You might also like
- Health Education - Lecture Notes PDFDocument60 pagesHealth Education - Lecture Notes PDFPetros Ndumba100% (8)
- Module - I: 2.Milio'S Framework For PreventionDocument26 pagesModule - I: 2.Milio'S Framework For PreventionIanaCarandang100% (3)
- Policy and Procedures For Hiring, PromotionsDocument2 pagesPolicy and Procedures For Hiring, PromotionsRazel Ann ElagioNo ratings yet
- Escape From The Western Diet Summary RevisedDocument3 pagesEscape From The Western Diet Summary Revisedapi-385530863100% (1)
- 2014 - Does Health Coaching WorkDocument25 pages2014 - Does Health Coaching WorkGONDHES CHANNELNo ratings yet
- Health Promotion: An Integral Discipline of Public HealthDocument6 pagesHealth Promotion: An Integral Discipline of Public HealthUsman Ahmad TijjaniNo ratings yet
- Practicing Health Promotion in Primary CareDocument6 pagesPracticing Health Promotion in Primary CareAlfia NadiraNo ratings yet
- Part 1 Jennie Naidoo - Jane Wills, MSC - Developing Practice For Public Health and Health Promotion-Bailliere Tindall - Elsevier (2010) (1) (018-092)Document75 pagesPart 1 Jennie Naidoo - Jane Wills, MSC - Developing Practice For Public Health and Health Promotion-Bailliere Tindall - Elsevier (2010) (1) (018-092)flameglitter21No ratings yet
- Health Promotion Strategies For NursesDocument2 pagesHealth Promotion Strategies For Nursespuding101No ratings yet
- DownloadDocument12 pagesDownloadMUHAMMAD FARIS SASMANNo ratings yet
- Research ArticleDocument32 pagesResearch ArticleEliezer NuenayNo ratings yet
- Ethics and Evidence - An Alternative View of HPDocument9 pagesEthics and Evidence - An Alternative View of HPTerence FusireNo ratings yet
- HIA Guide For PracticeDocument89 pagesHIA Guide For PracticeMariamNo ratings yet
- AJGP 10 2019 Focus Conn Health Coaching Lifestyle Medicine WEB 1Document4 pagesAJGP 10 2019 Focus Conn Health Coaching Lifestyle Medicine WEB 1Lely jumriani baktiNo ratings yet
- Health Promotion PGDocument16 pagesHealth Promotion PGp.gargNo ratings yet
- Health Promotion and Health Education: Bardarash Technical Institute Nursing DepartmentDocument36 pagesHealth Promotion and Health Education: Bardarash Technical Institute Nursing Departmentarazw IssaNo ratings yet
- Sách theo dõi đánh giá chương trình y tếDocument19 pagesSách theo dõi đánh giá chương trình y tếTran Quyet TienNo ratings yet
- 2nd CLASS ENG - HEALTH PROMOTIONDocument3 pages2nd CLASS ENG - HEALTH PROMOTIONS VaibhavNo ratings yet
- Health Promotion Models - PHOP 4 2017 - 2018 - YFDocument58 pagesHealth Promotion Models - PHOP 4 2017 - 2018 - YFFaishalNo ratings yet
- AH RI Quality Improvement UASDocument5 pagesAH RI Quality Improvement UASSrikit NurkamidenNo ratings yet
- Atestados de La Rueda de Cambio de ComportamientoDocument7 pagesAtestados de La Rueda de Cambio de Comportamientovero060112.vcNo ratings yet
- CCM: Community: Sumberdaya Dan Kebijakan KomunitasDocument53 pagesCCM: Community: Sumberdaya Dan Kebijakan KomunitasAlvinNo ratings yet
- Health PromotionDocument16 pagesHealth PromotionSushma LathNo ratings yet
- Integrated Theory of Health Behavior Change - Background and Intervention DevelopmentDocument10 pagesIntegrated Theory of Health Behavior Change - Background and Intervention Developmentvero060112.vcNo ratings yet
- Phpe 210Document2 pagesPhpe 210Reg LagartejaNo ratings yet
