You might also like
- Em Coding TablesDocument2 pagesEm Coding Tablesapi-270179959No ratings yet
- Myositis Core Set Measures of Activity Including The Mmt8 and Preliminary Definitions of Improvement 508Document25 pagesMyositis Core Set Measures of Activity Including The Mmt8 and Preliminary Definitions of Improvement 508Anonymous b2k9ABe7eNo ratings yet
- Therapy Worksheet (Page 1 of 2) : A. VALIDITY: Are The Results of This Single Preventive or Therapeutic Trial Valid?Document15 pagesTherapy Worksheet (Page 1 of 2) : A. VALIDITY: Are The Results of This Single Preventive or Therapeutic Trial Valid?andhikaNo ratings yet
- DHA Prometric 02-01-2014Document4 pagesDHA Prometric 02-01-2014Dr-Usman Khan80% (15)
- COAP Forum CollectionDocument6 pagesCOAP Forum Collectionprashmanic100% (1)
- Rheumatoid ArthritisDocument69 pagesRheumatoid ArthritisAditi HarerNo ratings yet
- DR Sandra S Langow SpPD-KRRA PIT IDI PDFDocument37 pagesDR Sandra S Langow SpPD-KRRA PIT IDI PDFAdisyari Puri HandiniNo ratings yet
- Immunologi 1Document47 pagesImmunologi 1Laboratorium Ansari SalehNo ratings yet
- 2010 Rheumatoid Arthritis Classification - EXCERPT 2010Document1 page2010 Rheumatoid Arthritis Classification - EXCERPT 2010Jocho NeavesNo ratings yet
- Feet Dont Fail Me Anymore Single Centre Results Using Low Dose Radiation Therapy For Feet Inflammatory Disorders and Review of Current EvidenceDocument12 pagesFeet Dont Fail Me Anymore Single Centre Results Using Low Dose Radiation Therapy For Feet Inflammatory Disorders and Review of Current EvidenceAthenaeum Scientific PublishersNo ratings yet
- Rheumatoid Arthritis - Assessment of Functional Performances of The PatientsDocument14 pagesRheumatoid Arthritis - Assessment of Functional Performances of The PatientsK. Vijay AnanthNo ratings yet
- Snot PontuaçãoDocument5 pagesSnot PontuaçãoCaio GonçalvesNo ratings yet
- SPN Lund Mackay and GosDocument3 pagesSPN Lund Mackay and GosMariaYoanitaAstrianiNo ratings yet
- Supplementary AppendixDocument18 pagesSupplementary AppendixRobertoNo ratings yet
- Classification CriteriaDocument1 pageClassification CriteriaLov Raj LohaniNo ratings yet
- Homework 3Document3 pagesHomework 3Cloud worldNo ratings yet
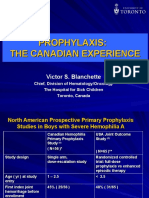
- GF2009 Victor S BlanchetteDocument23 pagesGF2009 Victor S Blanchettesorabhsharma35416No ratings yet
- OK Paper - Analysis of Oncology Studies For Programmers and Statisticians - 2018Document7 pagesOK Paper - Analysis of Oncology Studies For Programmers and Statisticians - 2018Laura SaglietiNo ratings yet
- Diagnostic Test: Magdalena SidhartaniDocument17 pagesDiagnostic Test: Magdalena SidhartaniPap PipNo ratings yet
- Therapy Worksheet (Page 1 ofDocument9 pagesTherapy Worksheet (Page 1 ofNararyasri HoeseinNo ratings yet
- Cópia de Meta-Analyses On HRV-thresholdsDocument49 pagesCópia de Meta-Analyses On HRV-thresholdsLeticia N. S. NevesNo ratings yet
- Ee121 Measurements and InstrumentationDocument62 pagesEe121 Measurements and InstrumentationJoseph Samir FaikNo ratings yet
- CEJPH 2023 03 178-183 Nechvatal 7767 3-1Document6 pagesCEJPH 2023 03 178-183 Nechvatal 7767 3-1ABIHANo ratings yet
- Oishi RecistDocument18 pagesOishi RecistJelena JovanovicNo ratings yet
- 03 Cadum Angelini 6 2 2014Document60 pages03 Cadum Angelini 6 2 2014Francesco AielloNo ratings yet
- Proportional Changes in Cephalometric Distances During Twin Block Appliance TherapyDocument8 pagesProportional Changes in Cephalometric Distances During Twin Block Appliance Therapyaddy yNo ratings yet
- Final Rheumatoid ArthritisDocument58 pagesFinal Rheumatoid ArthritisShivalingaiah GirishNo ratings yet
- SPSS2 Guide Basic Non-ParametricsDocument24 pagesSPSS2 Guide Basic Non-Parametricsrich_s_mooreNo ratings yet
- Management of Rheumatoid Arthritis: Consensus Recommendations From The Hong Kong Society of RheumatologyDocument11 pagesManagement of Rheumatoid Arthritis: Consensus Recommendations From The Hong Kong Society of RheumatologyMakhyan JibrilNo ratings yet
- Vibratin JudgementDocument9 pagesVibratin Judgementtovinny14159No ratings yet
