You might also like
- Set1 - Final FRCA Viva Qs - June 2009 PDFDocument25 pagesSet1 - Final FRCA Viva Qs - June 2009 PDFAdham SalemNo ratings yet
- Comprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFDocument530 pagesComprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFHaribabu ArumugamNo ratings yet
- Rodríguez-Monforte 2017 MS and Dietary PatternsDocument23 pagesRodríguez-Monforte 2017 MS and Dietary PatternsPaul SimononNo ratings yet
- Analysis: Dietary Guidelines and Health-Is Nutrition Science Up To The Task?Document9 pagesAnalysis: Dietary Guidelines and Health-Is Nutrition Science Up To The Task?Ainun RamadhantiNo ratings yet
- Ranasinghe Et Al, 2017Document9 pagesRanasinghe Et Al, 2017adi suputraNo ratings yet
- 2018 A Global Overview of Precision Medicine in Type 2 DiabetesDocument12 pages2018 A Global Overview of Precision Medicine in Type 2 Diabetesguanyulin01No ratings yet
- Nutrigenomics and Cardiovascular DiseaseDocument19 pagesNutrigenomics and Cardiovascular DiseaseAssignmentLab.comNo ratings yet
- Type 2 Diabetes: Annals of Internal MedicineDocument17 pagesType 2 Diabetes: Annals of Internal MedicinenicoolNo ratings yet
- The Impact of Physical Activity OnDocument7 pagesThe Impact of Physical Activity OnJudith Huarancca MariñoNo ratings yet
- From Nutrigenomics To Personalizing Diets: Are We Ready For Precision Medicine?Document2 pagesFrom Nutrigenomics To Personalizing Diets: Are We Ready For Precision Medicine?joeNo ratings yet
- Nmaa 108Document20 pagesNmaa 108fidya ardinyNo ratings yet
- Psychosocial Stress Induces Hyperphagia and Exacerbates Diet-Induced Insulin Resistance and The Manifestations of The Metabolic SyndromeDocument18 pagesPsychosocial Stress Induces Hyperphagia and Exacerbates Diet-Induced Insulin Resistance and The Manifestations of The Metabolic Syndromemariasr7No ratings yet
- PHD Thesis On Metabolic SyndromeDocument4 pagesPHD Thesis On Metabolic Syndromenlcnqrgld100% (2)
- PHD Thesis Metabolic SyndromeDocument5 pagesPHD Thesis Metabolic Syndromejanchampagnefargo100% (2)
- 2017 Article 540Document7 pages2017 Article 540venyNo ratings yet
- J. Nutr.-2016-Salas-Salvadó-jn.115.218487Document9 pagesJ. Nutr.-2016-Salas-Salvadó-jn.115.218487chiclebluejmNo ratings yet
- The Potential Role of Antioxidants in Metabolic Syndrome: Current Pharmaceutical Design December 2015Document12 pagesThe Potential Role of Antioxidants in Metabolic Syndrome: Current Pharmaceutical Design December 2015dr.martynchukNo ratings yet
- GLIM Malnutrition CriteriaDocument9 pagesGLIM Malnutrition CriteriaKarina AnggrenaniNo ratings yet
- Metabolic SyndromeDocument12 pagesMetabolic SyndromeMark AntoineNo ratings yet
- Kelompok 1 PDFDocument15 pagesKelompok 1 PDFristiaNo ratings yet
- Cardio Metabolic Risk in Individuals Prescribed Long Acting - 2019 - PsychiatryDocument7 pagesCardio Metabolic Risk in Individuals Prescribed Long Acting - 2019 - PsychiatryBelen MatteNo ratings yet
- Literature Review On Diabetes PDFDocument4 pagesLiterature Review On Diabetes PDFklbndecnd100% (1)
- Overweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisDocument12 pagesOverweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisLev FyodorNo ratings yet
- The Problem and It'S Background: World Health OrganizationDocument26 pagesThe Problem and It'S Background: World Health OrganizationGio LlanosNo ratings yet
- Nutrigenética, Nutrigenómica y ObesidadDocument50 pagesNutrigenética, Nutrigenómica y ObesidadYair BuenrostroNo ratings yet
- Exposicion Tx-ObesidadDocument16 pagesExposicion Tx-ObesidadMAURICIONo ratings yet
- Research ArticleDocument7 pagesResearch ArticleRicardo Joshua RojasNo ratings yet
- The Role of Diet in Multiple Sclerosis - A ReviewDocument16 pagesThe Role of Diet in Multiple Sclerosis - A ReviewHabib G. Moutran BarrosoNo ratings yet
- Targeting Ageing and Preventing Organ Degeneration With MetforminDocument7 pagesTargeting Ageing and Preventing Organ Degeneration With Metforminannisa habibullohNo ratings yet