- 1 - Method-and-Approaches of HPDocument63 pages1 - Method-and-Approaches of HPPutri EsaNo ratings yet
- Unit 3-Health Promotion and DiversityDocument37 pagesUnit 3-Health Promotion and DiversityKrista KloseNo ratings yet
- Lesson Plane On Health Promotion.Document6 pagesLesson Plane On Health Promotion.Topeshwar TpkNo ratings yet
- Nursing Process in The Care of The POPULATION GROUPSDocument3 pagesNursing Process in The Care of The POPULATION GROUPSCailah Sofia SelausoNo ratings yet
- Approaches To Health PromotionDocument4 pagesApproaches To Health PromotionJade Xy MasculinoNo ratings yet
- Health PromotionDocument30 pagesHealth PromotionZareen Tasnim Tapti 2225036080No ratings yet
- International Journal of Nursing Studies: ArticleinfoDocument16 pagesInternational Journal of Nursing Studies: Articleinfodewi retnoNo ratings yet
- Aminu Magaji T-PDocument27 pagesAminu Magaji T-PUsman Ahmad TijjaniNo ratings yet
- Materi - Method and Approaches in HPDocument98 pagesMateri - Method and Approaches in HPdiniindahlestariNo ratings yet
- Healthpromotion 190406154250Document77 pagesHealthpromotion 190406154250Latuloho Malay Colo MochoNo ratings yet
- UntitledDocument21 pagesUntitledSan MohapatraNo ratings yet
- Band UraDocument23 pagesBand UraAnonymous FTdGFgNo ratings yet
- A1 Introduction To Health PromotionDocument17 pagesA1 Introduction To Health PromotionAfia SarpongNo ratings yet
- Community Health EducationDocument5 pagesCommunity Health EducationCharlene LunaNo ratings yet
- Improving Health and Reducing Inequalities A Practical Guide To HIA - WAG Wales - 2004Document36 pagesImproving Health and Reducing Inequalities A Practical Guide To HIA - WAG Wales - 2004PublicHealthbyDesignNo ratings yet
- Tacking The Wider Determinants of Health InequalityDocument8 pagesTacking The Wider Determinants of Health InequalitymammaofxyzNo ratings yet
- Health Services System ManagementDocument21 pagesHealth Services System ManagementShimmering MoonNo ratings yet
- Activity 4-PHDocument5 pagesActivity 4-PHKate MendozaNo ratings yet
- Beacon Schools Project Health Education Level 8 Planning Guide Section 6Document8 pagesBeacon Schools Project Health Education Level 8 Planning Guide Section 6api-3803295No ratings yet
- Sexual & Reproductive Healthcare: EditorialDocument2 pagesSexual & Reproductive Healthcare: Editorialardian jayakusumaNo ratings yet
- Social Cognitive Theory - Bandura - Health Promotion by Social Cognitive Means - 2004 PDFDocument22 pagesSocial Cognitive Theory - Bandura - Health Promotion by Social Cognitive Means - 2004 PDFZuzu FinusNo ratings yet
- Health Promotion ModelDocument5 pagesHealth Promotion ModelMakau ElijahNo ratings yet
- Health Promot. Int.-2008-Tannahill-380-90Document11 pagesHealth Promot. Int.-2008-Tannahill-380-90Terence FusireNo ratings yet
- Paparan Semnas Promkes-Sapja AnantanyuDocument25 pagesPaparan Semnas Promkes-Sapja AnantanyuyuliaNo ratings yet
- Pabo - GOOD HEALTH AND WELL-BEINGDocument4 pagesPabo - GOOD HEALTH AND WELL-BEINGPA-PABO, Christine Jane A.No ratings yet
- Advantages and Disadvantages of Health Care AccredDocument32 pagesAdvantages and Disadvantages of Health Care Accredgiuliano moralesNo ratings yet
- Je CH 082743Document8 pagesJe CH 082743Anggriyani Wahyu PinandariNo ratings yet
- What Strategies Help To Promote The Health of Individuals?Document1 pageWhat Strategies Help To Promote The Health of Individuals?FlaaffyNo ratings yet
