You might also like
- Studies, Trials and Scientific Evidence Hierarchy - Lecture 1 - BTDocument48 pagesStudies, Trials and Scientific Evidence Hierarchy - Lecture 1 - BTblack.hadi194No ratings yet
- Introduction To Clinical Trials - 07april - 2021Document46 pagesIntroduction To Clinical Trials - 07april - 2021jeffreyNo ratings yet
- CDP - Design Decisions & Trial Design - 4-Jul-10Document67 pagesCDP - Design Decisions & Trial Design - 4-Jul-10Dnyanesh LimayeNo ratings yet
- Topic 10Document7 pagesTopic 10Arokiasamy JairishNo ratings yet
- Causality Assessment of Adverse Drug Reactions (ADR)Document21 pagesCausality Assessment of Adverse Drug Reactions (ADR)suhas reddy0% (1)
- Evidence-Based Medicine - UpToDateDocument20 pagesEvidence-Based Medicine - UpToDateKaiser D.No ratings yet
- Practice of Pharmacy: Prepared By: Jelly Mae T. Oviedo, RPHDocument37 pagesPractice of Pharmacy: Prepared By: Jelly Mae T. Oviedo, RPHNica ChuaNo ratings yet
- Pharmacoeconomics 3rd Prof.Document64 pagesPharmacoeconomics 3rd Prof.Ahmed ImranNo ratings yet
- Chapter 12 Systematic Review of Prognostic TestsDocument13 pagesChapter 12 Systematic Review of Prognostic TestsMuammar EmirNo ratings yet
- Randomized Controlled TrialDocument34 pagesRandomized Controlled TrialnouiraNo ratings yet
- Translet Farmakoterapi LanjutanDocument3 pagesTranslet Farmakoterapi LanjutanAlexander KwaitotaNo ratings yet
- Desain Uji KlinikDocument49 pagesDesain Uji KlinikAndika AfriansyahNo ratings yet
- Real-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsDocument5 pagesReal-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsCognizantNo ratings yet
- Patient Satisfaction: Presented by Amaal MersalDocument48 pagesPatient Satisfaction: Presented by Amaal MersalEhab Ahmed Hussein ReyadNo ratings yet
- glossaryoftermsusedinclinicaltrialsDocument8 pagesglossaryoftermsusedinclinicaltrialsingles.kesherNo ratings yet
- ACTG QOL 601-602 (QOL 601-2) Health Survey ManualDocument31 pagesACTG QOL 601-602 (QOL 601-2) Health Survey Manualjason manalotoNo ratings yet
- Clinical Trails GlossaryDocument68 pagesClinical Trails Glossaryapi-3810976100% (1)
- Epidemiology Lec 9Document24 pagesEpidemiology Lec 9اسامة محمد السيد رمضانNo ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- Clinical trial phases drug developmentDocument38 pagesClinical trial phases drug developmentSujan AdhikariNo ratings yet
- Towards Better Patient Care Drugs To Avoid in 2018Document9 pagesTowards Better Patient Care Drugs To Avoid in 2018Mabvan SarraNo ratings yet
- Decision Making in Medicine: Clinical Decision Using An Article About Harmful EffectDocument13 pagesDecision Making in Medicine: Clinical Decision Using An Article About Harmful EffectTP RMadNo ratings yet
- AssignmentDocument8 pagesAssignmentNayab SaeedNo ratings yet
- Dr Yaser Adi's Evidence-Based Healthcare PresentationDocument130 pagesDr Yaser Adi's Evidence-Based Healthcare PresentationAnonymous hF5zAdvwCCNo ratings yet
- Screening and Diagnostic TestsDocument7 pagesScreening and Diagnostic TestsYudith AnindyaNo ratings yet
- Critical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDDocument37 pagesCritical Appraisal: Prof. Dr. Mohammad Hakimi, Spog (K), PHDFebbty KuswantiNo ratings yet
- Outcome Measure Unit 3Document20 pagesOutcome Measure Unit 3Salini PatelNo ratings yet
- EBP Appraising DiagnosticDocument95 pagesEBP Appraising DiagnostictrimayunikaNo ratings yet
- CR IntroDocument21 pagesCR Introsivaram_12213443No ratings yet
- Pharmaco VigilanceDocument31 pagesPharmaco VigilanceRasika NatuNo ratings yet
- Introduction To Evidence Based Medicine: Dr. Rahma Yuantari, MSC, SP - PK Departemen Patologi Klinik FK UiiDocument57 pagesIntroduction To Evidence Based Medicine: Dr. Rahma Yuantari, MSC, SP - PK Departemen Patologi Klinik FK UiiTaufiq HidayatNo ratings yet
- Desain Study Halaman 31 40Document5 pagesDesain Study Halaman 31 40capita doankNo ratings yet
