You might also like
- Toward a Healthier Garden State: Beyond Cancer Clusters and COVIDFrom EverandToward a Healthier Garden State: Beyond Cancer Clusters and COVIDNo ratings yet
- Social determinants of health: Understanding the causes of health inequalitiesDocument3 pagesSocial determinants of health: Understanding the causes of health inequalitiesAcelasi' AndreiNo ratings yet
- Community Health Factors and Health DisparitiesDocument7 pagesCommunity Health Factors and Health Disparitiesshreeguru8No ratings yet
- Frieden - Health Impact Pyramid PDFDocument6 pagesFrieden - Health Impact Pyramid PDFFernanda PachecoNo ratings yet
- The Social Determinants of Health: It's Time To Consider The Causes of The CausesDocument13 pagesThe Social Determinants of Health: It's Time To Consider The Causes of The CausesMayson BaliNo ratings yet
- Contributions of Public Health, Pharmaceuticals and Other Medical Care To US Life Expectancy Changes, 1990-2015Document11 pagesContributions of Public Health, Pharmaceuticals and Other Medical Care To US Life Expectancy Changes, 1990-2015Mouna DardouriNo ratings yet
- Social Epidemiology: Questionable Answers and Answerable QuestionsDocument4 pagesSocial Epidemiology: Questionable Answers and Answerable QuestionsAsad MotenNo ratings yet
- Public Health and Level of PrevetionDocument17 pagesPublic Health and Level of PrevetionMalik AwanNo ratings yet
- Marmot Wilkonson - The Solid FactsDocument31 pagesMarmot Wilkonson - The Solid FactsLavinia BaleaNo ratings yet
- Discussion Paper Creating Social and Health Equity:: Adopting An Alberta Social Determinants of Health FrameworkDocument25 pagesDiscussion Paper Creating Social and Health Equity:: Adopting An Alberta Social Determinants of Health FrameworksukandeNo ratings yet
- Social Epidemiology: Questionable Answers and Answerable QuestionsDocument4 pagesSocial Epidemiology: Questionable Answers and Answerable QuestionsvictorNo ratings yet
- Module 3 Determinants of HealthDocument31 pagesModule 3 Determinants of HealthSamuel MbiriNo ratings yet
- Determinants of Health: DR Amir Akbar Shaikh Asst. Prof (Head of Department) Community DentistryDocument42 pagesDeterminants of Health: DR Amir Akbar Shaikh Asst. Prof (Head of Department) Community DentistryAriba AsifNo ratings yet
- Emerging Theories Into The Social Determinants of Health: Implications For Oral Health PromotionDocument7 pagesEmerging Theories Into The Social Determinants of Health: Implications For Oral Health PromotionEmmanuel PìnheiroNo ratings yet
- The (Still) Limited Contribution of Medical Measures To Declines in MortalityDocument5 pagesThe (Still) Limited Contribution of Medical Measures To Declines in MortalityJohn SmithNo ratings yet
- Sfc01-Social Science Perspectives On Health M2021HE024 Bijal PrajapatiDocument13 pagesSfc01-Social Science Perspectives On Health M2021HE024 Bijal PrajapatiBijal PrajapatiNo ratings yet
- P3 Health StatusDocument9 pagesP3 Health StatusNovita Mariani GlekoNo ratings yet
- All Over The MapDocument76 pagesAll Over The Mapxap4228No ratings yet
- (Critical Global Health - Evidence, Efficacy, Ethnography) Vincanne Adams - Metrics - What Counts in Global Health-Duke University Press (2016)Document265 pages(Critical Global Health - Evidence, Efficacy, Ethnography) Vincanne Adams - Metrics - What Counts in Global Health-Duke University Press (2016)gastonpereztaborda100% (1)
- Mental Health Recovery and Transformation Lessons For ActionDocument5 pagesMental Health Recovery and Transformation Lessons For ActionYorinda AlNo ratings yet
- Combined ReadingsDocument137 pagesCombined Readingsfaustina lim shu enNo ratings yet
- An Ecological Perspective On Health Promotion ProgramsDocument27 pagesAn Ecological Perspective On Health Promotion ProgramsDaniel MesaNo ratings yet
- Should Texas Fund Bariatric SurgeryDocument47 pagesShould Texas Fund Bariatric SurgerynaranothNo ratings yet
