You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Oo-Bmomeom: Certificate of Liability InsuranceDocument1 pageOo-Bmomeom: Certificate of Liability InsuranceMon DoceNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Theoretical Framework DesignDocument3 pagesTheoretical Framework DesignMon DoceNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Case 1 ManagementDocument1 pageCase 1 ManagementMon DoceNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
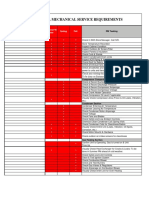
- Aspen Dental Mechanical Service Requirements: NotesDocument2 pagesAspen Dental Mechanical Service Requirements: NotesMon DoceNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 5 6109582981330895076Document5 pages5 6109582981330895076Mon DoceNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Objective TreeDocument1 pageObjective TreeMon DoceNo ratings yet
- Volvulus: Carol K. Le Phillip Nahirniak Sachit Anand Wantzy Cooper. Author InformationDocument22 pagesVolvulus: Carol K. Le Phillip Nahirniak Sachit Anand Wantzy Cooper. Author InformationMon DoceNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Clinical Summary (Dr. Yaoyao Meds)Document2 pagesClinical Summary (Dr. Yaoyao Meds)Mon DoceNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Type of FeedingDocument1 pageType of FeedingMon DoceNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Davao Medical School Foundation Inc. College of MidwiferyDocument2 pagesDavao Medical School Foundation Inc. College of MidwiferyMon DoceNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Quiz 1Document41 pagesQuiz 1Mon DoceNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- (Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Document1 page(Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Mon DoceNo ratings yet
- Sundown Quizzes PNLE 2018Document42 pagesSundown Quizzes PNLE 2018Mon DoceNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Your Patient Today Will Be Sheny DredDocument6 pagesYour Patient Today Will Be Sheny DredMon DoceNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Quiz EndocrineDocument16 pagesQuiz EndocrineMon DoceNo ratings yet
- Your Patient Today Will Be Sheny DredDocument6 pagesYour Patient Today Will Be Sheny DredMon DoceNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Sundown Quizzes PNLE 2018Document42 pagesSundown Quizzes PNLE 2018Mon DoceNo ratings yet
- (Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Document1 page(Minimal Haziness Seen On The Right Lobe?) (Or Blunted?)Mon DoceNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- CaseDocument1 pageCaseMon DoceNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Quiz EndocrineDocument16 pagesQuiz EndocrineMon DoceNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Quiz 1Document41 pagesQuiz 1Mon DoceNo ratings yet
- Clinical Summary (Dr. Yaoyao Meds)Document2 pagesClinical Summary (Dr. Yaoyao Meds)Mon DoceNo ratings yet
- Notes On Common Pediatric Drugs, Dosaging and Package: For FeverDocument1 pageNotes On Common Pediatric Drugs, Dosaging and Package: For FeverMon DoceNo ratings yet
- CaseDocument1 pageCaseMon DoceNo ratings yet
- SDASSDSADSADDocument2 pagesSDASSDSADSADMon DoceNo ratings yet
- Davao Medical School Foundation Department of Obstetrics and Gynecology APRIL 24, 2020 TOPIC: 25 Year-Old With AMENORRHEA (Student's Copy)Document11 pagesDavao Medical School Foundation Department of Obstetrics and Gynecology APRIL 24, 2020 TOPIC: 25 Year-Old With AMENORRHEA (Student's Copy)Mon DoceNo ratings yet
- VRDocument2 pagesVRMon DoceNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Neonatal ResuscitationDocument4 pagesNeonatal ResuscitationMon DoceNo ratings yet
- Mon Doce Online Exam 1Document43 pagesMon Doce Online Exam 1Mon DoceNo ratings yet
