of insufficient resources, dual bronchodilator therapy: fewer exacerbations
funding, and reimbursement.89 occurred when inhaled corticosteroids were part of the
inhaled maintenance therapy. Future studies will need to
Pharmacotherapy clarify the role of inhaled corticosteroids in combination
Maintenance pharmacotherapy of patients with stable with dual bronchodilator therapy for the prevention of
COPD aims to improve symptoms, health-related quality- exacerbations in patients with severe COPD.4
of-life, exercise intolerance, and the risk of exacerbations.5 In randomised controlled trials,100 bronchodilator
Inhaled long-acting β2 agonists (LABAs) and long-acting therapy (LABA, LAMA, or a combination of both) has
muscarinic antagonists (LAMAs) have similar positive been shown to be generally safe. However, because
effects on airflow limitation, reduction of air trapping, patients with major cardiac diseases are generally
and improvement of exercise intolerance.5 However, to excluded from these trials, clinicians should be aware of
prevent exacerbations the LAMA tiotropium seems to be the (usually rare) cardiac events that have been reported
superior to LABA90,91 and just as effective as a combination in meta-analyses and observational studies.100 Treatment
of fixed inhaled corticosteroid and LABA.92 The reason is with inhaled corticosteroids is associated with a higher
largely unknown but may be partly explained by risk of pneumonia in patients with severe COPD,101
β2-adrenergic receptor polymorphisms.93 Therefore, especially in patients of older age, a body-mass index of
LAMA monotherapy should be favoured over LABA less than 25 kg/m², or a history of pneumonia.102–104
monotherapy in patients with a history of exacerbations.5 Therefore, the potential benefit of reducing exacerbations
Now that several fixed combination therapies with by adding inhaled corticosteroids to a LABA needs to be
LABA and LAMA are available, the escalation of weighed against the potential risk of pneumonia.101
bronchodilator treatment is easier to handle: patients Patients with COPD with low blood eosinophil counts
need no longer inhale from several inhaler devices. might have an increased risk of pneumonia when
Although fixed dual bronchodilation has additional fluticasone (an inhaled corticosteroid) is added to their
benefits over monotherapy for airflow limitation, it is LABA treatment.105 Again, this would indicate that there
difficult to estimate those additional benefits for the is a subgroup of patients with high blood eosinophil
improvement of symptoms based on established patient- counts in whom the benefits of inhaled corticosteroid
reported outcomes.5 In part, this might be related to study treatment outweigh the risks.
design, because no studies sought patients in clinical need Once inhaled therapy is optimised, there might still be a
of escalation of therapy based on an insufficient response subgroup of patients with severe COPD who continue to
to monotherapy. One study94 specifically investigated the have exacerbations. Further treatment options for this
occurrence of exacerbations in patients with severe COPD subgroup need to be reviewed carefully in light of
by comparing the effects of fixed dual bronchodilation increasing importance of clinical characteristics and
with those of LAMA monotherapy. Significantly fewer individualised treatment decisions.106 Patients reporting
exacerbations occurred during treatment with LABA – symptoms of chronic bronchitis might benefit from the
LAMA (indacaterol–glyco pyrronium) than with LAMA addition of the oral phosphodiesterase 4 inhibitor
(glycopyrronium) monotherapy.94 Furthermore, adding a roflumilast.107 In particular, patients who have been
LAMA to LABA and an inhaled corticosteroid resulted in admitted to hospital for a COPD exacerbation or who have
fewer exacerbations than with LABA and inhaled had more than two exacerbations treated in the outpatient
corticosteroid alone.95 setting seem to benefit from this treatment.108,109 Side-
Another study3 compared a fixed combination of effects of roflumilast, such as diarrhoea, nausea, headache,
indacaterol–glycopyrronium with the combination of an and weight loss, need to be balanced against this benefit.
www.thelancet.com Vol 389 May 13, 2017 1935
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
Macrolide therapy might be another option, especially in interventions, including treatment with thermal vapour or
patients who are ex-smokers.110,111 However, macrolide- sclerosing agents, show some efficacy but might lead to
related side-effects, uncertainty about treatment beyond even more complications.121,125 An intervention using an
1 year, and bacterial resistance to macrolides need to be endobronchial bypass did not show any sustainable benefit
considered.5 Data regarding the addition of the mucolytic in patients with severe homogeneous emphysema.126 For
and antioxidative agent N-acetylcysteine to regular COPD patients with very advanced disease, lung transplantation
drugs are difficult to interpret for patients with severe is still an option to improve quality of life and exercise
COPD and maximised inhaled therapy.112,113 capacity, but has no effect on overall survival.5
There are limitations to the evidence base for
pharmacotherapies for COPD. Almost all pharma Oxygen and ventilatory support
cotherapy studies have included patients who were Patients with stable COPD and moderate resting or
continuous or former smokers with a smoking history of exercise-induced desaturation do not benefit from long-
at least 10 pack-years, and excluded patients with term oxygen therapy in terms of mortality, exacerbations,
concomitant asthma. It is not known how effective drugs or functional status.127 However, long-term oxygen therapy
for COPD are in patients who have never smoked or in should still be prescribed for patients with severe resting
those who also have asthma. Furthermore, large studies hypoxaemia (partial pressure O2 in arterial blood [PaO2]
have recruited patients with a certain degree of airflow ≤55 mm Hg)128 or patients with more moderate hypoxaemia
limitation, symptoms, or history of exacerbations, but it is (PaO2 ≤60 mm Hg) and signs of heart failure, pulmonary
likely that patients with predominant emphysema will hypertension, or polycythaemia.5
respond differently to therapy than will patients with Studies of survival following non-invasive positive airway
predominant airway abnormalities. pressure ventilation in patients with stable hypercapnia are
Considerable efforts have been made over the past not consistently positive.5 However, non-invasive positive
decade to find new therapies that target inflammation in pressure ventilation in patients with stable hypercapnic
COPD,114 but with little success. This might partly be a and high inspiratory pressures targeted to reduce partial
result of the complexity of inflammation and related pressure of CO2 in arterial blood (PaCO2) by at least 20% or
clinical phenotypes.115 Targeting a single inflammatory to achieve PaCO2 values of less than 6·5 kPa can improve
pathway or mechanism might not be sufficient to survival.129 Therefore, this option might be considered in
persistently suppress inflammation in all patients with appropriate patients and specialised home-care settings.