- Health Indicators: Ple 2000 & Healthy People 2010) Were MoreDocument5 pagesHealth Indicators: Ple 2000 & Healthy People 2010) Were MoreSyamsir RusdinNo ratings yet
- Community Diagnosis Health IndicatorsDocument42 pagesCommunity Diagnosis Health IndicatorsHany Aboelhamd Abdelgafar100% (1)
- Global Health Is Public HealthDocument3 pagesGlobal Health Is Public HealthDr Vijay Kumar Chattu MD, MPHNo ratings yet
- Brownson - Applied Epidemiology - Theory To Practice PDFDocument413 pagesBrownson - Applied Epidemiology - Theory To Practice PDFGentic Nguyen100% (3)
- Module 1 NRSG780Document12 pagesModule 1 NRSG780justdoyourNo ratings yet
- Public Health 101Document40 pagesPublic Health 101Siddarth Palleti100% (1)
- McKeown 2016 Determinants of Health (Ch9 Brown & Closser Understanding & Applying Medical Anthropology) )Document10 pagesMcKeown 2016 Determinants of Health (Ch9 Brown & Closser Understanding & Applying Medical Anthropology) )Jesse StockerNo ratings yet
- 5 Activities That The State Government Performs For HealthcareDocument5 pages5 Activities That The State Government Performs For HealthcareWonder LostNo ratings yet
- Work, Health, and Nursing ResearchDocument2 pagesWork, Health, and Nursing ResearchVita EvelynNo ratings yet
- Health Impact AssessmentDocument14 pagesHealth Impact AssessmentVictorNo ratings yet
- Su 6103Document44 pagesSu 6103Yulisa Prahasti Dewa AyuNo ratings yet
- Nimhd Strategic Plan 2021 2025Document38 pagesNimhd Strategic Plan 2021 2025jeanbourgeatNo ratings yet
- U.S. Department of Health, Education, and Welfare, 1979 IOM, 1982Document14 pagesU.S. Department of Health, Education, and Welfare, 1979 IOM, 1982puskesmas beloNo ratings yet
- Understanding Changing Concepts of HealthDocument4 pagesUnderstanding Changing Concepts of HealthHương PhạmNo ratings yet
- Leading Health Indicators 2011Document4 pagesLeading Health Indicators 2011ulul azmiNo ratings yet
- 2020 07 Direct and Indirect Impacts of Covid19 On Health and WellbeingDocument38 pages2020 07 Direct and Indirect Impacts of Covid19 On Health and Wellbeingdavedavids0n8475No ratings yet
- The Demography of Health and Health Care: Second EditionDocument385 pagesThe Demography of Health and Health Care: Second EditionTika Nur Laili L HiperkesNo ratings yet
- Global HealthDocument3 pagesGlobal HealthDinda ElahmadiNo ratings yet
- Notes For TestDocument44 pagesNotes For TestJingosi RAMPHARWANENo ratings yet
- Confronting Health Inequity - The Global DimensionDocument5 pagesConfronting Health Inequity - The Global Dimensionmanique_abeyrat2469No ratings yet
- Factors Influencing Health Knowledge and Behaviors Among The Elderly in Rural ChinaDocument17 pagesFactors Influencing Health Knowledge and Behaviors Among The Elderly in Rural ChinaDilaArdaNiNo ratings yet
- Lin - Gender SensitiveDocument8 pagesLin - Gender SensitivemariaconstanzavasqueNo ratings yet
- Social Determinants of Health, Infant Mortality Rates and Life Expectancy Name Subject SchoolDocument6 pagesSocial Determinants of Health, Infant Mortality Rates and Life Expectancy Name Subject SchooljohnbeardNo ratings yet
- Ijerph 17155403Document16 pagesIjerph 17155403Residente EnfermeroNo ratings yet
- Disparities Interim Report 2Document33 pagesDisparities Interim Report 2Lydia WanjikuNo ratings yet
- Social Determinants of Heart Disease in the ElderlyDocument4 pagesSocial Determinants of Heart Disease in the ElderlyAna MariaNo ratings yet
- Socialdeterminantsof Health:Anoverviewforthe PrimarycareproviderDocument19 pagesSocialdeterminantsof Health:Anoverviewforthe PrimarycareproviderCarlos Hernan Castañeda RuizNo ratings yet
- GG2071 Health DevelopmentDocument38 pagesGG2071 Health DevelopmentamyhryhorukNo ratings yet
- Figure 32.1Document2 pagesFigure 32.1Alyssa AshleyNo ratings yet
- Dying Green: A Journey through End-of-Life Medicine in Search of Sustainable Health CareFrom EverandDying Green: A Journey through End-of-Life Medicine in Search of Sustainable Health CareNo ratings yet