- Citibank Vs Hon ChuaDocument12 pagesCitibank Vs Hon ChuaJA BedrioNo ratings yet
- Bekic (Ed) - Submerged Heritage 6 Web Final PDFDocument76 pagesBekic (Ed) - Submerged Heritage 6 Web Final PDFutvrdaNo ratings yet
- Chapters Name in Sanskrit and English Setting The SceneDocument3 pagesChapters Name in Sanskrit and English Setting The Sceneishvarchandra dasNo ratings yet
- Block-1 Communication IGNOUDocument81 pagesBlock-1 Communication IGNOUr kumarNo ratings yet
- Manuel Vs AlfecheDocument2 pagesManuel Vs AlfecheGrace0% (1)
- Faculty of Computer Science and Information TechnologyDocument4 pagesFaculty of Computer Science and Information TechnologyNurafiqah Sherly Binti ZainiNo ratings yet
- Solaris Hardening Guide v1Document56 pagesSolaris Hardening Guide v1GusGualdNo ratings yet
- Chapter 2 Demand (ECO415)Document28 pagesChapter 2 Demand (ECO415)hurin inaniNo ratings yet
- All-India rWnMYexDocument89 pagesAll-India rWnMYexketan kanameNo ratings yet
- AN6001-G16 Optical Line Terminal Equipment Product Overview Version ADocument74 pagesAN6001-G16 Optical Line Terminal Equipment Product Overview Version AAdriano CostaNo ratings yet
- 1219201571137027Document5 pages1219201571137027Nishant SinghNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2.1BSA-CY2 - REVERAL, ANGELA R. - EXERCISE#1 - Management ScienceDocument3 pages2.1BSA-CY2 - REVERAL, ANGELA R. - EXERCISE#1 - Management ScienceAngela Ricaplaza ReveralNo ratings yet
- UNIT 1 Previewing and PredictingDocument8 pagesUNIT 1 Previewing and PredictingRisa nurlailiNo ratings yet
- Chapter 8 Supplier Quality ManagementDocument71 pagesChapter 8 Supplier Quality ManagementAnh NguyenNo ratings yet
- SAi Sankata Nivarana StotraDocument3 pagesSAi Sankata Nivarana Stotrageetai897No ratings yet
- Arthropods: Surviving The Frost: Charmayne Roanna L. GalangDocument2 pagesArthropods: Surviving The Frost: Charmayne Roanna L. GalangBabes-Rose GalangNo ratings yet
- Assignment 1: Microeconomics - Group 10Document13 pagesAssignment 1: Microeconomics - Group 10Hải LêNo ratings yet
- THM07 Module 2 The Tourist Market and SegmentationDocument14 pagesTHM07 Module 2 The Tourist Market and Segmentationjennifer mirandaNo ratings yet
- Federal Ombudsman of Pakistan Complaints Resolution Mechanism For Overseas PakistanisDocument41 pagesFederal Ombudsman of Pakistan Complaints Resolution Mechanism For Overseas PakistanisWaseem KhanNo ratings yet
- Test For Determining Agency - Analysis Using Case LawsDocument7 pagesTest For Determining Agency - Analysis Using Case Lawsanitta joseNo ratings yet
- Financial Accounting Theory Craig Deegan Chapter 7Document9 pagesFinancial Accounting Theory Craig Deegan Chapter 7Sylvia Al-a'maNo ratings yet
- Network Monitoring & Forensics: Jim IrvingDocument102 pagesNetwork Monitoring & Forensics: Jim IrvingKarel GoldmannNo ratings yet
- Principles of Cooking MethodsDocument8 pagesPrinciples of Cooking MethodsAizelle Guerrero Santiago100% (1)
- Co-Publisher AgreementDocument1 pageCo-Publisher AgreementMarcinNo ratings yet
- TRYOUT1Document8 pagesTRYOUT1Zaenul WafaNo ratings yet
- Bacanie 2400 Articole Cu Cod de BareDocument12 pagesBacanie 2400 Articole Cu Cod de BareGina ManolacheNo ratings yet
- Indian School Bousher Final Term End Exam (T2) : Academic Session - 2021-22 Grade: 7Document7 pagesIndian School Bousher Final Term End Exam (T2) : Academic Session - 2021-22 Grade: 7Shresthik VenkateshNo ratings yet
- Social Studies 5th Grade Georgia StandardsDocument6 pagesSocial Studies 5th Grade Georgia Standardsapi-366462849No ratings yet
- Jamb Crk-Past QuestionDocument59 pagesJamb Crk-Past QuestionFadele1981No ratings yet
- Wa0006.Document8 pagesWa0006.Poonm ChoudharyNo ratings yet