COPD.116,117 Furthermore, although targeting neutrophilic
airway inflammation with a CXCR2 antagonist can Treatment of comorbidities
improve lung function and reduce exacerbations in The treatment of comorbidities has a central role in the
patients with COPD who still smoke, serious side-effects management of patients. Physicians treating COPD
such as neutropenia might prohibit further developments.118 should either treat concomitant disease themselves or
Changing the formulation so that patients inhale certain refer the patients to colleagues in the respective
compounds, such as phosphodiesterase inhibitors, might disciplines. In the absence of any COPD-specific data,
help to target the lung but limit side-effects.119,120 Whereas each comorbidity should be treated according to the usual
the efficacy of bronchodilators can be shown in short-term standards for the disease.5 Some drugs for treatment of
studies in a small number of patients, longer studies in COPD have been assessed for treatment effects beyond
highly selected subgroups are needed in early study phases the lung. The inhaled combination of fluticasone furoate–
for drugs to target inflammation, which makes drug vilanterol (an inhaled corticosteroid and a LABA) did not
development more difficult. affect mortality or cardiovascular outcomes in patients
with moderate COPD and at increased risk for
Interventional treatments cardiovascular disease,130 but it improved hyperinflation-
Interventions to reduce emphysema-associated lung associated underfilling of the heart.131 Roflumilast
hyperinflation in patients with advanced COPD under treatment was associated with fewer major cardiovascular
optimal medical care include lung volume reduction events in a pooled analysis,132 but no randomised controlled
surgery and bronchoscopic interventions such as study has been done to test the potential benefits of
endobronchial valves and lung volume reduction coils.5,121 roflumilast treatment for cardio vascular outcomes in
Approval of bronchoscopic interventional therapies by COPD. Roflumilast might have benefits for patients with
health authorities, availability, and reimbursement differ COPD and diabetes, as suggested by data on glucose
from country to country. Individualised decisions for control in patients with diabetes who do not have COPD.133
treatment should be based on characteristics of the
emphysema (eg, heterogeneous vs homogeneous, intact Clinical trials in COPD: what is in the pipeline?
lobar fissure or collateral ventilation).121,122 For most There are several early phase trials with novel drugs for
patients, treatment effects are modest and need to be COPD.134 Many ongoing clinical trials with established
balanced against potential complications such as therapies are assessing the role of either inhaled dual
pneumothorax, pneumonia, and bleeding.123,124 Other bronchodilators compared with LAMA monotherapy
1936 www.thelancet.com Vol 389 May 13, 2017
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
(ClinicalTrials.gov, NCT02296138) or fixed-dose triple and biological understanding of this disease in its distinct
therapy consisting of a LABA, a LAMA, and an endotypes and phenotypes is needed to enable innovative
inhaled corticosteroid compared with fixed-dose dual drug development.
bronchodilators or fixed-dose treatment with an Contributors
inhaled corticosteroid and a LABA4 (ClinicalTrials.gov, KFR and HW searched the published work and wrote the Seminar.
NCT02465567, NCT02579850). Unfortunately, we know Declaration of interests
of no ongoing clinical phase 3 studies of truly novel drugs KFR has received personal fees from AstraZeneca, Takeda, Chiesi,
for patients with COPD. Novartis, Boehringer Ingelheim, Sanofi Aventis, Berlin Chemie,
and Teva, and grants from Chiesi. HW has received personal fees from
AstraZeneca, Takeda, Chiesi, Novartis, Boehringer Ingelheim,
Treatment of exacerbations of COPD GlaxoSmithKline, and Berlin Chemie.
Exacerbations of COPD are acute episodes of worsening References
respiratory symptoms (dyspnoea, cough, sputum 1 Martinez FD. Early-life origins of chronic obstructive pulmonary
volume, and purulence) that require a change in disease. N Engl J Med 2016; 375: 871–78.
2 Chapman KR, Burdon JG, Piitulainen E, et al.
treatment.5 Exacerbations negatively affect lung function Intravenous augmentation treatment and lung density in severe
decline, health-related quality of life, and prognosis.135 alpha1 antitrypsin deficiency (RAPID): a randomised, double-blind,
The leading symptom for hospital admissions is placebo-controlled trial. Lancet 2015; 386: 360–68.
3 Wedzicha JA, Banerji D, Chapman KR, et al.
dyspnoea,136 and most events are triggered by viral or Indacaterol-glycopyrronium versus salmeterol-fluticasone for COPD.
bacterial respiratory tract infections.135 Milder episodes N Engl J Med 2016; 374: 2222–34.
are usually handled by patients at home by increasing 4 Pascoe SJ, Lipson DA, Locantore N, et al. A phase III randomised
their use of short-acting reliever medications. More controlled trial of single-dose triple therapy in COPD: the IMPACT
protocol. Eur Respir J 2016; 48: 320–30.
troublesome and persistent symptoms require further 5 GOLD 2017 Global Strategy for the Diagnosis, Management and
diagnostic testing to rule out cardiovascular events, Prevention of COPD; http://goldcopd.org/gold-2017-global-
pulmonary embolism, and pneumonia. Systemic strategy-diagnosis-management-prevention-copd/ (accessed
Nov 26, 2016).
steroid treatment for a short period (eg, 40 mg of 6 Global, regional, and national incidence, prevalence, and years lived
prednisone for 5 days)137 with or without a short course with disability for 310 diseases and injuries, 1990-2015: a systematic
of antibiotics is the treatment of choice for these acute analysis for the Global Burden of Disease Study 2015. Lancet 2016;
388: 1545–602.
events. For moderate events, empirical treatment with 7 Adeloye D, Chua S, Lee C, et al. Global and regional estimates of
antibiotics added to systemic steroids is controversial.138 COPD prevalence: systematic review and meta-analysis. J Glob Health
Severe exacerbations require hospital admission and 2015; 5: 020415.
8 Gershon AS, Warner L, Cascagnette P, Victor JC, To T. Lifetime risk
individualised treatments, including non-invasive of developing chronic obstructive pulmonary disease: a longitudinal
ventilatory support, oxygen therapy, treatment of population study. Lancet 2011; 378: 991–96.
concomitant diseases (eg, heat failure, pneumonia), and, 9 Lamprecht B, Soriano JB, Studnicka M, et al. Determinants of
ultimately, invasive ventilation with a poor prognosis for underdiagnosis of COPD in national and international surveys. Chest
2015; 148: 971–85.
weaning and recovery. Cohort studies show that more 10 World Health Organization. Chronic respiratory diseases. Burden of
than half of patients admitted to hospital for COPD COPD. http://www.who.int/respiratory/copd/burden/en/ (accessed
exacerbation also have cardiovascular disease.139 Even Nov 19, 2016).
11 Han MK, Postma D, Mannino DM, et al. Gender and chronic
without clinical signs of cardiac involvement, biochemical obstructive pulmonary disease: why it matters.
evidence of cardiac dysfunction (eg, high concentrations Am J Respir Crit Care Med 2007; 176: 1179–84.
of troponin I or B-type natriuretic peptide) during 12 Sorheim IC, Johannessen A, Gulsvik A, Bakke PS, Silverman EK,
DeMeo DL. Gender differences in COPD: are women more
exacerbation is common.139 About 20% of exacerbations susceptible to smoking effects than men? Thorax 2010;
might be due to worsening of an underlying cardiovascular 65: 480–85.
disease.139 Prognosis after hospital admission is poor. In 13 Luoto JA, Elmstahl S, Wollmer P, Pihlsgard M. Incidence of airflow
Europe, 11% of patients died within 90 days of admission limitation in subjects 65-100 years of age. Eur Respir J 2016;
47: 461–72.
to hospital; half while still in hospital.136 35% of patients 14 Global, regional, and national life expectancy, all-cause mortality, and
were re-admitted within 90 days.136 These numbers cause-specific mortality for 249 causes of death, 1980–2015:
indicate that management after discharge needs to be a systematic analysis for the Global Burden of Disease Study 2015.
Lancet 2016; 388: 1459–544.
improved by, for example, implementing early 15 Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE,
rehabilitation after discharge.140 Mortality from COPD Connett JE. The effects of a smoking cessation intervention on
greatly increases after repeated re-admissions.141 14.5-year mortality: a randomized clinical trial. Ann Intern Med 2005;
142: 233–39.