- HRQo LDocument24 pagesHRQo LAdam QawasmiNo ratings yet
- Pharmacovigilance: "Drug Safety"Document39 pagesPharmacovigilance: "Drug Safety"Rona SalandoNo ratings yet
- Grading Evidence in Medicine: Bill Cayley JR MD Mdiv Uw Health Augusta Family MedicineDocument26 pagesGrading Evidence in Medicine: Bill Cayley JR MD Mdiv Uw Health Augusta Family MedicinerajeevsonaliNo ratings yet
- EBM-Internal Med Students-FinalDocument29 pagesEBM-Internal Med Students-FinalSelma MutiaraNo ratings yet
- BIOSTAT MIDTERM: EVALUATING CLINICAL TRIALSDocument14 pagesBIOSTAT MIDTERM: EVALUATING CLINICAL TRIALSRoh BilalNo ratings yet
- Notes - Up Till September 9, 2021Document40 pagesNotes - Up Till September 9, 2021vedant wakankarNo ratings yet
- Critiquing The Media CriteriaDocument7 pagesCritiquing The Media Criteriacoco the dodoNo ratings yet
- Lorne Basskin - Practical PE ArticleDocument5 pagesLorne Basskin - Practical PE ArticleCatalina Dumitru0% (1)
- Pharmacoepidemiology 9Document29 pagesPharmacoepidemiology 9Ani RahayuNo ratings yet
- Tutorial 9 Screening in Public Health DETA AMELIA HASRIDocument9 pagesTutorial 9 Screening in Public Health DETA AMELIA HASRIDeta HasriNo ratings yet
- Seligman Consumer Reports StudyDocument16 pagesSeligman Consumer Reports StudyZara KhanNo ratings yet
- Purpose of Drug DiscoveryDocument6 pagesPurpose of Drug DiscoveryUmer KhanNo ratings yet
- Reading Abstract FSDocument2 pagesReading Abstract FSRina WatiNo ratings yet
- Drug Development and EvaluationDocument25 pagesDrug Development and EvaluationArlises SinagaNo ratings yet
- Chapter 3Document28 pagesChapter 3SISNo ratings yet
- Critical appraisal of journal articles: A guide to evaluating research evidenceDocument29 pagesCritical appraisal of journal articles: A guide to evaluating research evidencemonique marwick100% (2)
- Experimental (Or Interventional) Studies: ConfoundingDocument4 pagesExperimental (Or Interventional) Studies: ConfoundingRiza AlfianNo ratings yet
- Identifying and Measuring Outcomes 6MN3hDocument16 pagesIdentifying and Measuring Outcomes 6MN3hYazeed AsrawiNo ratings yet
- Periodic Health ExaminationDocument38 pagesPeriodic Health ExaminationHilma NadhifaNo ratings yet
- MC N Med Dev Trials Compare With Drug TrialsDocument4 pagesMC N Med Dev Trials Compare With Drug TrialsAndrie JavsNo ratings yet
- Clinical Trials and BiostatisticsDocument16 pagesClinical Trials and BiostatisticsArumugam RamasamyNo ratings yet
- Experimental Epidemiology[1] 1Document27 pagesExperimental Epidemiology[1] 1ljilffbNo ratings yet
- 2 General Principles of Research Design and AnalysisDocument6 pages2 General Principles of Research Design and AnalysisMohamed Elprince AdelNo ratings yet
- Outcome Measures LectureDocument5 pagesOutcome Measures Lectureزيد مسعودNo ratings yet
- RCT GuideDocument29 pagesRCT Guidemvs hardhikNo ratings yet
- Introduction To Screening & Differntial DiagnosisDocument42 pagesIntroduction To Screening & Differntial DiagnosisHUSNAIN TECH AND FUNNo ratings yet
- Edit - The Monster Guide To Candlestick PatternsDocument34 pagesEdit - The Monster Guide To Candlestick PatternsArif Wira Adyatama100% (4)
- Pharmacotherapy Options for Treatment-Resistant SchizophreniaDocument6 pagesPharmacotherapy Options for Treatment-Resistant SchizophreniaSAURABH SINGHNo ratings yet
- Oxidative Stress in Sickle Cell Disease - A Tertiary Hospital Experience in Western OdishaDocument5 pagesOxidative Stress in Sickle Cell Disease - A Tertiary Hospital Experience in Western OdishaSAURABH SINGHNo ratings yet
- Gesc101 PDFDocument10 pagesGesc101 PDFlakhuindiaNo ratings yet
- Summary Antimicrobial Prescribing GuidanceDocument27 pagesSummary Antimicrobial Prescribing GuidanceZacky FairuzNo ratings yet
- Evaluating Medication Errors at a Teaching HospitalDocument60 pagesEvaluating Medication Errors at a Teaching HospitalSAURABH SINGHNo ratings yet