- What Are Health Information Systems, and Why Are They Important?Document7 pagesWhat Are Health Information Systems, and Why Are They Important?Malick GaiNo ratings yet
- Col Zulfiquer Ahmed Amin: M Phil (HHM), MPH (HM), PGD (Health Economics), MBBS Armed Forces Medical Institute (AFMI)Document60 pagesCol Zulfiquer Ahmed Amin: M Phil (HHM), MPH (HM), PGD (Health Economics), MBBS Armed Forces Medical Institute (AFMI)Manav Suman SinghNo ratings yet
- Health Promotion and Health Education 11.24.22Document99 pagesHealth Promotion and Health Education 11.24.22Compilation 2021No ratings yet
- C1 NCM 102Document20 pagesC1 NCM 102Khecia Freanne TorresNo ratings yet
- Health Literacy: Applying Current Concepts To Improve Health Services and Reduce Health InequalitiesDocument10 pagesHealth Literacy: Applying Current Concepts To Improve Health Services and Reduce Health InequalitiesasriadiNo ratings yet
- Knowledge Translation and Behaviour Change: Patients, Providers, and PopulationsDocument2 pagesKnowledge Translation and Behaviour Change: Patients, Providers, and PopulationsyodaNo ratings yet
- NR527 Module 3 (Health Promotion)Document5 pagesNR527 Module 3 (Health Promotion)96rubadiri96No ratings yet
- What Is Peer Education and How Peer Education Is Used - AdetDocument4 pagesWhat Is Peer Education and How Peer Education Is Used - AdetFamelasari Fitria RamdaniNo ratings yet
- برنامج الهندسة الكهربائيةDocument2 pagesبرنامج الهندسة الكهربائيةS AbdNo ratings yet
- Skit PDFDocument6 pagesSkit PDFPeterJLYNo ratings yet
- How To Publish A Scientific Manuscript in A High-Impact JournalDocument5 pagesHow To Publish A Scientific Manuscript in A High-Impact JournalS AbdNo ratings yet
- Comparision of PSO and GADocument13 pagesComparision of PSO and GAEswaranNo ratings yet
- A Survey of Fractional Order Calculus Applications of Multiple-Input, Multiple-Output (MIMO) Process ControlDocument32 pagesA Survey of Fractional Order Calculus Applications of Multiple-Input, Multiple-Output (MIMO) Process ControlS AbdNo ratings yet
- Soil Biology and BiochemistryDocument3 pagesSoil Biology and BiochemistryS AbdNo ratings yet
- Chaos, Solitons and Fractals: Vinay Kumar Reddy Chimmula, Lei ZhangDocument6 pagesChaos, Solitons and Fractals: Vinay Kumar Reddy Chimmula, Lei ZhangS AbdNo ratings yet
- Soil Biology and BiochemistryDocument3 pagesSoil Biology and BiochemistryS AbdNo ratings yet
- Soil Biology and BiochemistryDocument3 pagesSoil Biology and BiochemistryS AbdNo ratings yet
- 10 1016@j Ijleo 2020 165155 PDFDocument19 pages10 1016@j Ijleo 2020 165155 PDFS AbdNo ratings yet
- Research On Position Servo System Based On FractioDocument10 pagesResearch On Position Servo System Based On FractioS AbdNo ratings yet
- Filtering and ConvolutionsDocument15 pagesFiltering and ConvolutionssoumikbhNo ratings yet
- Hamiltonian-Based Energy Analysis For Brushless DC Motor Chaotic SystemDocument14 pagesHamiltonian-Based Energy Analysis For Brushless DC Motor Chaotic SystemS AbdNo ratings yet
- Supersymmetric Artificial Neural Network 2Document5 pagesSupersymmetric Artificial Neural Network 2S AbdNo ratings yet
- 12 29 11editionDocument27 pages12 29 11editionSan Mateo Daily JournalNo ratings yet
- May 2 Homework Solutions: S M X CDocument3 pagesMay 2 Homework Solutions: S M X CClerry SamuelNo ratings yet