- ACR-EULAR Gout Classification Criteria SlidesDocument53 pagesACR-EULAR Gout Classification Criteria SlideschizonaNo ratings yet
- s00296 012 2515 0Document4 pagess00296 012 2515 0Mia ZahirNo ratings yet
- Summary of OA Guideline Development ProcessDocument8 pagesSummary of OA Guideline Development ProcessomboNo ratings yet
- Shorter Treatment Duration For Selected Patients With Multidrug-Resistant TuberculosisDocument4 pagesShorter Treatment Duration For Selected Patients With Multidrug-Resistant Tuberculosispooja thanekarNo ratings yet
- Artrite Reumatoide: Uma Abordagem ContemporâneaDocument58 pagesArtrite Reumatoide: Uma Abordagem ContemporâneacarlosrschusterNo ratings yet
- MMC 1Document18 pagesMMC 1henryweiNo ratings yet
- Chapter IIDocument211 pagesChapter IIjonida88No ratings yet
- A Review and Analysis of The Mahalanobis Taguchi System PDFDocument16 pagesA Review and Analysis of The Mahalanobis Taguchi System PDFcualercowNo ratings yet
- Das 28Document2 pagesDas 28drtajamulhussainshah100% (1)
- Corse CheneauDocument17 pagesCorse Cheneauiguija6769No ratings yet
- Categorical Data AnalysisDocument44 pagesCategorical Data Analysisamonra10No ratings yet
- 3 - Evaluation and Management of Rheumatoid ArthritisDocument56 pages3 - Evaluation and Management of Rheumatoid ArthritisDwi Astika SariNo ratings yet
- Does Cardiac Rehabilitation Work in Chronic Heart Failure Patients? ... (And What Can We Learn From MetaDocument13 pagesDoes Cardiac Rehabilitation Work in Chronic Heart Failure Patients? ... (And What Can We Learn From MetaNicoletta OrphanouNo ratings yet
- The New ACR/EULAR Criteria For Rheumatoid Arthritis Can Identify Patients With Same Disease Activity But Less Damage by UltrasoundDocument4 pagesThe New ACR/EULAR Criteria For Rheumatoid Arthritis Can Identify Patients With Same Disease Activity But Less Damage by UltrasoundFajri WardiannurNo ratings yet
- Assessing Compatibility of Two Laboratories: Formulations As A Statistical Hypothesis Testing ProblemDocument12 pagesAssessing Compatibility of Two Laboratories: Formulations As A Statistical Hypothesis Testing Problemnauji_kNo ratings yet
- Diagnostic Performance of The ACR/EULAR 2010 Criteria For Rheumatoid Arthritis and Two Diagnostic Algorithms in An Early Arthritis Clinic (REACH)Document3 pagesDiagnostic Performance of The ACR/EULAR 2010 Criteria For Rheumatoid Arthritis and Two Diagnostic Algorithms in An Early Arthritis Clinic (REACH)Daniel Manay GuadalupeNo ratings yet
- BTL-6000 High Intensity Laser STUDY Microcirculation EN100 PreviewDocument4 pagesBTL-6000 High Intensity Laser STUDY Microcirculation EN100 PreviewNovaria Puspita SamudraNo ratings yet
- Scribd Upload A Document Search Documents Explore Sign Up Log inDocument23 pagesScribd Upload A Document Search Documents Explore Sign Up Log inNayan ThakurNo ratings yet
- Occupational Vibration in Urban Bus and Influence On Driver's Lower Limbs: A ReviewDocument11 pagesOccupational Vibration in Urban Bus and Influence On Driver's Lower Limbs: A ReviewMarko CvetkovićNo ratings yet
- Example ExamDocument3 pagesExample ExamDeepak KumarNo ratings yet
- Electronic Measurements and Instrumentation PPT SlidesDocument35 pagesElectronic Measurements and Instrumentation PPT SlidesAmit Shukla100% (3)
- 7909-Article Text-23014-1-10-20160830Document10 pages7909-Article Text-23014-1-10-20160830hafssa oukassouNo ratings yet
- Measrement Techniques - IIDocument40 pagesMeasrement Techniques - IIhani_chappidiNo ratings yet
- Interaction (Effect Modification) : Interaction Between Two Variables Is Said To Exist When The AssociationDocument22 pagesInteraction (Effect Modification) : Interaction Between Two Variables Is Said To Exist When The AssociationPalwasha MalikNo ratings yet
- Model Curriculum Diploma Production Engineering 040912Document202 pagesModel Curriculum Diploma Production Engineering 040912ab5918590No ratings yet
- Introduction To Taguchi TechniquesDocument13 pagesIntroduction To Taguchi TechniquesSreedhar Pugalendhi100% (1)