- Reconceiving Health Care To Improve Quality: William C. RichardsonDocument22 pagesReconceiving Health Care To Improve Quality: William C. RichardsonRob streetmanNo ratings yet
- Public Health EthicsDocument17 pagesPublic Health EthicsNongre ArphonNo ratings yet
- Changing Our Understanding of HealthDocument4 pagesChanging Our Understanding of HealthNGUYÊN PHẠM NGỌC KHÔINo ratings yet
- ExplanationDocument2 pagesExplanationAeron Jay Manuel TamangNo ratings yet
- Biostatistics On HealthDocument44 pagesBiostatistics On HealthNaresh KhanderayNo ratings yet
- Order 3697070Document20 pagesOrder 3697070GithinjiPeterNo ratings yet
- Drive AI-Powered Innovation and Intelligent Action: Data Cloud SummitDocument24 pagesDrive AI-Powered Innovation and Intelligent Action: Data Cloud Summitcwag68No ratings yet
- TermpaperDocument22 pagesTermpapercwag68No ratings yet
- SampleDocument13 pagesSamplecwag68No ratings yet
- How to Play the Cypher SystemDocument434 pagesHow to Play the Cypher SystemMNo ratings yet
- Arctic Terrain Shop RulesDocument28 pagesArctic Terrain Shop Rulescwag68No ratings yet
- Choosing the Right Database on Google CloudDocument30 pagesChoosing the Right Database on Google Cloudcwag68No ratings yet
- Data and Analytics Sharing at Equifax: Immediate, Interconnected, Scalable, and SecureDocument30 pagesData and Analytics Sharing at Equifax: Immediate, Interconnected, Scalable, and Securecwag68No ratings yet
- Solving for the future with Intelligent Data and Analytics FabricDocument18 pagesSolving for the future with Intelligent Data and Analytics Fabriccwag68No ratings yet
- Google Cloud Database Strategy: Solving for the futureDocument30 pagesGoogle Cloud Database Strategy: Solving for the futurecwag68No ratings yet
- Main Exploration TableDocument2 pagesMain Exploration Tablecwag68No ratings yet
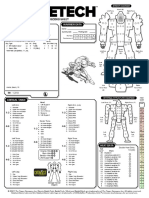
- Battlemech Record Sheet: 'Mech Data Warrior DataDocument1 pageBattlemech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- Battlemech Record Sheet: 'Mech Data Warrior DataDocument1 pageBattlemech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- Omnimech Record Sheet: 'Mech Data Warrior DataDocument1 pageOmnimech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- Omnimech Record Sheet: 'Mech Data Warrior DataDocument1 pageOmnimech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- Plot FormulasDocument2 pagesPlot FormulasIgor Airoides100% (12)
- Magical World BuilderDocument69 pagesMagical World BuilderRyan D Hall83% (6)
- Starfinder Auto Fill Sheet PDFDocument3 pagesStarfinder Auto Fill Sheet PDFnotgonna tellyouNo ratings yet
- BtechDocument2 pagesBtechcwag68No ratings yet
- Draw As Many Level 1 Treasure Cards As The Number of HeroesDocument1 pageDraw As Many Level 1 Treasure Cards As The Number of Heroescwag68No ratings yet
- Run One B&E Extraction: Meet TagsDocument3 pagesRun One B&E Extraction: Meet Tagscwag68No ratings yet
- ReadmeDocument1 pageReadmecwag68No ratings yet
- MessageDocument3 pagesMessagecwag68No ratings yet
- Sharing Desktop Via Skype SoftwareDocument1 pageSharing Desktop Via Skype Softwarecwag68No ratings yet
- Setup Sequence: Corellian CorvetteDocument2 pagesSetup Sequence: Corellian Corvettecwag68No ratings yet
- HistoryDocument1 pageHistorycwag68No ratings yet
- Omnimech Record Sheet: 'Mech Data Warrior DataDocument1 pageOmnimech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- Sequence of Play BG WWIIDocument3 pagesSequence of Play BG WWIIcwag68No ratings yet
- Omnimech Record Sheet: 'Mech Data Warrior DataDocument1 pageOmnimech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- Battlemech Record Sheet: 'Mech Data Warrior DataDocument1 pageBattlemech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- Battlemech Record Sheet: 'Mech Data Warrior DataDocument1 pageBattlemech Record Sheet: 'Mech Data Warrior Datacwag68No ratings yet
- The ShipbuilderDocument23 pagesThe Shipbuilderjunkyard0% (1)
- Amazing Health Benefits of Olive Oil BY NiyatijsDocument3 pagesAmazing Health Benefits of Olive Oil BY NiyatijsAsad ImranNo ratings yet
