You might also like
- Environmental Research: Jimyung Park, Hyung-Jun Kim, Chang-Hoon Lee, Chang Hyun Lee, Hyun Woo LeeDocument8 pagesEnvironmental Research: Jimyung Park, Hyung-Jun Kim, Chang-Hoon Lee, Chang Hyun Lee, Hyun Woo LeeJoaquim Lorenzetti BrancoNo ratings yet
- Do Inhaled Corticosteroids Protect Against Lung Cancer in Patients With COPD A Systematic ReviewDocument10 pagesDo Inhaled Corticosteroids Protect Against Lung Cancer in Patients With COPD A Systematic ReviewRicovially DavyaNo ratings yet
- Air Pollution As An Early Determinant of COPD: Zhuyi Lu, Patrice Coll, Bernard Maitre, Ralph Epaud and Sophie LanoneDocument13 pagesAir Pollution As An Early Determinant of COPD: Zhuyi Lu, Patrice Coll, Bernard Maitre, Ralph Epaud and Sophie LanoneywtmyxpezickztrkcfNo ratings yet
- Sarkar Et Al-2017-The Clinical Respiratory JournalDocument11 pagesSarkar Et Al-2017-The Clinical Respiratory JournalAntoninus HengkyNo ratings yet
- Air Pollution Exposure and Blood Pressure: An Updated Review of The LiteratureDocument24 pagesAir Pollution Exposure and Blood Pressure: An Updated Review of The LiteratureJackson LNo ratings yet
- Mehu130 - U2 - T47 - EPOC SeminarioDocument10 pagesMehu130 - U2 - T47 - EPOC SeminarioGabriel OlivaresNo ratings yet
- Work-Related Chronic Obstructive Pulmonary Disease (COPD) Statistics in Great Britain, 2020Document7 pagesWork-Related Chronic Obstructive Pulmonary Disease (COPD) Statistics in Great Britain, 2020Maral GanbilegNo ratings yet
- Chronic Obstructive Pulmonary Disease: Linking Outcomes and Pathobiology of Disease ModificationDocument5 pagesChronic Obstructive Pulmonary Disease: Linking Outcomes and Pathobiology of Disease ModificationAnonymous jbWresQ0lNo ratings yet
- Clinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary DiseaseDocument11 pagesClinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary DiseaseAgatha GeraldyneNo ratings yet
- Clinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary Disease-2Document11 pagesClinical Respiratory J - 2017 - Sarkar - Tuberculosis Associated Chronic Obstructive Pulmonary Disease-2Adistha Eka Noveyani,No ratings yet
- Chronic Bronchitis and COPDDocument11 pagesChronic Bronchitis and COPDRodli AkbarNo ratings yet
- Concise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseDocument10 pagesConcise Clinical Review: Chronic Bronchitis and Chronic Obstructive Pulmonary DiseaseMuhammad FakhruriNo ratings yet
- ComBat 2020-06-21 14 - 49 - 27Document23 pagesComBat 2020-06-21 14 - 49 - 27gfdsgefgijNo ratings yet
- 7ng-Triple Terapi & Risiko JantungDocument9 pages7ng-Triple Terapi & Risiko JantungsukiyantoNo ratings yet
- American Thoracic Society DocumentsDocument26 pagesAmerican Thoracic Society DocumentsGold4allNo ratings yet
- Hub TBC DG CopdDocument7 pagesHub TBC DG CopdAmalNo ratings yet
- An Association Between Air Pollution and MortalityDocument23 pagesAn Association Between Air Pollution and MortalityAna HerreraNo ratings yet
- HHS Public Access: Chronic Obstructive Pulmonary DiseaseDocument20 pagesHHS Public Access: Chronic Obstructive Pulmonary DiseaseafifahNo ratings yet
- COLE-HUNTER Long Term Air PollutionDocument10 pagesCOLE-HUNTER Long Term Air PollutionPaula VasconcellosNo ratings yet
- Osteo 2Document5 pagesOsteo 2Ardhyan ArdhyanNo ratings yet
- Update in EnvironmentalDocument6 pagesUpdate in EnvironmentalAidil Rahman NovesarNo ratings yet
- Hypertensionaha 116 07218Document9 pagesHypertensionaha 116 07218Nadhira KhairaniNo ratings yet
- Bronchite Chhronique 2022Document12 pagesBronchite Chhronique 2022Ella EllaNo ratings yet
- Contribution of Air Pollution To COPD and Small Airway DysfunctionDocument8 pagesContribution of Air Pollution To COPD and Small Airway DysfunctionWahyuNo ratings yet
