You might also like
- Joining Report: Annexure-IDocument14 pagesJoining Report: Annexure-Iharmeet454No ratings yet
- Change Request FormDocument1 pageChange Request FormhernadoyellowbirdNo ratings yet
- CRISPR Guide RNA Design: Methods and ProtocolsDocument287 pagesCRISPR Guide RNA Design: Methods and ProtocolsRch Chr100% (1)
- (Computerized) Employee Information Form (EIF) PDFDocument4 pages(Computerized) Employee Information Form (EIF) PDFAmanda SayfriedNo ratings yet
- 07 Laboratory Exercise 1 - Rodas, JessieDocument5 pages07 Laboratory Exercise 1 - Rodas, JessieJessie RodasNo ratings yet
- Ayaz Khaja JavaDocument6 pagesAyaz Khaja JavaSanya RastogiNo ratings yet
- Low-Code/No-Code: Citizen Developers and the Surprising Future of Business ApplicationsFrom EverandLow-Code/No-Code: Citizen Developers and the Surprising Future of Business ApplicationsRating: 2.5 out of 5 stars2.5/5 (2)
- Without GI Confirmation and Without Confirmation GR Is Not Possible - SAP Blogs PDFDocument6 pagesWithout GI Confirmation and Without Confirmation GR Is Not Possible - SAP Blogs PDFVigneshNo ratings yet
- VMware vSAN 8 Administration GuideDocument145 pagesVMware vSAN 8 Administration GuidevElements Dot NetNo ratings yet
- dll-EmTech Week 6Document4 pagesdll-EmTech Week 6Richard BaysicNo ratings yet
- A Technical Excellence Framework for Innovative Digital Transformation LeadershipFrom EverandA Technical Excellence Framework for Innovative Digital Transformation LeadershipRating: 5 out of 5 stars5/5 (1)
- Fm-Sds-Ict-001 Rev 01 Ict Technical Assistance (Ta) Form-EditableDocument2 pagesFm-Sds-Ict-001 Rev 01 Ict Technical Assistance (Ta) Form-EditableAlvin Agonoy NovencidoNo ratings yet
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesAriane Ace de GuzmanNo ratings yet
- Schools Division Office of Isabela: Department of Education Region 02 (Cagayan Valley)Document1 pageSchools Division Office of Isabela: Department of Education Region 02 (Cagayan Valley)Myra Dacquil AlingodNo ratings yet
- Ict Unit Technical Assistance (Ta) Form: Client InformationDocument1 pageIct Unit Technical Assistance (Ta) Form: Client InformationMia ManaayNo ratings yet
- Schools Division Office of IsabelaDocument2 pagesSchools Division Office of IsabelaEdgar Senense CariagaNo ratings yet
- Department of Education: (If Recipient Pls. Check)Document3 pagesDepartment of Education: (If Recipient Pls. Check)Ice JimenezNo ratings yet
- It Work RequestDocument1 pageIt Work RequeststevanologorNo ratings yet
- ELCINA Membership Form Feb2021Document3 pagesELCINA Membership Form Feb2021aby mani AbrahamNo ratings yet
- DCP & DICP School Survey and Monitoring ChecklistDocument3 pagesDCP & DICP School Survey and Monitoring ChecklistJoelle M. CruzNo ratings yet
- Recipient of DCP Survey and Monitoring Checklist 1Document4 pagesRecipient of DCP Survey and Monitoring Checklist 1Rodjone BinondoNo ratings yet
- Application For Technical Certification: California Water Environment AssociationDocument9 pagesApplication For Technical Certification: California Water Environment AssociationfooNo ratings yet
- ELCINA Membership Form 08feb2022Document3 pagesELCINA Membership Form 08feb2022Anil teaserNo ratings yet
- Government Internship Program (Gip) & Immersion Outreach Program (Iop)Document3 pagesGovernment Internship Program (Gip) & Immersion Outreach Program (Iop)Fhaiyne Aresgado LptNo ratings yet
- DCP Monitoring Report With HeaderDocument3 pagesDCP Monitoring Report With HeaderGerald MaimadNo ratings yet
- Issp CoverDocument2 pagesIssp CoverEliza CabugawanNo ratings yet
- ICT Service Request FormDocument1 pageICT Service Request FormkarebumussaNo ratings yet
- MBTB Application FormDocument3 pagesMBTB Application FormShekhar ShravagiNo ratings yet
- Sparx - Regform - 2Document2 pagesSparx - Regform - 2Priyanka ChowdaryNo ratings yet
- NLC-IAF-2016 National Logistic Cell Internship Application Form 2016Document4 pagesNLC-IAF-2016 National Logistic Cell Internship Application Form 2016Faisal AminNo ratings yet
- Msme Tool Room, Indore: Bio-DataDocument2 pagesMsme Tool Room, Indore: Bio-DataaviralNo ratings yet
- F Reg 304Document1 pageF Reg 304Nino Dave BauzonNo ratings yet
