You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Oo-Bmomeom: Certificate of Liability InsuranceDocument1 pageOo-Bmomeom: Certificate of Liability InsuranceMon DoceNo ratings yet
- 1st EvalsDocument20 pages1st EvalsMon DoceNo ratings yet
- Case 1 ManagementDocument1 pageCase 1 ManagementMon DoceNo ratings yet
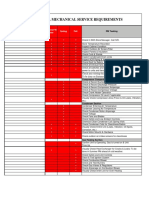
- Aspen Dental Mechanical Service Requirements: NotesDocument2 pagesAspen Dental Mechanical Service Requirements: NotesMon DoceNo ratings yet
- 5 6109582981330895076Document5 pages5 6109582981330895076Mon DoceNo ratings yet
- Theoretical Framework DesignDocument3 pagesTheoretical Framework DesignMon DoceNo ratings yet
- Objective TreeDocument1 pageObjective TreeMon DoceNo ratings yet
- Quiz 1Document41 pagesQuiz 1Mon DoceNo ratings yet
- Volvulus: Carol K. Le Phillip Nahirniak Sachit Anand Wantzy Cooper. Author InformationDocument22 pagesVolvulus: Carol K. Le Phillip Nahirniak Sachit Anand Wantzy Cooper. Author InformationMon DoceNo ratings yet
- Type of FeedingDocument1 pageType of FeedingMon DoceNo ratings yet
- Sundown Quizzes PNLE 2018Document42 pagesSundown Quizzes PNLE 2018Mon DoceNo ratings yet
- Clinical Summary (Dr. Yaoyao Meds)Document2 pagesClinical Summary (Dr. Yaoyao Meds)Mon DoceNo ratings yet
- Davao Medical School Foundation Inc. College of MidwiferyDocument2 pagesDavao Medical School Foundation Inc. College of MidwiferyMon DoceNo ratings yet
- (Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Document1 page(Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Mon DoceNo ratings yet
- Your Patient Today Will Be Sheny DredDocument6 pagesYour Patient Today Will Be Sheny DredMon DoceNo ratings yet
- Clinical Summary (Dr. Yaoyao Meds)Document2 pagesClinical Summary (Dr. Yaoyao Meds)Mon DoceNo ratings yet
- CaseDocument1 pageCaseMon DoceNo ratings yet
- Quiz EndocrineDocument16 pagesQuiz EndocrineMon DoceNo ratings yet
- Quiz EndocrineDocument16 pagesQuiz EndocrineMon DoceNo ratings yet
- Quiz 1Document41 pagesQuiz 1Mon DoceNo ratings yet
- Sundown Quizzes PNLE 2018Document42 pagesSundown Quizzes PNLE 2018Mon DoceNo ratings yet
- (Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Document1 page(Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Mon DoceNo ratings yet
- Davao Medical School Foundation Department of Obstetrics and Gynecology APRIL 24, 2020 TOPIC: 25 Year-Old With AMENORRHEA (Student's Copy)Document11 pagesDavao Medical School Foundation Department of Obstetrics and Gynecology APRIL 24, 2020 TOPIC: 25 Year-Old With AMENORRHEA (Student's Copy)Mon DoceNo ratings yet
- Your Patient Today Will Be Sheny DredDocument6 pagesYour Patient Today Will Be Sheny DredMon DoceNo ratings yet
- CaseDocument1 pageCaseMon DoceNo ratings yet
- SDASSDSADSADDocument2 pagesSDASSDSADSADMon DoceNo ratings yet
- Neonatal ResuscitationDocument4 pagesNeonatal ResuscitationMon DoceNo ratings yet
- Notes On Common Pediatric Drugs, Dosaging and Package: For FeverDocument1 pageNotes On Common Pediatric Drugs, Dosaging and Package: For FeverMon DoceNo ratings yet
- Mon Doce Online Exam 1Document43 pagesMon Doce Online Exam 1Mon DoceNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nursing Assessment in Family Nursing PracticeDocument22 pagesNursing Assessment in Family Nursing PracticeHydra Olivar - PantilganNo ratings yet
- Shoshana Bulka PragmaticaDocument17 pagesShoshana Bulka PragmaticaJessica JonesNo ratings yet