- (IJCST-V7I6P5) :S. A. Shaban, A. G. Sedki, D. L. ElsheweikhDocument16 pages(IJCST-V7I6P5) :S. A. Shaban, A. G. Sedki, D. L. ElsheweikhEighthSenseGroupNo ratings yet
- Natural Pet Food ReviewDocument34 pagesNatural Pet Food ReviewDafne CoilaNo ratings yet
- Health Status of Fishing Communities - by Dr. Rajan R PatilDocument45 pagesHealth Status of Fishing Communities - by Dr. Rajan R PatilDr. Rajan R Patil100% (3)
- Obesity FDocument25 pagesObesity FRashmi SinghNo ratings yet
- Effect of Cumin Powder On Body Composition and Lipid Profile in Overweight and Obese WomenDocument5 pagesEffect of Cumin Powder On Body Composition and Lipid Profile in Overweight and Obese WomenRaul DavilaNo ratings yet
- Grammar Practice with Focus on Nouns, Numbers, Adjectives and AdverbsDocument5 pagesGrammar Practice with Focus on Nouns, Numbers, Adjectives and AdverbsFelix HouNo ratings yet
- Healthy Living StyleDocument110 pagesHealthy Living StyleJacky ChanNo ratings yet
- Health Assessment FHP - Nutrition and MetabolismDocument25 pagesHealth Assessment FHP - Nutrition and MetabolismKim DajaoNo ratings yet
- Speech On EnglishDocument5 pagesSpeech On EnglishNagaretnam NagaNo ratings yet
- Don Mariano Marcos Memorial State University Campus Film Reveals Sugar's EffectsDocument3 pagesDon Mariano Marcos Memorial State University Campus Film Reveals Sugar's EffectsJinky FernandezNo ratings yet
- Causes of Obesity: Suzanne M. Wright, Louis J. AronneDocument3 pagesCauses of Obesity: Suzanne M. Wright, Louis J. AronneCarla Fernanda Sanhueza PozoNo ratings yet
- Reading Hobbies and HealthDocument18 pagesReading Hobbies and HealthNguyen NhanNo ratings yet
- Metabolism Clinical and Experimental: Anatoli Petridou, Aikaterina Siopi, Vassilis MougiosDocument7 pagesMetabolism Clinical and Experimental: Anatoli Petridou, Aikaterina Siopi, Vassilis MougiosUjian LancarNo ratings yet
- The Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthDocument28 pagesThe Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthThe Wilson Center100% (2)
- Cerita Dongengthe Smart DogDocument11 pagesCerita Dongengthe Smart DogNatalia KabanNo ratings yet
- Globalization's Impact on Food CultureDocument43 pagesGlobalization's Impact on Food CultureChristine Joy HufanaNo ratings yet
- Native American HealthDocument20 pagesNative American Healthapi-253792021No ratings yet
- Docteur (Ph. D) : Soutenance Publique de Thèse Pour L'obtention Du Grade de en Management International de La SantéDocument57 pagesDocteur (Ph. D) : Soutenance Publique de Thèse Pour L'obtention Du Grade de en Management International de La SantéDr Jean Berchmans NDARUSANZENo ratings yet
- The Blood Sugar Solution - Mark HymanDocument431 pagesThe Blood Sugar Solution - Mark HymanLi Lin100% (6)
- Chair Master-Exercise-Instructor-Manual-with-pictures PDFDocument64 pagesChair Master-Exercise-Instructor-Manual-with-pictures PDFonix2000100% (1)
- Clinical Screening Form - AgriSafe NetworkDocument4 pagesClinical Screening Form - AgriSafe NetworkAgriSafeNo ratings yet
- 7140SOHDocument6 pages7140SOHHarsha Vardhan LakshmipuramNo ratings yet
- Health and Hygiene Essentials for TeenagersDocument39 pagesHealth and Hygiene Essentials for Teenagersparisha dhebar100% (1)
- Senior Project Outline Salam ADocument3 pagesSenior Project Outline Salam Aapi-588486278No ratings yet
- A Clinical Profile of Metabolic Syndrome and Its Determinants Among Police Officers in BaliDocument5 pagesA Clinical Profile of Metabolic Syndrome and Its Determinants Among Police Officers in BaliDokter FebyanNo ratings yet
- Obesity Prevention and Education For School Nurses Community Health NursingDocument66 pagesObesity Prevention and Education For School Nurses Community Health NursingGabrielaNo ratings yet
- TES Harian: Bahasa InggrisDocument3 pagesTES Harian: Bahasa Inggris07 - Faizah Atiqah Maharani - 092No ratings yet
- Problem Lists Patient PlanDocument1 pageProblem Lists Patient Planangel23No ratings yet