You might also like
- (David Weinstock) NeuroKinetic Therapy An InnovatDocument151 pages(David Weinstock) NeuroKinetic Therapy An Innovatvioly100% (2)
- PHYSIOLOGY - The Case of The Unlucky HikerDocument2 pagesPHYSIOLOGY - The Case of The Unlucky HikerAnonymous s2jaDmP5F100% (1)
- 1.12 Gluteal Region and Posterior Thigh Compartment PDFDocument5 pages1.12 Gluteal Region and Posterior Thigh Compartment PDFJuliaNo ratings yet
- Athletes Book of Home RemediesDocument375 pagesAthletes Book of Home RemediesLynsey100% (1)
- Comminuted Patella FracturesDocument8 pagesComminuted Patella FracturesKirana lupitaNo ratings yet
- IT/IS Infrastructure ManagementDocument41 pagesIT/IS Infrastructure ManagementNarnishNo ratings yet
- The Meniscus in Kne e Osteoarthritis: Martin Englund,, Ali Guermazi,, L. Stefan LohmanderDocument12 pagesThe Meniscus in Kne e Osteoarthritis: Martin Englund,, Ali Guermazi,, L. Stefan LohmanderNati GallardoNo ratings yet
- 3 Column AnkleDocument8 pages3 Column AnkleJosé Eduardo Fernandez RodriguezNo ratings yet
- Aaos TraumaDocument59 pagesAaos Traumaidris tajouryNo ratings yet
- Flexion: To Improve Movement of The PivotalDocument3 pagesFlexion: To Improve Movement of The PivotalKelsey MacaraigNo ratings yet
- Surgical Techniques For Complex Proximal Tibial FracturesDocument13 pagesSurgical Techniques For Complex Proximal Tibial FracturesHannah CoNo ratings yet
- Richard Tan - Master Tung Points Lecture Notes Part 2Document69 pagesRichard Tan - Master Tung Points Lecture Notes Part 2Susana Oliveira100% (3)
- Applied Anatomy of Joints BY DR Iram Iqbal, PG Trainee, M Phill, AnatomyDocument89 pagesApplied Anatomy of Joints BY DR Iram Iqbal, PG Trainee, M Phill, Anatomyimmmi100% (3)
- Sclerotherapy: Treatment of Varicose Telangiectatic Leg VeinsDocument439 pagesSclerotherapy: Treatment of Varicose Telangiectatic Leg VeinsjesussalvadorsuazaNo ratings yet
- Pediatric Triplane Ankle Fractures Impact of Radiographs and Computed Tomography On Fracture Classification and Treatment Planning.Document8 pagesPediatric Triplane Ankle Fractures Impact of Radiographs and Computed Tomography On Fracture Classification and Treatment Planning.Alejandro Godoy SaidNo ratings yet
- 3 Columnas Acetabulares ClasificaiconDocument11 pages3 Columnas Acetabulares Clasificaiconlriveros540No ratings yet
- The Incidence of Posterior Tibial Plateau Fracture: An Investigation of 525 Fractures by Using A CT-based Classification SystemDocument6 pagesThe Incidence of Posterior Tibial Plateau Fracture: An Investigation of 525 Fractures by Using A CT-based Classification SystemJuan GomezNo ratings yet
- Analysis and Improvement of The Three-Column Spinal Theory: Researcharticle Open AccessDocument12 pagesAnalysis and Improvement of The Three-Column Spinal Theory: Researcharticle Open Accesssanzhez12raulNo ratings yet
- 1999 AhnDocument7 pages1999 Ahnosama-alaliNo ratings yet
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDocument8 pagesNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanNo ratings yet
- Ijcmsr 312 v1Document7 pagesIjcmsr 312 v1AshliiqueNo ratings yet
- Pelvic Fractures - Experience of Pelvic Ring Fractures at A Major Trauma CentreDocument8 pagesPelvic Fractures - Experience of Pelvic Ring Fractures at A Major Trauma CentreFatrika DewiNo ratings yet
- Cole 2013Document5 pagesCole 2013Angie MorrisNo ratings yet
- Plantillo Anteromedial + LCP + ApeDocument7 pagesPlantillo Anteromedial + LCP + ApeThiagoNo ratings yet