- Adopt A School FormDocument9 pagesAdopt A School FormRubina Fallorina Ozo100% (1)
- Adpro Prelim ExamDocument4 pagesAdpro Prelim Examlemuel sardualNo ratings yet
- Pece Checklist Updated As of Mar 11, 2015Document9 pagesPece Checklist Updated As of Mar 11, 2015Dennis ANo ratings yet
- Department of Electrical Engineering: Final Year Project ProposalDocument7 pagesDepartment of Electrical Engineering: Final Year Project ProposalAttique RehmanNo ratings yet
- Group Personal Data FormDocument8 pagesGroup Personal Data FormwhitenegroNo ratings yet
- Attachment Return FormDocument2 pagesAttachment Return FormRarry JohnsonNo ratings yet
- Job Application PDFDocument3 pagesJob Application PDFSilar BashaNo ratings yet
- FRM It 01 01 It Maintenance Form Rev01Document1 pageFRM It 01 01 It Maintenance Form Rev01rowlandNo ratings yet
- Activity PermitDocument2 pagesActivity PermitEarl TrinidadNo ratings yet
- Registration Form For InternshipDocument1 pageRegistration Form For InternshipSalman BaigNo ratings yet
- Application Form - EhsDocument2 pagesApplication Form - EhsmhelNo ratings yet
- Application Form: Tel Nos.: (086) 211-3901 Cel. No.: 09478919411Document1 pageApplication Form: Tel Nos.: (086) 211-3901 Cel. No.: 09478919411Rheeya PerezNo ratings yet
- DCP Issues and ConcernsDocument1 pageDCP Issues and ConcernsLeu NameNo ratings yet
- ISSP Cover Page PDFDocument9 pagesISSP Cover Page PDFMark Juan AbelonNo ratings yet
- Final Project Proposal Template (MUL)Document5 pagesFinal Project Proposal Template (MUL)Laiba KhanNo ratings yet
- Department of Education: Tablet/Laptop Borrower'S FormDocument2 pagesDepartment of Education: Tablet/Laptop Borrower'S FormMarilyn Cua DitchonNo ratings yet
- Indian Institute of Foreign Trade: Mba (International Business) : Part-TimeDocument4 pagesIndian Institute of Foreign Trade: Mba (International Business) : Part-TimeanimeshdevarshiNo ratings yet
- Certification Deferment of Installation of E-Classroom: Republic of The Philippines Department of EducationDocument1 pageCertification Deferment of Installation of E-Classroom: Republic of The Philippines Department of EducationElsa beljaminNo ratings yet
- Proof of Amateur ActivityDocument1 pageProof of Amateur ActivityRomeo MirandaNo ratings yet
- Ramanujan Computing Centre Anna University, CH: NNAI - 600 025Document3 pagesRamanujan Computing Centre Anna University, CH: NNAI - 600 025Ganesha KumarNo ratings yet
- Membership Record FormDocument1 pageMembership Record Formunc.aedNo ratings yet
- Progress Test 2Document5 pagesProgress Test 2Tiến NguyễnNo ratings yet
- Delnet Application FormDocument5 pagesDelnet Application FormKumara VelNo ratings yet
- Application For Graduation 005DDocument1 pageApplication For Graduation 005DBENIAL Shella Mae P.No ratings yet
- Indian Association of Structural Engineers: Application Form - Fellow/Member/Associate MemberDocument3 pagesIndian Association of Structural Engineers: Application Form - Fellow/Member/Associate Memberkhajarasool786No ratings yet
- Application For Local Council Funding: Form ADocument3 pagesApplication For Local Council Funding: Form AAnonymous RmzEd3jANo ratings yet
- F620 08ApplicationFormDocument4 pagesF620 08ApplicationFormstonedmountain95No ratings yet
- Business Plan TemplateDocument7 pagesBusiness Plan TemplatekakuararaNo ratings yet
- Egovernance Readiness Assessment Survey: I. Socio-Economic LandscapeDocument5 pagesEgovernance Readiness Assessment Survey: I. Socio-Economic LandscapeKris NuevaNo ratings yet
- Universal Testing Services: Staff Registration FormDocument4 pagesUniversal Testing Services: Staff Registration FormkalaNo ratings yet
- Universal Testing Services: Staff Registration FormDocument4 pagesUniversal Testing Services: Staff Registration FormkalaNo ratings yet
- Application Form 2018 19Document5 pagesApplication Form 2018 19Sujit KunduNo ratings yet
- June 4 Enrollment DataDocument504 pagesJune 4 Enrollment DataAlvin Agonoy NovencidoNo ratings yet
- Ict Technical Assistance (Ta) Form: Client InformationDocument1 pageIct Technical Assistance (Ta) Form: Client InformationAlvin Agonoy NovencidoNo ratings yet
- Melc NewDocument14 pagesMelc NewAlvin Agonoy NovencidoNo ratings yet