16 Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone
Conclusions and future directions propionate and survival in chronic obstructive pulmonary disease.
Globally, COPD will remain a significant public health N Engl J Med 2007; 356: 775–89.
17 Franssen FM, Soriano JB, Roche N, et al. Lung function
problem for the foreseeable future. With risk factors abnormalities in smokers with ischemic heart disease.
largely unchanged, demographic developments in high- Am J Respir Crit Care Med 2016; 194: 568–76.
income countries and a significant increase in non-com 18 Burney PG, Patel J, Newson R, Minelli C, Naghavi M. Global and
municable diseases in low-income countries will regional trends in COPD mortality, 1990–2010. Eur Respir J 2015;
45: 1239–47.
accelerate this health burden. A better genetic molecular
www.thelancet.com Vol 389 May 13, 2017 1937
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
19 Mannino DM, Buist AS. Global burden of COPD: risk factors, 45 Tsuji T, Aoshiba K, Nagai A. Alveolar cell senescence in patients with
prevalence, and future trends. Lancet 2007; 370: 765–73. pulmonary emphysema. Am J Respir Crit Care Med 2006; 174: 886–93.
20 Global, regional, and national comparative risk assessment of 46 Tsuji T, Aoshiba K, Nagai A. Cigarette smoke induces senescence
79 behavioural, environmental and occupational, and metabolic in alveolar epithelial cells. Am J Respir Cell Mol Biol 2004; 31: 643–49.
risks or clusters of risks, 1990–2015: a systematic analysis for the 47 Mercado N, Ito K, Barnes PJ. Accelerated ageing of the lung in
Global Burden of Disease Study 2015. Lancet 2016; 388: 1659–724. COPD: new concepts. Thorax 2015; 70: 482–89.
21 WHO. Global Health Observatory data. Prevalence of tobacco 48 Hoffman EA, Lynch DA, Barr RG, van Beek EJ, Parraga G.
smoking. http://www.who.int/gho/tobacco/use/en/ (accessed Pulmonary CT and MRI phenotypes that help explain chronic
Feb 5, 2017). pulmonary obstruction disease pathophysiology and outcomes.
22 WHO. World Health statistics 2016 data visualizations dashboard. J Magn Reson Imaging 2016; 43: 544–57.
Tobacco control. Region data. http://apps.who.int/gho/data/view. 49 Lynch DA, Austin JH, Hogg JC, et al. CT-definable subtypes of
sdg.3-a-data-reg?lang=en (accessed Feb 5, 2017). chronic obstructive pulmonary disease: a statement of the Fleischner
23 Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in Society. Radiology 2015; 277: 192–205.
non-smokers. Lancet 2009; 374: 733–43. 50 Nussbaumer-Ochsner Y, Rabe KF. Systemic manifestations of
24 Celli BR, Decramer M, Wedzicha JA, et al. An official American COPD. Chest 2011; 139: 165–73.
Thoracic Society/European Respiratory Society statement: research 51 Decramer M, Janssens W. Chronic obstructive pulmonary disease
questions in COPD. Eur Respir Rev 2015; 24: 159–72. and comorbidities. Lancet Respir Med 2013; 1: 73–83.
25 Ramirez-Venegas A, Sansores RH, Quintana-Carrillo RH, et al. 52 Vanfleteren LE, Spruit MA, Wouters EF, Franssen FM.
FEV1 decline in patients with chronic obstructive pulmonary Management of chronic obstructive pulmonary disease beyond the
disease associated with biomass exposure. lungs. Lancet Respir Med 2016; 4: 911–24.
Am J Respir Crit Care Med 2014; 190: 996–1002. 53 Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of
26 O’Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in cardiovascular comorbidity in patients with chronic obstructive
chronic obstructive pulmonary disease. Proc Am Thorac Soc 2006; pulmonary disease: a systematic review and meta-analysis.
3: 180–84. Lancet Respir Med 2015; 3: 631–39.
27 Regan EA, Lynch DA, Curran-Everett D, et al. Clinical and 54 Roversi S, Fabbri LM, Sin DD, Hawkins NM, Agusti A.
radiologic disease in smokers with normal spirometry. Chronic obstructive pulmonary disease and cardiac diseases:
JAMA Intern Med 2015; 175: 1539–49. an urgent need for integrated care. Am J Respir Crit Care Med 2016;
28 Woodruff PG, Barr RG, Bleecker E, et al. Clinical significance of 194: 1319–36.
symptoms in smokers with preserved pulmonary function. 55 Houghton AM, Mouded M, Shapiro SD. Common origins of lung
N Engl J Med 2016; 374: 1811–21. cancer and COPD. Nat Med 2008; 14: 1023–24.
29 Obeidat M, Hao K, Bosse Y, et al. Molecular mechanisms 56 Houghton AM. Mechanistic links between COPD and lung cancer.
underlying variations in lung function: a systems genetics analysis. Nat Rev Cancer 2013; 13: 233–45.
Lancet Respir Med 2015; 3: 782–95. 57 Durham AL, Adcock IM. The relationship between COPD and lung
30 Wain LV, Shrine N, Miller S, et al. Novel insights into the genetics cancer. Lung Cancer 2015; 90: 121–27.
of smoking behaviour, lung function, and chronic obstructive 58 de Torres JP, Marin JM, Casanova C, et al. Identification of COPD
pulmonary disease (UK BiLEVE): a genetic association study in patients at high risk for lung cancer mortality using the
UK Biobank. Lancet Respir Med 2015; 3: 769–81. COPD-LUCSS-DLCO. Chest 2016; 149: 936–42.
31 Brusselle GG, Bracke KR. Elucidating COPD pathogenesis by 59 de Torres JP, Wilson DO, Sanchez-Salcedo P, et al. Lung cancer in
large-scale genetic analyses. Lancet Respir Med 2015; 3: 737–39. patients with chronic obstructive pulmonary disease. Development
32 O’Donnell DE, Neder JA, Elbehairy AF. Physiological impairment and validation of the COPD Lung Cancer Screening Score.
in mild COPD. Respirology 2016; 21: 211–23. Am J Respir Crit Care Med 2015; 191: 285–91.
33 Decramer M, Janssens W, Miravitlles M. Chronic obstructive 60 de Torres JP, Marin JM, Casanova C, Cote C, et al. Lung cancer in
pulmonary disease. Lancet 2012; 379: 1341–51. patients with chronic obstructive pulmonary disease—incidence and
34 Hurst JR, Elborn JS, De Soyza A. COPD-bronchiectasis overlap predicting factors. Am J Respir Crit Care Med 2011; 184: 913–19.
syndrome. Eur Respir J 2015; 45: 310–13. 61 de Torres JP, Bastarrika G, Wisnivesky JP, et al. Assessing the
35 McDonough JE, Yuan R, Suzuki M, et al. Small-airway obstruction relationship between lung cancer risk and emphysema detected on
and emphysema in chronic obstructive pulmonary disease. low-dose CT of the chest. Chest 2007; 132: 1932–38.
N Engl J Med 2011; 365: 1567–75. 62 Sanchez-Salcedo P, Wilson DO, de Torres JP, et al.