- Evaluation of Ankle Fracture Classification Systems in 193 Trimalleolar Ankle FracturesDocument8 pagesEvaluation of Ankle Fracture Classification Systems in 193 Trimalleolar Ankle Fracturesmaria jose tapia petitNo ratings yet
- Art3a10 10072fs00256-014-1842-5Document9 pagesArt3a10 10072fs00256-014-1842-5api-253958760No ratings yet
- Em Editorial Commentary em The Segond FractureDocument3 pagesEm Editorial Commentary em The Segond FractureVinod kumarNo ratings yet
- 2309499017692700Document5 pages2309499017692700calinNo ratings yet
- 3 ColumnasDocument4 pages3 ColumnasGabriel CadenaNo ratings yet
- Acute Posterior Cruciate Ligament Injuries: Effect of Location, Severity, and Associated Injuries On Surgical ManagementDocument10 pagesAcute Posterior Cruciate Ligament Injuries: Effect of Location, Severity, and Associated Injuries On Surgical Managementshabrina nurafiatiNo ratings yet
- Neer Classification - How Do We Use It and Why Is It Important?Document46 pagesNeer Classification - How Do We Use It and Why Is It Important?endy ahmaruzamryNo ratings yet
- OSRM ProximalDocument9 pagesOSRM ProximalÂngelo Rosso LlantadaNo ratings yet
- Anatomy of Pilon Fractures of The Distal Tibia: TraumaDocument6 pagesAnatomy of Pilon Fractures of The Distal Tibia: TraumaaiakobyNo ratings yet
- A Crescent-Shaped Juxtafacet Cyst As A Rare Cause of High Thoracic Myelopathy With Partial Brown-Séquard's SyndromeDocument3 pagesA Crescent-Shaped Juxtafacet Cyst As A Rare Cause of High Thoracic Myelopathy With Partial Brown-Séquard's Syndromeg9dhczvdjxNo ratings yet
- OTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be DoneDocument6 pagesOTA Highlight Paper Predicting Future Displacement of Nonoperatively Managed Lateral Compression Sacral Fractures - Can It Be Doneakb601No ratings yet
- Articulo Cone BeanDocument9 pagesArticulo Cone Beanernesto chavez ruizNo ratings yet
- A 3-Dimensional Finite-Element Analysis Investigating The Biomechanical Behavior of The Mandible and Plate Osteosynthesis in Cases of Fractures of The Condylar ProcessDocument9 pagesA 3-Dimensional Finite-Element Analysis Investigating The Biomechanical Behavior of The Mandible and Plate Osteosynthesis in Cases of Fractures of The Condylar Processhyl776210No ratings yet
- !!!sonographic Evaluation of Patellar Tendon DisplaceDocument8 pages!!!sonographic Evaluation of Patellar Tendon Displacecris weeNo ratings yet
- Pi Is 0363502317302241Document5 pagesPi Is 0363502317302241ashik MohamedNo ratings yet
- Rotator Cuff Tear: ImagingDocument7 pagesRotator Cuff Tear: ImagingAurelie VainNo ratings yet
- 26 Ijss Mar Oa26 - 2019Document5 pages26 Ijss Mar Oa26 - 2019Ravikiran NandirajuNo ratings yet
- Management of The Mangled ExtremityDocument10 pagesManagement of The Mangled ExtremityosteonectinNo ratings yet
- Fraktur Klavikula PDFDocument15 pagesFraktur Klavikula PDFSJ Iraa100% (1)
- Cantarella2018 DisyunciónDocument9 pagesCantarella2018 DisyunciónFernando Ruiz BorsiniNo ratings yet
- Orthodontic Therapy Using The Roth Gnathologic Approach. Freeland 2003Document13 pagesOrthodontic Therapy Using The Roth Gnathologic Approach. Freeland 2003Fernando Ruiz BorsiniNo ratings yet
- Rotator Cuff Tear Arthropathy: Pathophysiology, Imaging Characteristics, and Treatment OptionsDocument10 pagesRotator Cuff Tear Arthropathy: Pathophysiology, Imaging Characteristics, and Treatment OptionsYuni AngrianiNo ratings yet
- New Classification of Mandibular Asymmetry in Class III MalocclusionDocument27 pagesNew Classification of Mandibular Asymmetry in Class III MalocclusionkalixinNo ratings yet
- 3D Imaging of Residual Limbs Using UltrasoundDocument10 pages3D Imaging of Residual Limbs Using UltrasoundVivek IyerNo ratings yet