- 1994 - Rusznak, Devalia, Davies - The Impact of Pollution On Allergic DiseaseDocument7 pages1994 - Rusznak, Devalia, Davies - The Impact of Pollution On Allergic DiseaseYOTIN JUPRASONGNo ratings yet
- GM 112Document10 pagesGM 112Thanasis PapatheodorouNo ratings yet
- Kwu 248Document9 pagesKwu 248NURUL ANIS AYUNI BINTI KHAIRUL ANUARNo ratings yet
- Pauwels 2004Document8 pagesPauwels 2004srichakadharsri911No ratings yet
- Chronic Bronchitis in West Sweden A Matter of Smoking and Social ClassDocument10 pagesChronic Bronchitis in West Sweden A Matter of Smoking and Social ClassTaro RahmatiaNo ratings yet
- Atm 09 05 390Document14 pagesAtm 09 05 390Adistha Eka Noveyani,No ratings yet
- 1 s2.0 S1877042810011444 Main PentingDocument9 pages1 s2.0 S1877042810011444 Main PentingEitavitaza Arzahzarah WillandNo ratings yet
- The Role of Cigarette Smoke-Induced Pulmonary Vascular Endothelial Cell Apoptosis in COPDDocument15 pagesThe Role of Cigarette Smoke-Induced Pulmonary Vascular Endothelial Cell Apoptosis in COPDAbeer SallamNo ratings yet
- COPD and StrokeDocument12 pagesCOPD and StrokeAndreea MoalesNo ratings yet
- EHP1699.altDocument11 pagesEHP1699.altkunkkonkNo ratings yet
- NatureDP 2015 Chronic Obstructive Pulmonary DiseaseDocument21 pagesNatureDP 2015 Chronic Obstructive Pulmonary DiseasePaloma GBNo ratings yet
- FullDocument10 pagesFullMuhammad SajidannorNo ratings yet
- Mechanistic Links Between COPD and Lung CancerDocument13 pagesMechanistic Links Between COPD and Lung CancerHoracioNo ratings yet
- COPDex Stroke 2017Document8 pagesCOPDex Stroke 2017Angelica ChavesNo ratings yet
- Christenson Stephanie A Chronic Obstructive PulmonaryDocument16 pagesChristenson Stephanie A Chronic Obstructive PulmonarynomokickNo ratings yet
- Tuberculosis Associated Chronic Obstructive Pulmonary DiseaseDocument12 pagesTuberculosis Associated Chronic Obstructive Pulmonary DiseaseinetNo ratings yet
- Small Airways Disease, A Condition in Which Small Bronchioles Are NarrowedDocument30 pagesSmall Airways Disease, A Condition in Which Small Bronchioles Are Narrowedanon_396086051No ratings yet
- (2247059X - Pneumologia) Asthma-COPD-Bronchiectasis Combination - An Unstudied TripletDocument3 pages(2247059X - Pneumologia) Asthma-COPD-Bronchiectasis Combination - An Unstudied TripletConstantin PopescuNo ratings yet
- Hubungan Intensitas Merokok Dan Kadar C-Reactive Protein Terhadap Penyakit Paru Obstruktif Kronis (PPOK)Document7 pagesHubungan Intensitas Merokok Dan Kadar C-Reactive Protein Terhadap Penyakit Paru Obstruktif Kronis (PPOK)Triana virgaNo ratings yet
- Copd and CVD Pulmonology JournalDocument9 pagesCopd and CVD Pulmonology JournalKessi VikaneswariNo ratings yet
- Heal Briefing Air Serbia EngDocument4 pagesHeal Briefing Air Serbia EngSladjana TeslićNo ratings yet
- EPOC LancetDocument16 pagesEPOC LancetKarliux JimenezNo ratings yet
- Atm 04 08 160Document9 pagesAtm 04 08 160manalNo ratings yet
- Acute Exacerbation of COPD Is It The Stroke of The LungsDocument9 pagesAcute Exacerbation of COPD Is It The Stroke of The LungsBruna AlencarNo ratings yet
- Choudhury 2014Document30 pagesChoudhury 2014Andry Wahyudi AgusNo ratings yet
- Cellular and Molecular Mechanisms of Asthma and COPDDocument18 pagesCellular and Molecular Mechanisms of Asthma and COPDMihaela BerindeieNo ratings yet
- COPD As An Endothelial Disorder Endothelial Injury LinkingDocument18 pagesCOPD As An Endothelial Disorder Endothelial Injury LinkingAndreea MoalesNo ratings yet
- HHS Public Access: Air Pollution, Oxidative Stress, and Diabetes: A Life Course Epidemiologic PerspectiveDocument18 pagesHHS Public Access: Air Pollution, Oxidative Stress, and Diabetes: A Life Course Epidemiologic PerspectiveKikiaraNo ratings yet