36 Lange P, Celli B, Agusti A, et al. Lung-function trajectories leading Improving selection criteria for lung cancer screening. The potential
to chronic obstructive pulmonary disease. N Engl J Med 2015; role of emphysema. Am J Respir Crit Care Med 2015; 191: 924–31.
373: 111–22. 63 Vanfleteren LE, Spruit MA, Groenen M, et al. Clusters of
37 Fuchs O, Bahmer T, Rabe KF, von Mutius E. Asthma transition comorbidities based on validated objective measurements and
from childhood into adulthood. Lancet Respir Med 2016; published systemic inflammation in patients with chronic obstructive
online Sept 22. http://dx.doi.org/10.1016/S2213-2600(16)30187-4. pulmonary disease. Am J Respir Crit Care Med 2013; 187: 728–35.
38 Postma DS, Rabe KF. The asthma-COPD overlap syndrome. 64 Watz H, Waschki B, Kirsten A, et al. The metabolic syndrome in
N Engl J Med 2015; 373: 1241–49. patients with chronic bronchitis and COPD: frequency and
39 Demedts IK, Bracke KR, Van Pottelberge G, et al. Accumulation of associated consequences for systemic inflammation and physical
dendritic cells and increased CCL20 levels in the airways of patients inactivity. Chest 2009; 136: 1039–46.
with chronic obstructive pulmonary disease. 65 McAllister DA, Maclay JD, Mills NL, et al. Arterial stiffness is
Am J Respir Crit Care Med 2007; 175: 998–1005. independently associated with emphysema severity in patients with
40 Barnes PJ, Shapiro SD, Pauwels RA. Chronic obstructive chronic obstructive pulmonary disease. Am J Respir Crit Care Med
pulmonary disease: molecular and cellular mechanisms. 2007; 176: 1208–14.
Eur Respir J 2003; 22: 672–88. 66 Houben-Wilke S, Jorres RA, Bals R, et al. Peripheral artery disease
41 Brusselle GG, Joos GF, Bracke KR. New insights into the immunology and its clinical relevance in patients with chronic obstructive
of chronic obstructive pulmonary disease. Lancet 2011; 378: 1015–26. pulmonary disease in the COPD and Systemic Consequences–
42 Sullivan AK, Simonian PL, Falta MT, et al. Oligoclonal CD4+ T cells Comorbidities Network Study. Am J Respir Crit Care Med 2017;
in the lungs of patients with severe emphysema. 195: 189–97.
Am J Respir Crit Care Med 2005; 172: 590–96. 67 Williams MC, Murchison JT, Edwards LD, et al. Coronary artery
43 van der Strate BW, Postma DS, Brandsma CA, et al. calcification is increased in patients with COPD and associated
Cigarette smoke-induced emphysema: a role for the B cell? with increased morbidity and mortality. Thorax 2014; 69: 718–23.
Am J Respir Crit Care Med 2006; 173: 751–58. 68 Young RP, Duan F, Chiles C, et al. Airflow limitation and
44 MacNee W, Tuder RM. New paradigms in the pathogenesis of histology shift in the National Lung Screening Trial.
chronic obstructive pulmonary disease I. Proc Am Thorac Soc 2009; The NLST-ACRIN Cohort Substudy. Am J Respir Crit Care Med 2015;
6: 527–31. 192: 1060–67.
1938 www.thelancet.com Vol 389 May 13, 2017
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
69 Scanlon PD, Connett JE, Waller LA, Altose MD, Bailey WC, 89 Rochester CL, Vogiatzis I, Holland AE, et al. An Official American
Buist AS. Smoking cessation and lung function in mild-to-moderate Thoracic Society/European Respiratory Society Policy Statement:
chronic obstructive pulmonary disease. The Lung Health Study. enhancing implementation, use, and delivery of pulmonary
Am J Respir Crit Care Med 2000; 161: 381–90. rehabilitation. Am J Respir Crit Care Med 2015; 192: 1373–86.
70 Jimenez-Ruiz CA, Andreas S, Lewis KE, et al. Statement on 90 Vogelmeier C, Hederer B, Glaab T, et al. Tiotropium versus
smoking cessation in COPD and other pulmonary diseases and in salmeterol for the prevention of exacerbations of COPD.
smokers with comorbidities who find it difficult to quit. Eur Respir J N Engl J Med 2011; 364: 1093–103.
2015; 46: 61–79. 91 Decramer ML, Chapman KR, Dahl R, et al. Once-daily indacaterol
71 Romieu I, Riojas-Rodriguez H, Marron-Mares AT, Schilmann A, versus tiotropium for patients with severe chronic obstructive
Perez-Padilla R, Masera O. Improved biomass stove intervention in pulmonary disease (INVIGORATE): a randomised, blinded,
rural Mexico: impact on the respiratory health of women. parallel-group study. Lancet Respir Med 2013; 1: 524–33.
Am J Respir Crit Care Med 2009; 180: 649–56. 92 Wedzicha JA, Calverley PM, Seemungal TA, Hagan G, Ansari Z,
72 Hoogendoorn M, Feenstra TL, Hoogenveen RT, Stockley RA. The prevention of chronic obstructive pulmonary
Rutten-van Molken MP. Long-term effectiveness and cost- disease exacerbations by salmeterol/fluticasone propionate or
effectiveness of smoking cessation interventions in patients with tiotropium bromide. Am J Respir Crit Care Med 2008; 177: 19–26.
COPD. Thorax 2010; 65: 711–18. 93 Rabe KF, Fabbri LM, Israel E, et al. Effect of ADRB2
73 Poole PJ, Chacko E, Wood-Baker RW, Cates CJ. Influenza vaccine polymorphisms on the efficacy of salmeterol and tiotropium in
for patients with chronic obstructive pulmonary disease. preventing COPD exacerbations: a prespecified substudy of the
Cochrane Database Syst Rev 2006: CD002733. POET-COPD trial. Lancet Respir Med 2014; 2: 44–53.
74 Walters JA, Smith S, Poole P, Granger RH, Wood-Baker R. 94 Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic
Injectable vaccines for preventing pneumococcal infection in obstructive pulmonary disease exacerbations with the dual
patients with chronic obstructive pulmonary disease. bronchodilator QVA149 compared with glycopyrronium and
Cochrane Database Syst Rev 2010: CD001390. tiotropium (SPARK): a randomised, double-blind, parallel-group
75 Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Anto JM. study. Lancet Respir Med 2013; 1: 199–209.
Regular physical activity reduces hospital admission and mortality 95 Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus
in chronic obstructive pulmonary disease: a population based inhaled corticosteroid plus long-acting beta2-agonist therapy for
cohort study. Thorax 2006; 61: 772–78. chronic obstructive pulmonary disease (TRILOGY): a double-blind,
76 Waschki B, Kirsten AM, Holz O, et al. Disease progression and parallel group, randomised controlled trial. Lancet 2016; 388: 963–73.
changes in physical activity in patients with chronic obstruct 96 Magnussen H, Disse B, Rodriguez-Roisin R, et al. Withdrawal of
ive pulmonary disease. Am J Respir Crit Care Med 2015; inhaled glucocorticoids and exacerbations of COPD. N Engl J Med
192: 295–306. 2014; 371: 1285–94.
