You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Low Carb RevolutionDocument457 pagesThe Low Carb RevolutionJohn McLean100% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Jan 2021 QuestionnaireDocument6 pagesJan 2021 Questionnairealiz k100% (2)
- Heart Disease Case StudyDocument13 pagesHeart Disease Case Studyapi-284823421100% (1)
- FMcase 2Document27 pagesFMcase 2Ryan Townsend100% (3)
- Mark Hyman - The Blood Sugar Solution 10-Day Detox DietDocument561 pagesMark Hyman - The Blood Sugar Solution 10-Day Detox DietPrasad PillarisettiNo ratings yet
- CHN ReviewerDocument9 pagesCHN ReviewerShare MeNo ratings yet
- Public Health Ethics Key - Concepts and Issues in Policy and PracticeDocument247 pagesPublic Health Ethics Key - Concepts and Issues in Policy and Practicemnigam64No ratings yet
- Soduim Prescription in The Prevention of Intradialytic HypotensionDocument10 pagesSoduim Prescription in The Prevention of Intradialytic HypotensionTalala tililiNo ratings yet
- Bardet-Biedl Syndrome Is It Only Cilia DysfunctionDocument13 pagesBardet-Biedl Syndrome Is It Only Cilia DysfunctionTalala tililiNo ratings yet
- Le Syndrome de Bardet Biedl Endocrino 2008Document9 pagesLe Syndrome de Bardet Biedl Endocrino 2008Talala tililiNo ratings yet
- Association of Bifid Epiglottis and Laryngeal Web With Bardet BiedlDocument3 pagesAssociation of Bifid Epiglottis and Laryngeal Web With Bardet BiedlTalala tililiNo ratings yet
- MODULE 3 Lesson 1-3Document14 pagesMODULE 3 Lesson 1-3Elenor May Chantal MessakaraengNo ratings yet
- Impact of Food On HealthDocument3 pagesImpact of Food On HealthAmit GolaNo ratings yet
- Tanvir Osteoporosis Centre: Tissue Mapping Segmental AnalysisDocument5 pagesTanvir Osteoporosis Centre: Tissue Mapping Segmental AnalysiskchowNo ratings yet
- Association Between Obesity and Thyroid Hormone Levels Among Saudi Arabian PatientsDocument4 pagesAssociation Between Obesity and Thyroid Hormone Levels Among Saudi Arabian PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetes NIDocument8 pagesDiabetes NIBeatrizCamposNo ratings yet
- Science - Death of The Calorie - 1843 Magazine - The EconomistDocument21 pagesScience - Death of The Calorie - 1843 Magazine - The EconomistLy LuongNo ratings yet
- GR 168081 Yrasuegui Vs PALDocument17 pagesGR 168081 Yrasuegui Vs PALJP De La PeñaNo ratings yet
- Department of Education: Republic of The PhilippinesDocument7 pagesDepartment of Education: Republic of The Philippinesmazie lopezNo ratings yet
- SF8 2019 SampleDocument6 pagesSF8 2019 Samplemacren septemberNo ratings yet
- Eapp Quarter 2 Module 8Document6 pagesEapp Quarter 2 Module 8Jasmine CorpuzNo ratings yet
- Malnutrition Screening Tool (MST)Document3 pagesMalnutrition Screening Tool (MST)Aini SavinaNo ratings yet
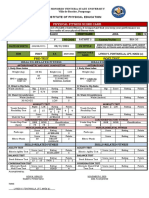
- Pre-Test Post Test: Physical Fitness Score CardDocument2 pagesPre-Test Post Test: Physical Fitness Score CardRed CactusNo ratings yet
- Relationship Between Parental Control and Child's Eating BehaviorsDocument10 pagesRelationship Between Parental Control and Child's Eating Behaviorsapi-556856793No ratings yet
- Formulas de PesoDocument4 pagesFormulas de PesoviaereaNo ratings yet
- Bulking Up WorkoutDocument7 pagesBulking Up WorkoutP_leeNo ratings yet
- The Effects of A Healthy LifestyleDocument5 pagesThe Effects of A Healthy LifestyleMary Monique OrdinarioNo ratings yet
- Peh 1 (Notes)Document14 pagesPeh 1 (Notes)Louise Bea ValbuenaNo ratings yet
- Articles About Gossip ShowsDocument5 pagesArticles About Gossip ShowssuperultimateamazingNo ratings yet
- Renal Cell CancerDocument575 pagesRenal Cell CancerIon VasianNo ratings yet
- Jurnal Studi Ekologi Bahasa Inggris PDFDocument6 pagesJurnal Studi Ekologi Bahasa Inggris PDFpinashty aulianaNo ratings yet
- 110 Course Reader Spring 2015Document87 pages110 Course Reader Spring 2015CindiHarris100% (1)
- Nutrition Applied in Nursing "Supersize Me": DE CHAVEZ, Michaela P. Prof. Geralden G. Cantor Prof. Ann Maris L. RellamaDocument2 pagesNutrition Applied in Nursing "Supersize Me": DE CHAVEZ, Michaela P. Prof. Geralden G. Cantor Prof. Ann Maris L. Rellamaela garciaNo ratings yet
- Slim and SassyDocument13 pagesSlim and Sassyhmaddy3117No ratings yet