- References 12345Document4 pagesReferences 12345Alvin Agonoy NovencidoNo ratings yet
- Traditional Burmese MusicDocument8 pagesTraditional Burmese MusicAlvin Agonoy NovencidoNo ratings yet
- Outreach Project Proposal Format: Objective Activities Outputs Personnel BudgetDocument2 pagesOutreach Project Proposal Format: Objective Activities Outputs Personnel BudgetAlvin Agonoy NovencidoNo ratings yet
- Mark Louie T. Valdez Purok 1 Reina Mercedes Isabela Contact No#: 09756565150Document2 pagesMark Louie T. Valdez Purok 1 Reina Mercedes Isabela Contact No#: 09756565150Alvin Agonoy NovencidoNo ratings yet
- Carlo Fernandez Galam Purok 4 Lalog 1 Isabela Contact No#:09361097132Document3 pagesCarlo Fernandez Galam Purok 4 Lalog 1 Isabela Contact No#:09361097132Alvin Agonoy NovencidoNo ratings yet
- Franz Joseph Haydn (1732-1809) : Composer Fact SheetsDocument1 pageFranz Joseph Haydn (1732-1809) : Composer Fact SheetsAlvin Agonoy NovencidoNo ratings yet
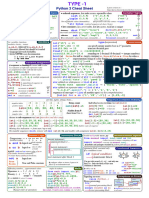
- Python Chee T SetDocument30 pagesPython Chee T SetkanuukNo ratings yet
- 11.position Ict Officer I Database Administration JSG 5Document2 pages11.position Ict Officer I Database Administration JSG 5abdifatah ibrahimNo ratings yet
- PA-00861 - SpaceLogic Zigbee Wireless Connectivity For EcoStruxure Building OperationDocument4 pagesPA-00861 - SpaceLogic Zigbee Wireless Connectivity For EcoStruxure Building OperationWalter BarbaNo ratings yet
- Windows 10 Availability For Xerox Fiery Servers: Why Upgrade To Windows 10?Document2 pagesWindows 10 Availability For Xerox Fiery Servers: Why Upgrade To Windows 10?XcopyNo ratings yet
- Fpa Australia - Ps 06 v1 Water Tanks For Fire Protection SystemsDocument11 pagesFpa Australia - Ps 06 v1 Water Tanks For Fire Protection Systemsyogesh0% (1)
- How To Update PAN Details On An Existing Zerodha Account?Document4 pagesHow To Update PAN Details On An Existing Zerodha Account?prasan bhandariNo ratings yet
- Lab Guide: Advanced Network Automation Solutions Using Cisco Ios EemDocument30 pagesLab Guide: Advanced Network Automation Solutions Using Cisco Ios EemResi Pramudyo PariwibowoNo ratings yet
- Computer Ethics: Living in IT EraDocument20 pagesComputer Ethics: Living in IT EraPatricia ReyesNo ratings yet
- Lab 3 Update and DeleteDocument7 pagesLab 3 Update and DeleteRheny BondocNo ratings yet
- 6277 How2useDocument2 pages6277 How2useNestor OyagaNo ratings yet
- Case Study: ARCON - User Behaviour Analytics (UBA) Predict - Protect - PreventDocument6 pagesCase Study: ARCON - User Behaviour Analytics (UBA) Predict - Protect - PreventPrasad KshirsagarNo ratings yet
- VNX - VNX 5100 Procedures-Replacing A 2U Power SupplyDocument25 pagesVNX - VNX 5100 Procedures-Replacing A 2U Power SupplyWei LeeNo ratings yet
- Linux Remote Access & AdministrationDocument10 pagesLinux Remote Access & AdministrationMrKey LordNo ratings yet
- Lab SparkDocument3 pagesLab SparkAymane BelhajeNo ratings yet
- DS Syllabus Question BankDocument3 pagesDS Syllabus Question BankKiran KumarNo ratings yet
- Products Variations and User Uploads - Part I: By: Muhammad Zeeshan AliDocument10 pagesProducts Variations and User Uploads - Part I: By: Muhammad Zeeshan Alisania ejazNo ratings yet
- Balaguru ExceptionDocument21 pagesBalaguru ExceptionKaustubh SaksenaNo ratings yet
- IManager NetEco 1000S Product DescriptionDocument16 pagesIManager NetEco 1000S Product DescriptionLambert LambrintoNo ratings yet
- ADV-JAVA by Ramchandra New (Update1)Document555 pagesADV-JAVA by Ramchandra New (Update1)Akash NaikNo ratings yet
- CommuteEZY - Manuscript REVISEDDocument6 pagesCommuteEZY - Manuscript REVISEDMavoori AkhilNo ratings yet
- Bbih4103 - International Human Resource ManagementDocument8 pagesBbih4103 - International Human Resource ManagementSimon RajNo ratings yet
- Fundamentals of SchedulingDocument8 pagesFundamentals of SchedulingAndrew UgohNo ratings yet
- Dell Vostro 1000 System BIOSDocument5 pagesDell Vostro 1000 System BIOSillusion_imranNo ratings yet
- ZTE IEnergy ElasticNet UME System Product DescriptionDocument13 pagesZTE IEnergy ElasticNet UME System Product DescriptionSara OmranNo ratings yet