- Problem 21-02 Wright Company Spreadsheet For The Statement of Cash Flows Dec. 31 Changes Dec. 31 2020 Debits Credits 2021 Balance SheetDocument17 pagesProblem 21-02 Wright Company Spreadsheet For The Statement of Cash Flows Dec. 31 Changes Dec. 31 2020 Debits Credits 2021 Balance SheetVishal P RaoNo ratings yet
- Research 101Document14 pagesResearch 101Ace Ryu SmithNo ratings yet
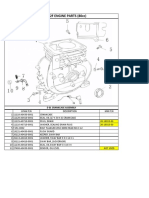
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Arduino CertificationDocument8 pagesArduino Certificationhack reportNo ratings yet
- PSV Sizing For Two Phase FlowDocument28 pagesPSV Sizing For Two Phase FlowSyed Haideri100% (1)
- PBL 3 - Toothache Drugs and MedicationsDocument10 pagesPBL 3 - Toothache Drugs and MedicationsAlbert LawNo ratings yet
- Week 1Document14 pagesWeek 1kohalehNo ratings yet
- Chapter 3 - Assessment of PostureDocument31 pagesChapter 3 - Assessment of Posturehis.thunder122No ratings yet
- Korean Wellhead KWM-2014-Revision0Document20 pagesKorean Wellhead KWM-2014-Revision0DrakkarNo ratings yet
- Arrival Guide To MalaysiaDocument2 pagesArrival Guide To Malaysiaamanu092No ratings yet
- Internship-Plan BSBA FInalDocument2 pagesInternship-Plan BSBA FInalMark Altre100% (1)
- Banana Disease 2 PDFDocument4 pagesBanana Disease 2 PDFAlimohammad YavariNo ratings yet
- Production & Downstream Processing of Baker's Best FriendDocument26 pagesProduction & Downstream Processing of Baker's Best FriendMelissaNo ratings yet
- Lab Manual For Series Parallel Rasonant CircuitDocument3 pagesLab Manual For Series Parallel Rasonant CircuitManoj PardhanNo ratings yet
- Brown Wolf ExerciseDocument8 pagesBrown Wolf ExerciseAarnav kumar0% (1)
- Distance Learning in Clinical MedicalDocument7 pagesDistance Learning in Clinical MedicalGeraldine Junchaya CastillaNo ratings yet
- Gastrointestinal Tract PDFDocument3 pagesGastrointestinal Tract PDFAlexandra Suan CatambingNo ratings yet
- "Unadulterated" - The Organic and Ethnic - For Vegetarians and Non-VegetariansDocument21 pages"Unadulterated" - The Organic and Ethnic - For Vegetarians and Non-VegetariansShilpa PatilNo ratings yet
- Physical, Biology and Chemical Environment: Its Effect On Ecology and Human HealthDocument24 pagesPhysical, Biology and Chemical Environment: Its Effect On Ecology and Human Health0395No ratings yet
- SyllabusDocument2 pagesSyllabusPrakash KumarNo ratings yet
- Quality Control Argex 0032/32.50.15.08 4/10 MM EN 13055: EN 15732 NL BSB K73820/01 (1/01/2004)Document1 pageQuality Control Argex 0032/32.50.15.08 4/10 MM EN 13055: EN 15732 NL BSB K73820/01 (1/01/2004)joe briffaNo ratings yet
- Alabama Religious Exemption AdvisoryDocument1 pageAlabama Religious Exemption AdvisoryABC 33/40No ratings yet
- Income Taxation Module Compilation FinalsDocument107 pagesIncome Taxation Module Compilation FinalsJasmine CardinalNo ratings yet
- Substation Off Line and Hot Line CommissioningDocument3 pagesSubstation Off Line and Hot Line CommissioningMohammad JawadNo ratings yet
- Cockerspaniel Pra CarriersDocument28 pagesCockerspaniel Pra CarriersJo M. ChangNo ratings yet
- 1-A Colored Substance That Is Spread Over A Surface and Dries To Leave A Thin Decorative or Protective Coating. Decorative or Protective CoatingDocument60 pages1-A Colored Substance That Is Spread Over A Surface and Dries To Leave A Thin Decorative or Protective Coating. Decorative or Protective Coatingjoselito lacuarinNo ratings yet