- Brief Resume of Intended WorkDocument7 pagesBrief Resume of Intended WorkNavin ChandarNo ratings yet
- MDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewDocument9 pagesMDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewcalinmariusNo ratings yet
- PIIS08Document8 pagesPIIS08Ahmad Ibrahim SalemNo ratings yet
- New Classification System ForDocument12 pagesNew Classification System ForJaviera Paz HerreraNo ratings yet
- Comparison of Iliac Crest Versus Supraacetabular External FixatorDocument7 pagesComparison of Iliac Crest Versus Supraacetabular External FixatortripodegrandeNo ratings yet
- 2017 Article 566Document10 pages2017 Article 566abdo houamerNo ratings yet
- Stress Changes of Lateral Collateral Ligament at Different Knee Flexion With or Without Displaced Movements: A 3-Dimensional Finite Element AnalysisDocument5 pagesStress Changes of Lateral Collateral Ligament at Different Knee Flexion With or Without Displaced Movements: A 3-Dimensional Finite Element AnalysisastritriNo ratings yet
- C. Gerber - Arthroscopic Correction of The Critical Shoulder Angle Through Lateral Acromioplasty A Safe Adjunct To Rotator Cuff Repair (2017)Document10 pagesC. Gerber - Arthroscopic Correction of The Critical Shoulder Angle Through Lateral Acromioplasty A Safe Adjunct To Rotator Cuff Repair (2017)João Pedro ZenattoNo ratings yet
- Clinical BiomechanicsDocument7 pagesClinical BiomechanicsAngélica Luna AyalaNo ratings yet
- The Accuracy of Positioning of A Custom-Made Implant Within A Large Acetabular Defect at Revision Arthroplasty of The HipDocument6 pagesThe Accuracy of Positioning of A Custom-Made Implant Within A Large Acetabular Defect at Revision Arthroplasty of The HipIrina DesyatykhNo ratings yet
- Achot 2012 6 473 483Document11 pagesAchot 2012 6 473 483LuisAngelPonceTorresNo ratings yet
- Forces - Medial Meniscal - 3DDocument26 pagesForces - Medial Meniscal - 3DmtwakadNo ratings yet
- Chahla 2018Document9 pagesChahla 2018Miguel Angel Lamas RamirezNo ratings yet
- Biomechanical RationaleDocument10 pagesBiomechanical RationalekhudecNo ratings yet
- Oral and Maxillofacial Radiology: Editor: Stephen R. MattesonDocument9 pagesOral and Maxillofacial Radiology: Editor: Stephen R. MattesonLiz StephanyNo ratings yet
- PengDocument10 pagesPengBarath NMNo ratings yet
- Displaced Acetabular FracturesDocument11 pagesDisplaced Acetabular FracturesJayNo ratings yet
- A Reliable Radiographic Measurement Technique ForDocument9 pagesA Reliable Radiographic Measurement Technique ForjemierudyanNo ratings yet
- Distal Clavicle Fracture Radiography and Treatment: A Pictorial EssayDocument9 pagesDistal Clavicle Fracture Radiography and Treatment: A Pictorial EssayAdella Maharani SNo ratings yet
- Complex and Revision Shoulder Arthroplasty: An Evidence-Based Approach to Evaluation and ManagementFrom EverandComplex and Revision Shoulder Arthroplasty: An Evidence-Based Approach to Evaluation and ManagementRobert Z. TashjianNo ratings yet
- Tips and Tricks for Problem Fractures, Volume I: The Upper ExtremityFrom EverandTips and Tricks for Problem Fractures, Volume I: The Upper ExtremityDaniel S. HorwitzNo ratings yet
- BenchmarkingDocument14 pagesBenchmarkingNarnish100% (1)
- In-Press Article: Comparative Analysis of Mechanism-Associated 3-Dimensional Tibial Plateau Fracture PatternsDocument9 pagesIn-Press Article: Comparative Analysis of Mechanism-Associated 3-Dimensional Tibial Plateau Fracture PatternsNarnishNo ratings yet