- Pollution and Respiratory Disease: Can Diet or Supplements Help? A ReviewDocument14 pagesPollution and Respiratory Disease: Can Diet or Supplements Help? A ReviewEgy SunandaNo ratings yet
- 1056 FullDocument10 pages1056 Fullrulitos000No ratings yet
- Therefore Proper and Early Management of COPD Is NeededDocument11 pagesTherefore Proper and Early Management of COPD Is NeededAwliyatul FitriyahNo ratings yet
- Manifestaciones Sistemicas EPOCDocument9 pagesManifestaciones Sistemicas EPOCAlejandra OrtegaNo ratings yet
- Taking A Stand Against Air Pollution - The Impact On Cardiovascular DiseaseDocument6 pagesTaking A Stand Against Air Pollution - The Impact On Cardiovascular Diseasepao.pearanda1998No ratings yet
- Spleen Removal Surgery Breakthrough by SlidesgoDocument40 pagesSpleen Removal Surgery Breakthrough by SlidesgoWahyuNo ratings yet
- Jawaban BoyDocument4 pagesJawaban BoyWahyuNo ratings yet
- 3D Printed Bone Models in Oral and Cranio-Maxillofacial Surgery: A Systematic ReviewDocument19 pages3D Printed Bone Models in Oral and Cranio-Maxillofacial Surgery: A Systematic ReviewWahyuNo ratings yet
- Prevalence, Pattern, Etiology, and Management of Maxillofacial TraumaDocument8 pagesPrevalence, Pattern, Etiology, and Management of Maxillofacial TraumaWahyuNo ratings yet
- Diagnosis Akut Abdomen Akibat Peritonitis: Amalita Mananna', Stephanus J. Ch. Tangel, Eko PrasetyoDocument7 pagesDiagnosis Akut Abdomen Akibat Peritonitis: Amalita Mananna', Stephanus J. Ch. Tangel, Eko PrasetyoAvika MuharrahmahNo ratings yet
- Chapter 23the Multiply & Severely Injured PatientDocument19 pagesChapter 23the Multiply & Severely Injured PatientWahyuNo ratings yet
- Trauma Maksilofacial 63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma MaksilofacialDocument7 pagesTrauma Maksilofacial 63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma Maksilofacial63423246 Trauma MaksilofacialChristian SolihinNo ratings yet
- Epidemiology of Facial Fractures: Incidence, Prevalence and Years Lived With Disability Estimates From The Global Burden of Disease 2017 StudyDocument9 pagesEpidemiology of Facial Fractures: Incidence, Prevalence and Years Lived With Disability Estimates From The Global Burden of Disease 2017 StudyWahyuNo ratings yet
- Maxillofacial Trauma in The Emergency Department: Pearls and Pitfalls in Airway ManagementDocument13 pagesMaxillofacial Trauma in The Emergency Department: Pearls and Pitfalls in Airway ManagementWahyuNo ratings yet
- Contribution of Air Pollution To COPD and Small Airway DysfunctionDocument8 pagesContribution of Air Pollution To COPD and Small Airway DysfunctionWahyuNo ratings yet
- Maxillofacial Trauma (Facial)Document8 pagesMaxillofacial Trauma (Facial)Anonymous LnWIBo1GNo ratings yet
- Karakteristik Penderita Asma Bronkial Dewasa Yang Dirawat Inap Di RSUP H. Adam Malik Medan Tahun 2014-2015Document10 pagesKarakteristik Penderita Asma Bronkial Dewasa Yang Dirawat Inap Di RSUP H. Adam Malik Medan Tahun 2014-2015WahyuNo ratings yet
- Hubungan Facial Injury Severity Scale Dengan Lama Rawat Inap Pasien Trauma MaksilofasialDocument5 pagesHubungan Facial Injury Severity Scale Dengan Lama Rawat Inap Pasien Trauma MaksilofasialDwi PascawitasariNo ratings yet
- Jcem 0739Document9 pagesJcem 0739WahyuNo ratings yet
- ALFREDO 22010112130140 Lap - KTI Bab7Document19 pagesALFREDO 22010112130140 Lap - KTI Bab7titikNo ratings yet
- Jawaban Si BoyDocument2 pagesJawaban Si BoyWahyuNo ratings yet
- JurnakDocument14 pagesJurnakWindy MasengiNo ratings yet
- Mantap GuysDocument14 pagesMantap GuysWahyuNo ratings yet
- Jurnal Stapilokokus OsteomielitisDocument27 pagesJurnal Stapilokokus OsteomielitisWahyuNo ratings yet