- CNCR 29602Document8 pagesCNCR 29602Joseph PerezNo ratings yet
- The Development of A New Orthosis (Neuro-Orthosis) For Patients With Carpal Tunnel Syndrome: Its Effect On The Function and Strength of The HandDocument19 pagesThe Development of A New Orthosis (Neuro-Orthosis) For Patients With Carpal Tunnel Syndrome: Its Effect On The Function and Strength of The HandSayan DeyNo ratings yet
- ArticleDocument2 pagesArticleamit_oncquestNo ratings yet
- Neuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodFrom EverandNeuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodNo ratings yet
- Systemic Lupus Erythematosus: A Systematic Approach to Arthritis of Rheumatic Diseases: Volume 4From EverandSystemic Lupus Erythematosus: A Systematic Approach to Arthritis of Rheumatic Diseases: Volume 4No ratings yet
- Paraffin Wax Bath: Sreeraj S RDocument20 pagesParaffin Wax Bath: Sreeraj S RMichael SelvarajNo ratings yet
- Tetralogy of FallotDocument3 pagesTetralogy of FallotJohn Mark PocsidioNo ratings yet
- "Destroyer and Teacher": Managing The Masses During The 1918-1919 Influenza PandemicDocument15 pages"Destroyer and Teacher": Managing The Masses During The 1918-1919 Influenza PandemicJavier BassiNo ratings yet
- Pneumonia in Immunocompromised Patients: Respirology (2009) 14 (Suppl. 2) S44 - S50Document7 pagesPneumonia in Immunocompromised Patients: Respirology (2009) 14 (Suppl. 2) S44 - S50intankmlsNo ratings yet
- 2018 - Early Diagnosis and Detection of Breast Cancer - Milosevic2018Document31 pages2018 - Early Diagnosis and Detection of Breast Cancer - Milosevic2018Adriano R. OrtizNo ratings yet
- Augmentin SyrDocument4 pagesAugmentin Syross-20502745No ratings yet
- Critical Appraisal On Systematic ReviewsDocument22 pagesCritical Appraisal On Systematic ReviewsDesiree MejicaNo ratings yet
- Latest Cva 1...Document57 pagesLatest Cva 1...eric macabiogNo ratings yet
- 8223-Article Text-34619-3-10-20230704Document6 pages8223-Article Text-34619-3-10-20230704Dea NopiantiNo ratings yet
- TREATMENTDocument9 pagesTREATMENTMae LibreNo ratings yet
- Review of System Done... 1Document2 pagesReview of System Done... 1Dheng EsquijoNo ratings yet
- Downtime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimeDocument5 pagesDowntime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimerupaliNo ratings yet
- Woldia University College of Health Science Department of NursingDocument28 pagesWoldia University College of Health Science Department of Nursingmezgebu aysheshimNo ratings yet
- 401H Report BioHealth 7 16 PDFDocument1 page401H Report BioHealth 7 16 PDFgreatgeniusNo ratings yet
- Siadh - Patho, Signs, Causes, TreatmentDocument1 pageSiadh - Patho, Signs, Causes, TreatmentVishalNo ratings yet
- DermatologyDocument44 pagesDermatologymumunooNo ratings yet
- Kidney CancerDocument6 pagesKidney CancerAKHILNo ratings yet
- ++serrapeptase The Miracle EnzymeDocument2 pages++serrapeptase The Miracle EnzymeabazanNo ratings yet
- Mechanism of InfectionDocument3 pagesMechanism of Infectionshyamsunder68100% (5)
- ShockDocument29 pagesShockKoRnflakes100% (4)
- Level of Breast Cancer Awareness On Fourth-Year FemaleDocument28 pagesLevel of Breast Cancer Awareness On Fourth-Year FemaleLafayette Kirsi NoelNo ratings yet
- Should I Stop Being A Perfectionist?Document3 pagesShould I Stop Being A Perfectionist?Maia GroisNo ratings yet
- Anaesthesia RCOphth GuidelinesDocument4 pagesAnaesthesia RCOphth GuidelinesDiana SmithNo ratings yet
- Afar Biomarkers of Aging 2016 PDFDocument4 pagesAfar Biomarkers of Aging 2016 PDFPD SNo ratings yet
- GOLD Report Portugues Mais Respeitada Guideline DpocDocument127 pagesGOLD Report Portugues Mais Respeitada Guideline Dpocizacbug100% (1)
- Pharmacology Questions From HypertensionDocument7 pagesPharmacology Questions From HypertensionNeha Roy100% (4)
- Funding Vaccines For Emerging Infectious DiseasesDocument4 pagesFunding Vaccines For Emerging Infectious Diseasesfadfdafade uohdajufadNo ratings yet
- Polycystic Kidney DiseaseDocument21 pagesPolycystic Kidney DiseasePrifate Beheljambi100% (1)