- IT Performance MeasurementsDocument49 pagesIT Performance MeasurementsNarnishNo ratings yet
- Structuring ItDocument21 pagesStructuring ItNarnishNo ratings yet
- IT Performance MeasurementsDocument49 pagesIT Performance MeasurementsNarnishNo ratings yet
- Reverensi Kuisioner Oswestry PDFDocument3 pagesReverensi Kuisioner Oswestry PDFagungary95No ratings yet
- Management of Perthes' Disease: SymposiumDocument8 pagesManagement of Perthes' Disease: SymposiumNarnishNo ratings yet
- Protocol Osteomielita BostonDocument6 pagesProtocol Osteomielita BostonAna VavuraNo ratings yet
- Information SystemsDocument17 pagesInformation SystemsNarnishNo ratings yet
- Business EnvironmentDocument32 pagesBusiness EnvironmentNarnishNo ratings yet
- Chapter 10: Arrays: Programming With Microsoft Visual BasicDocument47 pagesChapter 10: Arrays: Programming With Microsoft Visual BasicNarnishNo ratings yet
- Information SystemsDocument17 pagesInformation SystemsNarnishNo ratings yet
- Business and IT AlignmentDocument13 pagesBusiness and IT AlignmentNarnishNo ratings yet
- ClubfootDocument5 pagesClubfootcreyannc0% (1)
- Peroneus Longus Tendon Rupture: A Case Report: BackgroundDocument14 pagesPeroneus Longus Tendon Rupture: A Case Report: BackgroundAlgivar DaudNo ratings yet
- Must To Know Myologi Dan Topografi FKG 2021Document4 pagesMust To Know Myologi Dan Topografi FKG 2021NurfadilahNo ratings yet
- The Functional Anatomy of The Knee JointDocument12 pagesThe Functional Anatomy of The Knee JointFadzlee SoujiNo ratings yet
- Jospt 2018 7426Document9 pagesJospt 2018 7426Specializzandi FisiatriaNo ratings yet
- Tecnica Quirurgica PTG SygmaDocument58 pagesTecnica Quirurgica PTG SygmaDS JeanNo ratings yet
- 839 FullDocument5 pages839 Fullwinda athyaNo ratings yet
- Review Test: Directions: One-BestDocument8 pagesReview Test: Directions: One-BestFrederieNo ratings yet
- Plantar Fasciitis GuidelinesDocument19 pagesPlantar Fasciitis Guidelinesband12No ratings yet
- Medscimonit 25 7746Document9 pagesMedscimonit 25 7746sina dabiriNo ratings yet
- Effectiveness of Popular Race Walking DrillsDocument8 pagesEffectiveness of Popular Race Walking DrillsLukmanul HakimNo ratings yet
- AFO Orthometry FormDocument2 pagesAFO Orthometry Formmanjukumard2007No ratings yet
- Acl InjuriesDocument2 pagesAcl InjuriesFrnz RiveraNo ratings yet
- Top of The Foot Pain and Swelling TreatmentDocument13 pagesTop of The Foot Pain and Swelling TreatmentNyanLinKyawNo ratings yet
- The Obturator Nerve - Course - Motor - Sensory - TeachMeAnatomyDocument3 pagesThe Obturator Nerve - Course - Motor - Sensory - TeachMeAnatomyAreebaNo ratings yet
- Articulatio Genu: Posterior Aspects of Right Genu Lateral Aspects of Right GenuDocument5 pagesArticulatio Genu: Posterior Aspects of Right Genu Lateral Aspects of Right GenuindahkurNo ratings yet
- Popliteal Nerve BlockDocument3 pagesPopliteal Nerve BlockRatna Widiyanti KNo ratings yet
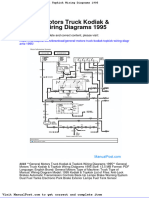
- General Motors Truck Kodiak Topkick Wiring Diagrams 1995Document23 pagesGeneral Motors Truck Kodiak Topkick Wiring Diagrams 1995emilycollins260586owp99% (134)
- Injuries of The Sporting KneeDocument3 pagesInjuries of The Sporting KneeDanar Hari AdhimuktiNo ratings yet
- Frog S Muscular System PDFDocument9 pagesFrog S Muscular System PDFVia CabardaNo ratings yet
- List of 100 Stretching ExercisesDocument4 pagesList of 100 Stretching ExercisesAmal SMNo ratings yet
- Hip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDDocument97 pagesHip Dislocations and Femoral Head Fractures: John T. Gorczyca, MDLassie LazyNo ratings yet