- Asthma GuidelinesDocument12 pagesAsthma Guidelinesantr_patsNo ratings yet
- Karakteristik Penderita Asma Bronkial Dewasa Yang Dirawat Inap Di RSUP H. Adam Malik Medan Tahun 2014-2015Document10 pagesKarakteristik Penderita Asma Bronkial Dewasa Yang Dirawat Inap Di RSUP H. Adam Malik Medan Tahun 2014-2015WahyuNo ratings yet
- The Neuromuscular Junction.2Document4 pagesThe Neuromuscular Junction.2WahyuNo ratings yet
- Milling of Legume PulsesDocument7 pagesMilling of Legume Pulsessuresh100% (1)
- Yrc1000 Options InstructionsDocument36 pagesYrc1000 Options Instructionshanh nguyenNo ratings yet
- List of Medical Institutions Available For Foreign Language(s)Document24 pagesList of Medical Institutions Available For Foreign Language(s)leithNo ratings yet
- Computer Systems Servicing NC II CGDocument238 pagesComputer Systems Servicing NC II CGRickyJeciel100% (2)
- Times Leader 06-13-2013Document42 pagesTimes Leader 06-13-2013The Times LeaderNo ratings yet
- Promax Reference PDFDocument32 pagesPromax Reference PDFfarkli88No ratings yet
- ERP and Oracle E-Business Suite ConceptsDocument73 pagesERP and Oracle E-Business Suite ConceptsAlaa Mostafa100% (1)
- Architecture Design Planning Undergraduate Postgraduate Guide 2018Document52 pagesArchitecture Design Planning Undergraduate Postgraduate Guide 2018Jack LinNo ratings yet
- Mulberry VarietiesDocument24 pagesMulberry VarietiesKUNTAMALLA SUJATHANo ratings yet
- Reviewer MathDocument261 pagesReviewer MathMac Jayson DiazNo ratings yet
- 3HAC9821-1 Rev01Document8 pages3HAC9821-1 Rev01TensaigaNo ratings yet
- In-N-Out vs. DoorDashDocument16 pagesIn-N-Out vs. DoorDashEaterNo ratings yet
- Ease Us Fix ToolDocument7 pagesEase Us Fix ToolGregorio TironaNo ratings yet
- ReDocument3 pagesReSyahid FarhanNo ratings yet
- Axe FX II Tone Match ManualDocument6 pagesAxe FX II Tone Match Manualsteven monacoNo ratings yet
- FDD SRM & NDGDocument3 pagesFDD SRM & NDGEnd EndNo ratings yet
- Valuation of Bonds and Stocks: Financial Management Prof. Deepa IyerDocument49 pagesValuation of Bonds and Stocks: Financial Management Prof. Deepa IyerAahaanaNo ratings yet
- Bc-6800plus Series Auto Hematology Analyzer Operator's ManualDocument322 pagesBc-6800plus Series Auto Hematology Analyzer Operator's ManualHenock MelesseNo ratings yet
- ZF SI 6hp Family Tree enDocument2 pagesZF SI 6hp Family Tree enfercho573No ratings yet
- Impact of Child Labour On School Attendance and Academic Performance of Pupils in Public Primary Schools in Niger StateDocument90 pagesImpact of Child Labour On School Attendance and Academic Performance of Pupils in Public Primary Schools in Niger StateJaikes100% (3)
- Kaizenvest Education Report IndiaDocument62 pagesKaizenvest Education Report IndiaSakshi SodhiNo ratings yet
- Expansion Junction 1Document1 pageExpansion Junction 1kojjasNo ratings yet
- 1Document6 pages1Vignesh VickyNo ratings yet
- DWC Ordering InformationDocument15 pagesDWC Ordering InformationbalaNo ratings yet
- Sop Welder TigDocument2 pagesSop Welder TigShahid RazaNo ratings yet
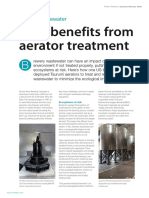
- Beer Benefits From Aerator TreatmentDocument2 pagesBeer Benefits From Aerator TreatmentSam MurrayNo ratings yet
- PDFs/Sprinker NFPA 13/plan Review Sprinkler Checklist 13Document5 pagesPDFs/Sprinker NFPA 13/plan Review Sprinkler Checklist 13isbtanwir100% (1)
- Jsa Camp Engine Service 350 HRSDocument1 pageJsa Camp Engine Service 350 HRSAdel AlKhedawyNo ratings yet
- Aegps Manual Fluxpower Hpi Installation enDocument44 pagesAegps Manual Fluxpower Hpi Installation enAbdus SalamNo ratings yet
- 2019 Book TheEBMTHandbookDocument688 pages2019 Book TheEBMTHandbook88tk6rccsmNo ratings yet