- Presentation On Acute Amyloid Lateral SclerosisDocument31 pagesPresentation On Acute Amyloid Lateral SclerosisSAURABH SINGHNo ratings yet
- AHT LancetDocument11 pagesAHT LancetDr Shuchita MundleNo ratings yet
- Dialysis DrugsDocument51 pagesDialysis Drugslimkokhui100% (2)
- Edit - The Monster Guide To Candlestick PatternsDocument34 pagesEdit - The Monster Guide To Candlestick PatternsArif Wira Adyatama100% (4)
- English Informed Consent Form PDFDocument1 pageEnglish Informed Consent Form PDFSAURABH SINGHNo ratings yet
- Year 10 Maths PlaneDocument62 pagesYear 10 Maths Planehal wangNo ratings yet
- Communications201101 DLDocument132 pagesCommunications201101 DLAle SandovalNo ratings yet
- 1 PBDocument11 pages1 PBAnggita Wulan RezkyanaNo ratings yet
- ElectricalDocument30 pagesElectricalketerNo ratings yet
- Ek Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics GemDocument1 pageEk Pardesi Mera Dil Le Gaya Lyrics English Translation - Lyrics Gemmahsa.molaiepanahNo ratings yet
- Membandingkan Recall 24 Jam Nutri Survey Dengan TkpiDocument7 pagesMembandingkan Recall 24 Jam Nutri Survey Dengan TkpiFransisca SihotangNo ratings yet
- Operating Manual: Please Read These Operating Instructions Before Using Your FreedomchairDocument24 pagesOperating Manual: Please Read These Operating Instructions Before Using Your FreedomchairNETHYA SHARMANo ratings yet
- JTP Brochure - 2Document6 pagesJTP Brochure - 2YAKOVNo ratings yet
- City MSJDocument50 pagesCity MSJHilary LedwellNo ratings yet
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- SMEs, Trade Finance and New TechnologyDocument34 pagesSMEs, Trade Finance and New TechnologyADBI EventsNo ratings yet
- Lesson Plan 2 Revised - Morgan LegrandDocument19 pagesLesson Plan 2 Revised - Morgan Legrandapi-540805523No ratings yet
- Lateral capacity of pile in clayDocument10 pagesLateral capacity of pile in clayGeetha MaNo ratings yet
- Final Annotated BibiliographyDocument4 pagesFinal Annotated Bibiliographyapi-491166748No ratings yet
- Best Way To LearnDocument3 pagesBest Way To LearnRAMIZKHAN124No ratings yet
- TNG UPDATE InstructionsDocument10 pagesTNG UPDATE InstructionsDiogo Alexandre Crivelari CrivelNo ratings yet
- English Extra Conversation Club International Women's DayDocument2 pagesEnglish Extra Conversation Club International Women's Dayevagloria11No ratings yet
- Bhakti Trader Ram Pal JiDocument232 pagesBhakti Trader Ram Pal JiplancosterNo ratings yet
- Body Shaming Among School Going AdolesceDocument5 pagesBody Shaming Among School Going AdolesceClara Widya Mulya MNo ratings yet
- Structural IfpDocument4 pagesStructural IfpDanny NguyenNo ratings yet
- School of Public Health: Haramaya University, ChmsDocument40 pagesSchool of Public Health: Haramaya University, ChmsRida Awwal100% (1)
- SS1c MIDTERMS LearningModuleDocument82 pagesSS1c MIDTERMS LearningModuleBryce VentenillaNo ratings yet
- GVB 1Document8 pagesGVB 1Aaron SylvestreNo ratings yet
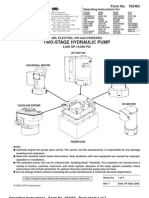
- Power Team PE55 ManualDocument13 pagesPower Team PE55 ManualTitanplyNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
- Geometric Sculpture From 72 PencilsDocument5 pagesGeometric Sculpture From 72 PencilsHugo Iván Gonzalez CruzNo ratings yet
- Abbreviation Meaning Notes: Cibo ("With Food")Document4 pagesAbbreviation Meaning Notes: Cibo ("With Food")TantriNo ratings yet
- TILE FIXING GUIDEDocument1 pageTILE FIXING GUIDEStavros ApostolidisNo ratings yet
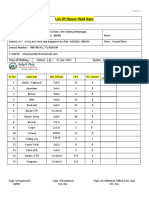
- List of household items for relocationDocument4 pagesList of household items for relocationMADDYNo ratings yet
- European Business in China Position Paper 2017 2018 (English Version)Document408 pagesEuropean Business in China Position Paper 2017 2018 (English Version)Prasanth RajuNo ratings yet






















































![Experimental Epidemiology[1] 1](https://imgv2-2-f.scribdassets.com/img/document/719742795/149x198/c335b883fc/1712168237?v=1)