- WCDMA Radio Access OverviewDocument8 pagesWCDMA Radio Access OverviewDocMasterNo ratings yet
- Speaking RubricDocument1 pageSpeaking RubricxespejoNo ratings yet
- When SIBO & IBS-Constipation Are Just Unrecognized Thiamine DeficiencyDocument3 pagesWhen SIBO & IBS-Constipation Are Just Unrecognized Thiamine Deficiencyps piasNo ratings yet
- Ortho TechnologyDocument196 pagesOrtho Technologyr3doc3No ratings yet
- Assessment - UK Forestry Data ICT THEORY For CAT1Document13 pagesAssessment - UK Forestry Data ICT THEORY For CAT1Joanna AchemaNo ratings yet
- Icc Esr-2302 Kb3 ConcreteDocument11 pagesIcc Esr-2302 Kb3 ConcretexpertsteelNo ratings yet
- Academic Performance of Senior High School Students 4Ps Beneficiaries in VNHSDocument19 pagesAcademic Performance of Senior High School Students 4Ps Beneficiaries in VNHSkathlen mae marollanoNo ratings yet
- Bullying Report - Ending The Torment: Tackling Bullying From The Schoolyard To CyberspaceDocument174 pagesBullying Report - Ending The Torment: Tackling Bullying From The Schoolyard To CyberspaceAlexandre AndréNo ratings yet
- 8 Adam AmuraroDocument28 pages8 Adam Amurarokmeena73No ratings yet
- An Introduction To Routine and Special StainingDocument13 pagesAn Introduction To Routine and Special StainingBadiu ElenaNo ratings yet
- Sips 1328Document64 pagesSips 1328Jean Claude De AldánNo ratings yet
- Midterm ReviewerDocument20 pagesMidterm ReviewerJonnafe IgnacioNo ratings yet
- NamalDocument5 pagesNamalAyusnab KarkiNo ratings yet
- CESCOM 10 - Aircraft Status Report: Maintenance InspectionsDocument78 pagesCESCOM 10 - Aircraft Status Report: Maintenance InspectionsAlejandro BarradasNo ratings yet
- KM170, KM171, KM172, F3A21, F3A22: 3 SPEED FWD (Lock Up & Non Lock Up)Document4 pagesKM170, KM171, KM172, F3A21, F3A22: 3 SPEED FWD (Lock Up & Non Lock Up)krzysiek1975No ratings yet
- A Detailed Lesson PlanDocument5 pagesA Detailed Lesson PlanIsaac-elmar Agtarap74% (23)
- Chromatographic Separation PDFDocument7 pagesChromatographic Separation PDFNicolle CletoNo ratings yet
- Science9 Q4 Week2Document16 pagesScience9 Q4 Week2Maria Josie Lopez TumlosNo ratings yet
- Some Studies On Structure and Properties of Wrapped Jute (Parafil) YarnsDocument5 pagesSome Studies On Structure and Properties of Wrapped Jute (Parafil) YarnsVedant MahajanNo ratings yet
- The Handmaid's TaleDocument40 pagesThe Handmaid's Taleleher shahNo ratings yet
- School Activity Calendar - Millsberry SchoolDocument2 pagesSchool Activity Calendar - Millsberry SchoolSushil DahalNo ratings yet
- Charles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)Document441 pagesCharles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)joan82% (17)
- A Structural Modelo of Limital Experienci Un TourismDocument15 pagesA Structural Modelo of Limital Experienci Un TourismcecorredorNo ratings yet
- The Determinants of Corporate Dividend PolicyDocument16 pagesThe Determinants of Corporate Dividend PolicyRutvikNo ratings yet
- Cella Di Carico Sartorius MP77 eDocument3 pagesCella Di Carico Sartorius MP77 eNCNo ratings yet
- High Speed Power TransferDocument33 pagesHigh Speed Power TransferJAYKUMAR SINGHNo ratings yet
- TESP12201R0Document20 pagesTESP12201R0Muhammad AliNo ratings yet
- The Sandbox Approach and Its Potential For Use inDocument13 pagesThe Sandbox Approach and Its Potential For Use invalentina sekarNo ratings yet