77 Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest 97 Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID.
predictor of all-cause mortality in patients with COPD: a prospective Blood eosinophil counts, exacerbations, and response to the
cohort study. Chest 2011; 140: 331–42. addition of inhaled fluticasone furoate to vilanterol in patients with
78 Watz H, Pitta F, Rochester CL, et al. An official European chronic obstructive pulmonary disease: a secondary analysis of data
Respiratory Society statement on physical activity in COPD. from two parallel randomised controlled trials. Lancet Respir Med
Eur Respir J 2014; 44: 1521–37. 2015; 3: 435–42.
79 Watz H, Waschki B, Meyer T, Magnussen H. Physical activity in 98 Siddiqui SH, Guasconi A, Vestbo J, et al. Blood Eosinophils:
patients with COPD. Eur Respir J 2009; 33: 262–72. a biomarker of response to extrafine beclomethasone/formoterol in
80 Spruit MA, Pitta F, McAuley E, ZuWallack RL, Nici L. chronic obstructive pulmonary disease. Am J Respir Crit Care Med
Pulmonary rehabilitation and physical activity in patients with 2015; 192: 523–25.
chronic obstructive pulmonary disease. Am J Respir Crit Care Med 99 Watz H, Tetzlaff K, Wouters EF, et al. Blood eosinophil count
2015; 192: 924–33. and exacerbations in severe chronic obstructive pulmonary
81 Beeh KM, Watz H, Puente-Maestu L, et al. Aclidinium improves disease after withdrawal of inhaled corticosteroids: a post-hoc
exercise endurance, dyspnea, lung hyperinflation, and physical analysis of the WISDOM trial. Lancet Respir Med 2016;
activity in patients with COPD: a randomized, placebo-controlled, 4: 390–98.
crossover trial. BMC Pulm Med 2014; 14: 209. 100 Lahousse L, Verhamme KM, Stricker BH, Brusselle GG.
82 Watz H, Mailander C, Baier M, Kirsten A. Effects of Cardiac effects of current treatments of chronic obstructive
indacaterol/glycopyrronium (QVA149) on lung hyperinflation and pulmonary disease. Lancet Respir Med 2016; 4: 149–64.
physical activity in patients with moderate to severe COPD: 101 Nannini LJ, Lasserson TJ, Poole P. Combined corticosteroid and
a randomised, placebo-controlled, crossover study (the MOVE long-acting beta(2)-agonist in one inhaler versus long-acting
Study). BMC Pulm Med 2016; 16: 95. beta(2)-agonists for chronic obstructive pulmonary disease.
83 Watz H, Krippner F, Kirsten A, Magnussen H, Vogelmeier C. Cochrane Database Syst Rev 2012: CD006829.
Indacaterol improves lung hyperinflation and physical activity in 102 Crim C, Calverley PM, Anderson JA, et al. Pneumonia risk in
patients with moderate chronic obstructive pulmonary disease—a COPD patients receiving inhaled corticosteroids alone or in
randomized, multicenter, double-blind, placebo-controlled study. combination: TORCH study results. Eur Respir J 2009; 34: 641–47.
BMC Pulm Med 2014; 14: 158. 103 Crim C, Dransfield MT, Bourbeau J, et al. Pneumonia risk with
84 Wen CP, Wai JP, Tsai MK, et al. Minimum amount of physical inhaled fluticasone furoate and vilanterol compared with vilanterol
activity for reduced mortality and extended life expectancy: alone in patients with COPD. Ann Am Thorac Soc 2015; 12: 27–34.
a prospective cohort study. Lancet 2011; 378: 1244–53. 104 Finney L, Berry M, Singanayagam A, Elkin SL, Johnston SL,
85 Demeyer H, Burtin C, Hornikx M, et al. The minimal important Mallia P. Inhaled corticosteroids and pneumonia in chronic
difference in physical activity in patients with COPD. PLoS One obstructive pulmonary disease. Lancet Respir Med 2014; 2: 919–32.
2016; 11: e0154587. 105 Pavord ID, Lettis S, Anzueto A, Barnes N. Blood eosinophil count
86 Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic and pneumonia risk in patients with chronic obstructive pulmonary
Society/European Respiratory Society statement: key concepts and disease: a patient-level meta-analysis. Lancet Respir Med 2016;
advances in pulmonary rehabilitation. Am J Respir Crit Care Med 4: 731–41.
2013; 188: e13–64. 106 Woodruff PG, Agusti A, Roche N, Singh D, Martinez FJ.
87 Casaburi R, ZuWallack R. Pulmonary rehabilitation for Current concepts in targeting chronic obstructive pulmonary
management of chronic obstructive pulmonary disease. disease pharmacotherapy: making progress towards personalised
N Engl J Med 2009; 360: 1329–35. management. Lancet 2015; 385: 1789–98.
88 Puhan MA, Gimeno-Santos E, Scharplatz M, Troosters T, 107 Fabbri LM, Calverley PM, Izquierdo-Alonso JL, et al. Roflumilast in
Walters EH, Steurer J. Pulmonary rehabilitation following moderate-to-severe chronic obstructive pulmonary disease treated
exacerbations of chronic obstructive pulmonary disease. with longacting bronchodilators: two randomised clinical trials.
Cochrane Database Syst Rev 2011: CD005305. Lancet 2009; 374: 695–703.
www.thelancet.com Vol 389 May 13, 2017 1939
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
Seminar
108 Martinez FJ, Calverley PM, Goehring UM, Brose M, Fabbri LM, 125 Herth FJ, Valipour A, Shah PL, et al. Segmental volume reduction
Rabe KF. Effect of roflumilast on exacerbations in patients with using thermal vapour ablation in patients with severe emphysema:
severe chronic obstructive pulmonary disease uncontrolled by 6-month results of the multicentre, parallel-group, open-label,
combination therapy (REACT): a multicentre randomised randomised controlled STEP-UP trial. Lancet Respir Med 2016;
controlled trial. Lancet 2015; 385: 857–66. 4: 185–93.
109 Martinez FJ, Rabe KF, Sethi S, et al. Effect of roflumilast and inhaled 126 Shah PL, Slebos DJ, Cardoso PF, et al. Bronchoscopic lung-volume
corticosteroid/long-acting beta2-agonist on chronic obstructive reduction with Exhale airway stents for emphysema (EASE trial):
pulmonary disease exacerbations (RE(2)SPOND). A randomized randomised, sham-controlled, multicentre trial. Lancet 2011;
clinical trial. Am J Respir Crit Care Med 2016; 194: 559–67. 378: 997–1005.
110 Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention 127 The Long-Term Oxygen Treatment Trial Research Group. A
of exacerbations of COPD. N Engl J Med 2011; 365: 689–98. randomized trial of long-term oxygen for COPD with moderate
111 Han MK, Tayob N, Murray S, et al. Predictors of chronic obstructive desaturation. N Engl J Med 2016; 375: 1617–27.
pulmonary disease exacerbation reduction in response to daily 128 Ekstrom M. Clinical usefulness of long-term oxygen therapy in
azithromycin therapy. Am J Respir Crit Care Med 2014; 189: 1503–08. adults. N Engl J Med 2016; 375: 1683–84.