- Supplementation With Okra Combined or Not With Exercise Training Is Able To Protect The Heart of Animals With Metabolic SyndromeDocument11 pagesSupplementation With Okra Combined or Not With Exercise Training Is Able To Protect The Heart of Animals With Metabolic SyndromeMoisés Felipe GomesNo ratings yet
- Obesidade - 11154 - 2023 - Article - 9829Document7 pagesObesidade - 11154 - 2023 - Article - 9829dbepplerNo ratings yet
- Research Essay Paper On DiabetesDocument6 pagesResearch Essay Paper On Diabetesluwahudujos3100% (1)
- Diet, A New Target To Prevent Depression?: BMC Medicine January 2013Document5 pagesDiet, A New Target To Prevent Depression?: BMC Medicine January 2013ARESS RIPNo ratings yet
- Risks and Benefits of Statins For Glucose Control Management of Type 2 Diabetes PatientsDocument11 pagesRisks and Benefits of Statins For Glucose Control Management of Type 2 Diabetes PatientspaulallenfileNo ratings yet
- The Prevalence of Metabolic Syndrome in Latin AmerDocument13 pagesThe Prevalence of Metabolic Syndrome in Latin AmercarolinaNo ratings yet
- Studiu 2018Document7 pagesStudiu 2018Catalina CalinNo ratings yet
- Current Treatments For Type 2 Diabetes, Their Side Effects and Possible Complementary TreatmentsDocument13 pagesCurrent Treatments For Type 2 Diabetes, Their Side Effects and Possible Complementary TreatmentsBianca GhibaNo ratings yet
- JOURNALDocument15 pagesJOURNALKirsten NVNo ratings yet
- Diet Soft Drink Consumption Is Associated With The Metabolic Syndrome: A Two Sample ComparisonDocument18 pagesDiet Soft Drink Consumption Is Associated With The Metabolic Syndrome: A Two Sample ComparisonPK MilkyNo ratings yet
- 10 1016@j Jacc 2017 11 011Document16 pages10 1016@j Jacc 2017 11 011Anita YolandhaNo ratings yet
- The Metabolic Syndrome: Time For A Critical AppraisalDocument16 pagesThe Metabolic Syndrome: Time For A Critical AppraisalprabhatguyNo ratings yet
- J Parenter Enteral Nutr - 2022 - Gressies - Nutrition Issues in The General Medical Ward Patient From General Screening ToDocument8 pagesJ Parenter Enteral Nutr - 2022 - Gressies - Nutrition Issues in The General Medical Ward Patient From General Screening ToRaiden EiNo ratings yet
- AyunoDocument8 pagesAyunoRaul DavilaNo ratings yet
- 1 s2.0 S0002822310014902 Main PDFDocument38 pages1 s2.0 S0002822310014902 Main PDFMr.GoneNo ratings yet
- Μάθημα 7 Παράδειγμα ΜεταανάλυσηςDocument93 pagesΜάθημα 7 Παράδειγμα ΜεταανάλυσηςΠόπη ΜποζίκηNo ratings yet
- Obesity A Review of Pathophysiology and Classific - 2023 - Mayo Clinic ProceediDocument16 pagesObesity A Review of Pathophysiology and Classific - 2023 - Mayo Clinic Proceedialerta.bfcmNo ratings yet
- USDA Grant Mattes 2001-2006Document6 pagesUSDA Grant Mattes 2001-2006The Nutrition CoalitionNo ratings yet
- Mehu131 U1 T6 Obesidad4Document16 pagesMehu131 U1 T6 Obesidad4Valeria Moretto VegaNo ratings yet
- Metabolic Syndrome Past Present and FutureDocument7 pagesMetabolic Syndrome Past Present and FutureLaura LizarazoNo ratings yet
- Association of Plasma Procalcitonin With Various Components of Metabolic Syndrome and Insulin ResistanceDocument13 pagesAssociation of Plasma Procalcitonin With Various Components of Metabolic Syndrome and Insulin ResistanceCentral Asian StudiesNo ratings yet
- اساليبDocument16 pagesاساليبAlshq AlshqNo ratings yet
- Perspective: Systems Biology of Metabolism: A Driver For Developing Personalized and Precision MedicineDocument8 pagesPerspective: Systems Biology of Metabolism: A Driver For Developing Personalized and Precision MedicineMauricio RíosNo ratings yet
- The Impact of Education and Age On Metabolic DisordersDocument20 pagesThe Impact of Education and Age On Metabolic DisordersAzahel RangelNo ratings yet
- Biomarkers in ObesityDocument6 pagesBiomarkers in ObesitydrmadankumarbnysNo ratings yet
- Trend of Nutrition Research in Endocrine Disorders, Gaps, and Future Plans A Collection of Experiences of An Endocrinology Research InstituteDocument8 pagesTrend of Nutrition Research in Endocrine Disorders, Gaps, and Future Plans A Collection of Experiences of An Endocrinology Research InstituteChawki MokademNo ratings yet
- 1 s2.0 S2001037021000751 Main PDFDocument27 pages1 s2.0 S2001037021000751 Main PDFغاز الشمالNo ratings yet
