You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sickle Cell AnemiaDocument63 pagesSickle Cell Anemiaoss-20502745100% (4)
- Whe The Sun Bur The Eni of SCHDocument241 pagesWhe The Sun Bur The Eni of SCHArhip CojocNo ratings yet
- NeurotransmittersDocument92 pagesNeurotransmittersClare DucutNo ratings yet
- Krok 2014 Base All 2Document237 pagesKrok 2014 Base All 2Gaurav S Batra0% (1)
- Fluid and Electrolyte Imbalance QuizDocument2 pagesFluid and Electrolyte Imbalance QuizteabagmanNo ratings yet
- ErythromycinDocument2 pagesErythromycinEurielle MioleNo ratings yet
- Neuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawangDocument65 pagesNeuro-Ophthalmology: DR Jusuf Wijaya, SPM FK - Uki CawanggeorgyNo ratings yet
- International Society For Peritoneal Dialysis Practice Recommendations: Prescribing High-Quality Goal-Directed Peritoneal DialysisDocument10 pagesInternational Society For Peritoneal Dialysis Practice Recommendations: Prescribing High-Quality Goal-Directed Peritoneal DialysisMade Dedy KusnawanNo ratings yet
- 8-Article Text-8-1-10-20181018Document7 pages8-Article Text-8-1-10-20181018Made Dedy KusnawanNo ratings yet
- How To Manage Steroid Diabetes in The Patient With CancerDocument5 pagesHow To Manage Steroid Diabetes in The Patient With CancerMade Dedy KusnawanNo ratings yet
- Khowaja2018 Article GlycemicControlInHospitalizedP PDFDocument9 pagesKhowaja2018 Article GlycemicControlInHospitalizedP PDFMade Dedy KusnawanNo ratings yet
- Steroid Hyperglycemia: Prevalence, Early Detection and Therapeutic Recommendations: A Narrative ReviewDocument10 pagesSteroid Hyperglycemia: Prevalence, Early Detection and Therapeutic Recommendations: A Narrative ReviewMade Dedy KusnawanNo ratings yet
- Common Dose AnakDocument2 pagesCommon Dose AnakMade Dedy KusnawanNo ratings yet
- EpistasisDocument26 pagesEpistasisy4heherNo ratings yet
- Evaluation of Anti Stress Effects of Nardostachys Jatamansi DC Root Extract On Clinical Patients A Psycological EstimationDocument8 pagesEvaluation of Anti Stress Effects of Nardostachys Jatamansi DC Root Extract On Clinical Patients A Psycological EstimationESSENCE - International Journal for Environmental Rehabilitation and ConservaionNo ratings yet
- EsophagomyotomyDocument3 pagesEsophagomyotomySamVelascoNo ratings yet
- World Bank Essay From The PhilippinesDocument8 pagesWorld Bank Essay From The PhilippinesDavid Michael San JuanNo ratings yet
- Concept Map PedsDocument6 pagesConcept Map Pedsapi-546398486No ratings yet
- 7 Mistakes Divers Make: and How To Avoid ThemDocument12 pages7 Mistakes Divers Make: and How To Avoid ThemFranciscoNo ratings yet
- Timing of Revascularization in Patients With Transient ST Segment Elevation Myocardial Infarction A Randomized Clinical TrialDocument9 pagesTiming of Revascularization in Patients With Transient ST Segment Elevation Myocardial Infarction A Randomized Clinical TrialWelly WijayaNo ratings yet
- MCQ Final 1981Document19 pagesMCQ Final 1981JohnSonNo ratings yet
- Case Study: MaricultureDocument51 pagesCase Study: MaricultureAmelia C. BiberaNo ratings yet
- Prentice9e Im Chap19Document6 pagesPrentice9e Im Chap19api-2813400240% (1)
- Calcutta Samaritans ReportDocument15 pagesCalcutta Samaritans ReportAshok GeorgeNo ratings yet
- AmitriptylineDocument13 pagesAmitriptylineاحمد محسنNo ratings yet
- 8, Identitas Pasien SoapDocument10 pages8, Identitas Pasien SoapsunarsihNo ratings yet
- 3.lessons 21-22, Respiratory System, PP 446-456Document28 pages3.lessons 21-22, Respiratory System, PP 446-456Lazare ChNo ratings yet
- FijiTimes Aug 12 2016 PDFDocument20 pagesFijiTimes Aug 12 2016 PDFfijitimescanadaNo ratings yet
- District Health Profile PeshawarDocument14 pagesDistrict Health Profile Peshawarkhalilishtiaq6361No ratings yet
- Full Essentials of Pediatric Nursing 3Rd Edition Kyle Carman Test Bank PDF Docx Full Chapter ChapterDocument36 pagesFull Essentials of Pediatric Nursing 3Rd Edition Kyle Carman Test Bank PDF Docx Full Chapter Chapterophismprecludekil0100% (23)
- Marieb Ch3aDocument45 pagesMarieb Ch3aNorhayna DadiaNo ratings yet
- II EXAMEN DEPARTAMENTALSR LDocument8 pagesII EXAMEN DEPARTAMENTALSR LPaloma JGNo ratings yet
- Annex A - MT LAWSDocument6 pagesAnnex A - MT LAWSFrances Riane SimoyNo ratings yet
- AJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Document13 pagesAJOG Modelo Predictivo para Preeclampsia Nicolaides 2019Ana PadillaNo ratings yet
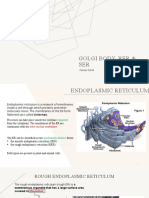
- Golgi Body, Rer & SerDocument8 pagesGolgi Body, Rer & SerZainab ZahidNo ratings yet
- Asymmetrical Hearing Loss and Mega Cisterna Magna: A Case StudyDocument5 pagesAsymmetrical Hearing Loss and Mega Cisterna Magna: A Case StudyValentina Jara CalderónNo ratings yet