112 Decramer M, Rutten-van Molken M, Dekhuijzen PN, et al. 129 Kohnlein T, Windisch W, Kohler D, et al. Non-invasive positive
Effects of N-acetylcysteine on outcomes in chronic obstructive pressure ventilation for the treatment of severe stable chronic
pulmonary disease (Bronchitis Randomized on NAC Cost-Utility obstructive pulmonary disease: a prospective, multicentre,
Study, BRONCUS): a randomised placebo-controlled trial. Lancet randomised, controlled clinical trial. Lancet Respir Med 2014;
2005; 365: 1552–60. 2: 698–705.
113 Zheng JP, Wen FQ, Bai CX, et al. Twice daily N-acetylcysteine 130 Vestbo J, Anderson JA, Brook RD, et al. Fluticasone furoate and
600 mg for exacerbations of chronic obstructive pulmonary disease vilanterol and survival in chronic obstructive pulmonary disease
(PANTHEON): a randomised, double-blind placebo-controlled trial. with heightened cardiovascular risk (SUMMIT): a double-blind
Lancet Respir Med 2014; 2: 187–94. randomised controlled trial. Lancet 2016; 387: 1817–26.
114 Barnes PJ, Hansel TT. Prospects for new drugs for chronic 131 Stone IS, Barnes NC, James WY, et al. Lung deflation and
obstructive pulmonary disease. Lancet 2004; 364: 985–96. cardiovascular structure and function in chronic obstructive
115 Martinez FJ, Donohue JF, Rennard SI. The future of chronic pulmonary disease. A randomized controlled trial.
obstructive pulmonary disease treatment--difficulties of and barriers Am J Respir Crit Care Med 2016; 193: 717–26.
to drug development. Lancet 2011; 378: 1027–37. 132 White WB, Cooke GE, Kowey PR, et al. Cardiovascular safety in
116 Watz H, Barnacle H, Hartley BF, Chan R. Efficacy and safety of the patients receiving roflumilast for the treatment of COPD. Chest
p38 MAPK inhibitor losmapimod for patients with chronic 2013; 144: 758–65.
obstructive pulmonary disease: a randomised, double-blind, 133 Wouters EF, Bredenbroker D, Teichmann P, et al. Effect of the
placebo-controlled trial. Lancet Respir Med 2014; 2: 63–72. phosphodiesterase 4 inhibitor roflumilast on glucose metabolism in
117 Brightling CE, Bleecker ER, Panettieri RA Jr, et al. Benralizumab for patients with treatment-naive, newly diagnosed type 2 diabetes
chronic obstructive pulmonary disease and sputum eosinophilia: mellitus. J Clin Endocrinol Metab 2012; 97: E1720–25.
a randomised, double-blind, placebo-controlled, phase 2a study. 134 Gross NJ, Barnes PJ. New therapies for asthma and chronic
Lancet Respir Med 2014; 2: 891–901. obstructive pulmonary disease. Am J Respir Crit Care Med 2017;
118 Rennard SI, Dale DC, Donohue JF, et al. CXCR2 antagonist 195: 159–66.
MK-7123. A phase 2 proof-of-concept trial for chronic obstructive 135 Wedzicha JA, Seemungal TA. COPD exacerbations: defining their
pulmonary disease. Am J Respir Crit Care Med 2015; 191: 1001–11. cause and prevention. Lancet 2007; 370: 786–96.
119 Franciosi LG, Diamant Z, Banner KH, et al. Efficacy and safety of 136 Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, et al. Risk of death
RPL554, a dual PDE3 and PDE4 inhibitor, in healthy volunteers and and readmission of hospital-admitted COPD exacerbations:
in patients with asthma or chronic obstructive pulmonary disease: European COPD Audit. Eur Respir J 2016; 47: 113–21.
findings from four clinical trials. Lancet Respir Med 2013; 1: 714–27. 137 Leuppi JD, Schuetz P, Bingisser R, et al. Short-term vs conventional
120 Watz H, Mistry SJ, Lazaar AL. Safety and tolerability of the inhaled glucocorticoid therapy in acute exacerbations of chronic obstructive
phosphodiesterase 4 inhibitor GSK256066 in moderate COPD. pulmonary disease: the REDUCE randomized clinical trial. JAMA
Pulm Pharmacol Ther 2013; 26: 588–95. 2013; 309: 2223–31.
121 Shah PL, Herth FJ, van Geffen WH, Deslee G, Slebos DJ. 138 Rohde GG, Koch A, Welte T. Randomized double blind placebo-
Lung volume reduction for emphysema. Lancet Respir Med 2016; controlled study to demonstrate that antibiotics are not needed in
5: 147–56. moderate acute exacerbations of COPD--the ABACOPD study.
122 Herth FJ, Slebos DJ, Rabe KF, Shah PL. Endoscopic lung volume BMC Pulm Med 2015; 15: 5.
reduction: an expert panel recommendation. Respiration 2016; 139 MacDonald MI, Shafuddin E, King PT, Chang CL, Bardin PG,
91: 241–50. Hancox RJ. Cardiac dysfunction during exacerbations of chronic
123 Sciurba FC, Criner GJ, Strange C, et al. Effect of endobronchial obstructive pulmonary disease. Lancet Respir Med 2016; 4: 138–48.
coils vs usual care on exercise tolerance in patients with severe 140 Wedzicha JA, Miravitlles M, Hurst JR, et al. Management of COPD
emphysema: the RENEW randomized clinical trial. JAMA 2016; exacerbations: a European Respiratory Society/American Thoracic
315: 2178–89. Society guideline. Eur Respir J 2017; 49: 1600791.
124 Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of 141 Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of
endobronchial valves for advanced emphysema. N Engl J Med 2010; chronic obstructive pulmonary disease: severe exacerbations and
363: 1233–44. mortality. Thorax 2012; 67: 957–63.
1940 www.thelancet.com Vol 389 May 13, 2017
Descargado para Anonymous User (n/a) en Antenor Orrego Private University de ClinicalKey.es por Elsevier en mayo 24, 2020.
Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2020. Elsevier Inc. Todos los derechos reservados.