- Mona Mohamed Ibrahim Paper 13-12-2020Document19 pagesMona Mohamed Ibrahim Paper 13-12-2020mclinelkumahNo ratings yet
- AACE Diabetes Algorithm Executive 2016Document30 pagesAACE Diabetes Algorithm Executive 2016Luis Andres Carrero TovarNo ratings yet
- Food Ingredients and Suplements - Is This The FutureDocument2 pagesFood Ingredients and Suplements - Is This The FutureDonato CignoliNo ratings yet
- Slavin 2019Document16 pagesSlavin 2019dr.martynchukNo ratings yet
- Jcem 2952Document9 pagesJcem 2952parta anantamaNo ratings yet
- Funda Vital SignsDocument63 pagesFunda Vital SignsElia Saph MoonNo ratings yet
- Renovascular Hypertension: Department of Vascular Interventional Radiology Kem HospitalDocument45 pagesRenovascular Hypertension: Department of Vascular Interventional Radiology Kem Hospitalamrita narangNo ratings yet
- NCM 106A Nursing Pharmacology: Reflection PaperDocument2 pagesNCM 106A Nursing Pharmacology: Reflection PaperKristil ChavezNo ratings yet
- 1 s2.0 S0022282816302176 MainDocument85 pages1 s2.0 S0022282816302176 MainNia Rukman100% (1)
- Junk Food: Impact On Health: Journal of Drug Delivery and Therapeutics May 2012Document8 pagesJunk Food: Impact On Health: Journal of Drug Delivery and Therapeutics May 2012Binte SajjadNo ratings yet
- Prevalence and Impact of Pain Among Older Adults in The United StatesDocument9 pagesPrevalence and Impact of Pain Among Older Adults in The United StatesLucas TarquiNo ratings yet
- Omron M6 Instruction ManualDocument24 pagesOmron M6 Instruction ManualsvigosNo ratings yet
- Factors Contributing To Emergence of Hypertension in Diabetic Patients Attending Diabetics Outpatient Clinic in Nyamira CountyDocument27 pagesFactors Contributing To Emergence of Hypertension in Diabetic Patients Attending Diabetics Outpatient Clinic in Nyamira CountyJoshua Mokaya100% (1)
- Concepts For Nursing Practice 3rd Edition Giddens Full-53-56Document4 pagesConcepts For Nursing Practice 3rd Edition Giddens Full-53-56هدوء النسمةNo ratings yet
- A Comparative Study of Relationship Between Vegetarians and Non-Vegetarians - Diet, Blood Pressure and Body Fat CompositionDocument3 pagesA Comparative Study of Relationship Between Vegetarians and Non-Vegetarians - Diet, Blood Pressure and Body Fat CompositionmamtakumariNo ratings yet
- Rüthrich2021 Article COVID-19InCancerPatientsClinicDocument11 pagesRüthrich2021 Article COVID-19InCancerPatientsClinicdianaNo ratings yet
- HTN PPT - YasDocument18 pagesHTN PPT - YasCiaNo ratings yet
- Microvascular and Macrovascular Complications of Diabetes: Editor's Note: This Article Is The 6th in ADocument6 pagesMicrovascular and Macrovascular Complications of Diabetes: Editor's Note: This Article Is The 6th in AnadyaNo ratings yet
- Eng PDFDocument302 pagesEng PDFAnonymous YdFUaW6fBNo ratings yet
- Adhrence 1Document9 pagesAdhrence 1nabilahbilqisNo ratings yet
- Nursing 110 FinalDocument36 pagesNursing 110 FinalAngel Lopez100% (1)
- 7th March 2020 Plab 1 MockDocument32 pages7th March 2020 Plab 1 MockZoha QureshiNo ratings yet
- NCP - Acute PainDocument4 pagesNCP - Acute PainCharmin AlegreNo ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDeepakNo ratings yet
- Chronic Kidney Disease in Homoeopathy Part-1Document31 pagesChronic Kidney Disease in Homoeopathy Part-1Tarique ImamNo ratings yet
- 2008.clin Chem - RantnerDocument7 pages2008.clin Chem - RantnertwkangNo ratings yet
- Nclex Med For NursesDocument24 pagesNclex Med For NursesSoleil Angeline Díaz77% (13)
- Regulation of Blood Pressure - 2Document38 pagesRegulation of Blood Pressure - 2vikrant gholapNo ratings yet
- EpitensDocument2 pagesEpitensmahgadNo ratings yet
- Prepregnancy Counseling NoprintDocument11 pagesPrepregnancy Counseling NoprintDo le QuangNo ratings yet
- Spot MapDocument28 pagesSpot MapCarrie Joy DecalanNo ratings yet
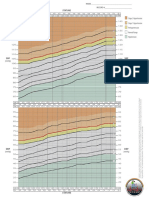
- BP Chart Girls Color WideDocument1 pageBP Chart Girls Color WidealbertNo ratings yet
- Hypertensive Disorders in PregnancyDocument10 pagesHypertensive Disorders in PregnancyRwabugili ChrisNo ratings yet