You might also like
- COPD Lancet PDFDocument10 pagesCOPD Lancet PDFDickyNo ratings yet
- Mechanistic links between COPD and lung cancerDocument13 pagesMechanistic links between COPD and lung cancerHoracioNo ratings yet
- Copd and Cardiovascular Disease: Original ArticleDocument9 pagesCopd and Cardiovascular Disease: Original Articlemgoez077No ratings yet
- Copd and CVD Pulmonology JournalDocument9 pagesCopd and CVD Pulmonology JournalKessi VikaneswariNo ratings yet
- Acute Exacerbation of COPD Is It The Stroke of The LungsDocument9 pagesAcute Exacerbation of COPD Is It The Stroke of The LungsBruna AlencarNo ratings yet
- Do Inhaled Corticosteroids Protect Against Lung Cancer in Patients With COPD A Systematic ReviewDocument10 pagesDo Inhaled Corticosteroids Protect Against Lung Cancer in Patients With COPD A Systematic ReviewRicovially DavyaNo ratings yet
- COPDex Stroke 2017Document8 pagesCOPDex Stroke 2017Angelica ChavesNo ratings yet
- EPOC LancetDocument16 pagesEPOC LancetKarliux JimenezNo ratings yet
- Chronic Obstructive Pulmonary Disease: An Overview: John F. Devine, DO, FACPDocument9 pagesChronic Obstructive Pulmonary Disease: An Overview: John F. Devine, DO, FACPAngelica GatdulaNo ratings yet
- Obesity Lung COPDDocument8 pagesObesity Lung COPDDumitru BiniucNo ratings yet
- An Overview: Chronic Obstructive Pulmonary DiseaseDocument9 pagesAn Overview: Chronic Obstructive Pulmonary Diseaseulfiandi rizkiNo ratings yet
- Concise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseDocument10 pagesConcise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseMuhammad FakhruriNo ratings yet
- Pauwels 2004Document8 pagesPauwels 2004srichakadharsri911No ratings yet
- HHS Public Access: Chronic Obstructive Pulmonary DiseaseDocument20 pagesHHS Public Access: Chronic Obstructive Pulmonary DiseaseafifahNo ratings yet
- NatureDP 2015 Chronic Obstructive Pulmonary DiseaseDocument21 pagesNatureDP 2015 Chronic Obstructive Pulmonary DiseasePaloma GBNo ratings yet
- Atm 04 08 160Document9 pagesAtm 04 08 160manalNo ratings yet
- Christenson Stephanie A Chronic Obstructive PulmonaryDocument16 pagesChristenson Stephanie A Chronic Obstructive PulmonarynomokickNo ratings yet
- P 6 B 06 Sample 01Document15 pagesP 6 B 06 Sample 01adjoaaframd12No ratings yet
- Chronic Bronchitis and COPDDocument11 pagesChronic Bronchitis and COPDRodli AkbarNo ratings yet
- Chronic Obstructive Pulmonary Disease (Lancet)Document16 pagesChronic Obstructive Pulmonary Disease (Lancet)marcos gamboaNo ratings yet
- Update On The Pathogenesis of Chronic Obstructive Pulmonary DiseaseDocument9 pagesUpdate On The Pathogenesis of Chronic Obstructive Pulmonary DiseaseHum BlumNo ratings yet
- Non Farmako Mulhall ReviewDocument19 pagesNon Farmako Mulhall Reviewgita cahayaNo ratings yet
- Ajplung 00400 2021Document5 pagesAjplung 00400 2021YaYakNo ratings yet
- American Thoracic Society DocumentsDocument26 pagesAmerican Thoracic Society DocumentsGold4allNo ratings yet
- TB-Linked COPD Risk FactorsDocument11 pagesTB-Linked COPD Risk FactorsAntoninus HengkyNo ratings yet
- COPDDocument2 pagesCOPDSérgio PauloNo ratings yet
- Medical Progress: C O P DDocument12 pagesMedical Progress: C O P DPablo CamposNo ratings yet
- Clinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary DiseaseDocument11 pagesClinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary DiseaseAgatha GeraldyneNo ratings yet
- ComBat 2020-06-21 14 - 49 - 27Document23 pagesComBat 2020-06-21 14 - 49 - 27gfdsgefgijNo ratings yet
- Choudhury 2014Document30 pagesChoudhury 2014Andry Wahyudi AgusNo ratings yet
- Agusti Et Al-2023-Clinical Research in CardiologyDocument10 pagesAgusti Et Al-2023-Clinical Research in CardiologySupaluk Mod ChuencheepNo ratings yet
- Prevalence and Attributable Health Burden of Chronic Respiratory DiseasesDocument12 pagesPrevalence and Attributable Health Burden of Chronic Respiratory DiseasesNjala SankhulaniNo ratings yet
- COPD2019Document9 pagesCOPD2019ClintonNo ratings yet
- GOLD SlideSet 2017Document88 pagesGOLD SlideSet 2017RicoPratamaWiyonoNo ratings yet
- Emboli Paru & PPOKDocument7 pagesEmboli Paru & PPOKsukiyantoNo ratings yet
- 1 s2.0 S0300289623000364 MainDocument17 pages1 s2.0 S0300289623000364 MainwulanesterNo ratings yet
- Copd Nihilismo BuenisimoDocument8 pagesCopd Nihilismo BuenisimoJose Lopez FuentesNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document7 pagesChronic Obstructive Pulmonary Disease (COPD)Dwight Lhenard TuazonNo ratings yet
- 2011 in The Clinic - EPOCDocument16 pages2011 in The Clinic - EPOCKarla WevarNo ratings yet
- 956 FullDocument7 pages956 FullayuNo ratings yet
- Air Pollution As An Early Determinant of COPD: Zhuyi Lu, Patrice Coll, Bernard Maitre, Ralph Epaud and Sophie LanoneDocument13 pagesAir Pollution As An Early Determinant of COPD: Zhuyi Lu, Patrice Coll, Bernard Maitre, Ralph Epaud and Sophie LanoneywtmyxpezickztrkcfNo ratings yet
- Caramori 2019Document16 pagesCaramori 2019Dusan MilovanovicNo ratings yet
- GOLD SlideSet 2017Document103 pagesGOLD SlideSet 2017LengNo ratings yet
- Epidemiology of Chronic Obstructive Pulmonary Disease: A Literature ReviewDocument39 pagesEpidemiology of Chronic Obstructive Pulmonary Disease: A Literature ReviewgalihNo ratings yet
- Gold 2023 (016 193)Document178 pagesGold 2023 (016 193)Mariana Tovar RodriguezNo ratings yet
- Metoprolol y El EPOCDocument10 pagesMetoprolol y El EPOCMadyurit RamírezNo ratings yet
- Acute Exacerbations of COPD and Risk of Lung Cancer in COPD Patients With and Without A History of AsthmaDocument9 pagesAcute Exacerbations of COPD and Risk of Lung Cancer in COPD Patients With and Without A History of AsthmaHaidir MuhammadNo ratings yet
- The Effects of Air Pollution and Temperature on COPD OutcomesDocument15 pagesThe Effects of Air Pollution and Temperature on COPD OutcomesWahyuNo ratings yet
- COPD Update LancetDocument52 pagesCOPD Update LancetlilydariniNo ratings yet
- (2247059X - Pneumologia) Asthma-COPD-Bronchiectasis Combination - An Unstudied TripletDocument3 pages(2247059X - Pneumologia) Asthma-COPD-Bronchiectasis Combination - An Unstudied TripletConstantin PopescuNo ratings yet
- Copd 1Document8 pagesCopd 1Meinita M.DNo ratings yet
- Chest: Cardiovascular Comorbidity in COPDDocument16 pagesChest: Cardiovascular Comorbidity in COPDAndry Wahyudi AgusNo ratings yet
- Assessment of Cardiovascular Changes Among Chronic Obstructive Pulmonary Disease Patients at Rural Tertiary Care Center of Northern IndiaDocument5 pagesAssessment of Cardiovascular Changes Among Chronic Obstructive Pulmonary Disease Patients at Rural Tertiary Care Center of Northern IndiaKarthik SNo ratings yet
- Gold Copd 2017Document4 pagesGold Copd 2017ChrisNo ratings yet
- Life 13 00459Document14 pagesLife 13 00459wulanesterNo ratings yet
- Copd 2019Document18 pagesCopd 2019Ella EllaNo ratings yet
- Cardiovascular Comorbidities in Chronic Obstructive Pulmonary Disease (COPD) - Current Considerations For Clinical PracticeDocument14 pagesCardiovascular Comorbidities in Chronic Obstructive Pulmonary Disease (COPD) - Current Considerations For Clinical Practicerbatjun576No ratings yet
- Reference 222Document7 pagesReference 222sabrinaNo ratings yet
- Osteo 2Document5 pagesOsteo 2Ardhyan ArdhyanNo ratings yet
- Mehu131 - U1 - T6 - Neurocysticercosis A Review of Current Status and ManagementDocument10 pagesMehu131 - U1 - T6 - Neurocysticercosis A Review of Current Status and ManagementGabriel OlivaresNo ratings yet
- Mehu131 U1 T6 NeurocysticercosisDocument16 pagesMehu131 U1 T6 NeurocysticercosisGabriel OlivaresNo ratings yet
- Mehu130 - U2 - T47 - AVANCES GENETICA EPOCDocument14 pagesMehu130 - U2 - T47 - AVANCES GENETICA EPOCGabriel OlivaresNo ratings yet
- Mehu131 - U1 - T6 - Clinical Symptoms, Diagnosis, and Treatment of NeuricysticercosisDocument14 pagesMehu131 - U1 - T6 - Clinical Symptoms, Diagnosis, and Treatment of NeuricysticercosisGabriel OlivaresNo ratings yet
- YesDocument10 pagesYesRabin SitumorangNo ratings yet
- Gold 2020 Report Ver1.0wmsDocument141 pagesGold 2020 Report Ver1.0wmsRoxana GonzalezNo ratings yet
- GINA 2019 Main Report June 2019 Wms PDFDocument201 pagesGINA 2019 Main Report June 2019 Wms PDFAndrada PredaNo ratings yet
- MEHU130 - U1 - T38 Epidemiology and Burden of Urinary Tract InfectionsDocument5 pagesMEHU130 - U1 - T38 Epidemiology and Burden of Urinary Tract InfectionsGabriel OlivaresNo ratings yet
- Clinical Practice Guidelines For The Antibiotic Treatment of Community-Acquired Urinary Tract InfectionsDocument34 pagesClinical Practice Guidelines For The Antibiotic Treatment of Community-Acquired Urinary Tract InfectionsdiasNo ratings yet
- 1-s2 0Document7 pages1-s2 0Anonymous 8k5cuCvOOYNo ratings yet
- Nuevas Cefalosporinas 2018 PDFDocument11 pagesNuevas Cefalosporinas 2018 PDFLud OleaNo ratings yet
- Neumonía IdsaDocument23 pagesNeumonía IdsaCarolina MoralesNo ratings yet
- 52-Article Text-219-2-10-20170628 PDFDocument6 pages52-Article Text-219-2-10-20170628 PDFGabriel OlivaresNo ratings yet
- Guide to alternative inhalers during shortagesDocument2 pagesGuide to alternative inhalers during shortagesDevs AbdouNo ratings yet
- Treatment - of - Asthma (TUSOM - Pharmwiki)Document20 pagesTreatment - of - Asthma (TUSOM - Pharmwiki)Angela Adobea TotiNo ratings yet
- Inhaler Chart 2016 PDFDocument2 pagesInhaler Chart 2016 PDFAlmas TalidaNo ratings yet
- Anoro Ellipta Pi MGDocument35 pagesAnoro Ellipta Pi MGAgusJiethoSfarmAptNo ratings yet
- GOLD 2011 Guideline SummaryDocument25 pagesGOLD 2011 Guideline SummaryebramnainggolanNo ratings yet
- Symbicort 80/4.5: Inhalation AerosolDocument14 pagesSymbicort 80/4.5: Inhalation AerosolAndrei MihaiNo ratings yet
- Status AsthmaticusDocument29 pagesStatus AsthmaticusDavid OlsonNo ratings yet
- Cardiovascular Safety of Long Acting Beta Agonist-Inhaled Corticosteroid Combination Products in Adult Patients With Asthma: A Systematic ReviewDocument8 pagesCardiovascular Safety of Long Acting Beta Agonist-Inhaled Corticosteroid Combination Products in Adult Patients With Asthma: A Systematic ReviewHaniifah Dhiya UlhaqNo ratings yet
- Asma Dalam KehamilanDocument33 pagesAsma Dalam KehamilanAnonymous wztrzkVnNo ratings yet
- Asthma & COPDDocument26 pagesAsthma & COPDraheenbushNo ratings yet
- Severe Asthma: Definition, Diagnosis and TreatmentDocument9 pagesSevere Asthma: Definition, Diagnosis and TreatmentHalim Muhammad SatriaNo ratings yet
- Asthma: Rochelle M. Nolte, MD CDR Usphs Family MedicineDocument56 pagesAsthma: Rochelle M. Nolte, MD CDR Usphs Family MedicineJoan Marie Lechado InoviaNo ratings yet
- New Treatments For Severe Treatment-Resistant Asthma - Lancet Resp Med 2013Document14 pagesNew Treatments For Severe Treatment-Resistant Asthma - Lancet Resp Med 2013Azan Al RasyidNo ratings yet
- Copd19 PDFDocument31 pagesCopd19 PDFAdinda Suci MaghfiraNo ratings yet
- Formoterol-Budesonide - EpdaDocument8 pagesFormoterol-Budesonide - EpdaAditya RounakNo ratings yet
- Drug Name Mechanism of Action Indication Contraindication Side Effects Nursing Responsibility Generic NameDocument4 pagesDrug Name Mechanism of Action Indication Contraindication Side Effects Nursing Responsibility Generic NameDan HizonNo ratings yet
- Asthma Control SABA UseDocument9 pagesAsthma Control SABA UsemapuxdNo ratings yet
- COPDSwissguidelinesDocument16 pagesCOPDSwissguidelinesNurul Kamilah SadliNo ratings yet
- The Medical Letter: On Drugs and TherapeuticsDocument11 pagesThe Medical Letter: On Drugs and TherapeuticsTom BiusoNo ratings yet
- Bronchial Asthma SeminarDocument64 pagesBronchial Asthma SeminarShidevNo ratings yet
- Breo ElliptaDocument11 pagesBreo ElliptamohammadNo ratings yet
- Abediterol (LAS100977), A Novel Long-Acting B - Agonist: Efficacy, Safety and Tolerability in Persistent AsthmaDocument6 pagesAbediterol (LAS100977), A Novel Long-Acting B - Agonist: Efficacy, Safety and Tolerability in Persistent AsthmaFi NoNo ratings yet
- Evaluating Triple ICS-LABA-LAMA and 2 CombinationDocument28 pagesEvaluating Triple ICS-LABA-LAMA and 2 CombinationharyatiNo ratings yet
- SMART Asthma TherapyDocument4 pagesSMART Asthma TherapyKen Won100% (1)
- SalmeterolDocument10 pagesSalmeterolArezoo JamNo ratings yet
- 9 18 Trelegy Ellipta Media Factsheet Final Approved 2Document3 pages9 18 Trelegy Ellipta Media Factsheet Final Approved 2Peter GálvezNo ratings yet
- Prescribing Patterns and Pharmacoeconomic Analysis of Drugs Used in Pediatric Asthma Patients at Tertiary Care HospitalDocument18 pagesPrescribing Patterns and Pharmacoeconomic Analysis of Drugs Used in Pediatric Asthma Patients at Tertiary Care Hospitalrajesh sumanNo ratings yet