You might also like
- Health Promotion PGDocument16 pagesHealth Promotion PGp.gargNo ratings yet
- Health PromotionDocument50 pagesHealth PromotionKailash NagarNo ratings yet
- Health PromotionDocument30 pagesHealth PromotionZareen Tasnim Tapti 2225036080No ratings yet
- Health PromotionDocument51 pagesHealth PromotionKailash NagarNo ratings yet
- Foundations of Health Promotion MODULEDocument143 pagesFoundations of Health Promotion MODULEAndrew100% (2)
- Lecture-1: University of Kufa Faculty of Nursing, Community Health Nursing BranchDocument27 pagesLecture-1: University of Kufa Faculty of Nursing, Community Health Nursing Branchآمنة محمد كاظمNo ratings yet
- Lecture 2 Public Health Nutrition - Health Promotion and Theories of Behaviour Change-1Document98 pagesLecture 2 Public Health Nutrition - Health Promotion and Theories of Behaviour Change-1Eric MensahNo ratings yet
- PBH 203 - Health Promotion - PBH 203 - Latest-2Document56 pagesPBH 203 - Health Promotion - PBH 203 - Latest-2Ajao RukayatNo ratings yet
- Healthpromotlectamany 150627111718 Lva1 App6892Document56 pagesHealthpromotlectamany 150627111718 Lva1 App6892B 70 Mohit KumarNo ratings yet
- Health Promotion and EducationDocument75 pagesHealth Promotion and EducationDaniel DubeNo ratings yet
- CHN MIdterms DiscussionDocument60 pagesCHN MIdterms DiscussionShaira PacallesNo ratings yet
- Health Education & Behaviour Change CommunicationDocument50 pagesHealth Education & Behaviour Change CommunicationAarya MathewNo ratings yet
- What Is Health PromotionDocument2 pagesWhat Is Health PromotionKen MelendezNo ratings yet
- Milestones Health Promotion 05022010Document42 pagesMilestones Health Promotion 05022010Claire Cassar100% (1)
- Healthpromotion 190406154250Document77 pagesHealthpromotion 190406154250Latuloho Malay Colo MochoNo ratings yet
- 11 Health PromotionDocument172 pages11 Health PromotionJalalNo ratings yet
- Global Programme On Health Promotion Effectiveness: Dewirokhmah@unej - Ac.idDocument35 pagesGlobal Programme On Health Promotion Effectiveness: Dewirokhmah@unej - Ac.idNurul FadilahNo ratings yet
- MPU3313 MPU2313 Topic 6Document26 pagesMPU3313 MPU2313 Topic 6CheAzahariCheAhmad100% (1)
- Strategies for Health PromotionDocument15 pagesStrategies for Health PromotionpuskesmasNo ratings yet
- Primary Health Care: A Foundation for Universal Health CoverageDocument43 pagesPrimary Health Care: A Foundation for Universal Health CoverageShyla Bantolinao100% (1)
- Health Promotion: Enabling Control and Improving HealthDocument23 pagesHealth Promotion: Enabling Control and Improving HealthPrimalj Pinnaduwa100% (1)
- Global Programme On Health Promotion Effectiveness: Dewirokhmah@unej - Ac.idDocument35 pagesGlobal Programme On Health Promotion Effectiveness: Dewirokhmah@unej - Ac.idNurul FadilahNo ratings yet
- The Ottawa Charter For Health PromotionDocument8 pagesThe Ottawa Charter For Health PromotionnipoNo ratings yet
- Activity 4-PHDocument5 pagesActivity 4-PHKate MendozaNo ratings yet
- 2nd CLASS ENG - HEALTH PROMOTIONDocument3 pages2nd CLASS ENG - HEALTH PROMOTIONS VaibhavNo ratings yet
- Setting Realistic GoalsDocument13 pagesSetting Realistic GoalsNhadz AgagonNo ratings yet
- History of HPDocument45 pagesHistory of HPNicole MedinaNo ratings yet
- HEALTH PROMOTION PRINCIPLESDocument16 pagesHEALTH PROMOTION PRINCIPLESSushma LathNo ratings yet
- A1 Introduction To Health PromotionDocument17 pagesA1 Introduction To Health PromotionAfia SarpongNo ratings yet
- Health Promotion StrategiesDocument27 pagesHealth Promotion StrategiesAsal Salah100% (1)
- Health Promotion Principles ValuesDocument49 pagesHealth Promotion Principles Valuesfaltarion66100% (3)
- Public HealthDocument25 pagesPublic HealthMuhammad Saim Bin SaeedNo ratings yet
- OttawaDocument4 pagesOttawaangie Linett Quina ArboledaNo ratings yet
- Health Promotion Models - PHOP 4 2017 - 2018 - YFDocument58 pagesHealth Promotion Models - PHOP 4 2017 - 2018 - YFFaishalNo ratings yet
- Liberia - National Policy and Strategic Plan On Health Promotion, 2016 - 2021Document44 pagesLiberia - National Policy and Strategic Plan On Health Promotion, 2016 - 2021Rémi DANHOUNDONo ratings yet
- Child To Child ApproachDocument18 pagesChild To Child ApproachPalwasha KhanNo ratings yet
- Health PromotionDocument36 pagesHealth PromotionJhaji Mei Margarete CasiNo ratings yet
- Basics of Health Promotion 2Document48 pagesBasics of Health Promotion 2Mathews showsNo ratings yet
- Health Promotion and Health Education 11.24.22Document99 pagesHealth Promotion and Health Education 11.24.22Compilation 2021No ratings yet
- Applying Indigenous Models Pasifika Health PromotionDocument36 pagesApplying Indigenous Models Pasifika Health Promotionpritikachand100% (1)
- Ottawa Charter For HPDocument5 pagesOttawa Charter For HPRoberto Cláudio CordeiroNo ratings yet
- PHN PrinciplesDocument47 pagesPHN PrinciplesSarah MumbaNo ratings yet
- BCMH201 HEALTH PROMOTIONSpdfDocument11 pagesBCMH201 HEALTH PROMOTIONSpdfYeboah Kukudabi AsiamahNo ratings yet
- PROMOSI KESEHATAN Pertemuan 1 & 2 2019 DosenDocument33 pagesPROMOSI KESEHATAN Pertemuan 1 & 2 2019 DosenRirin SetiyaniNo ratings yet
- Summary of HP TermsDocument5 pagesSummary of HP TermsMayom MabuongNo ratings yet
- Ottawa Charter For Health PromotionDocument5 pagesOttawa Charter For Health PromotionEleanorNo ratings yet
- AJOT 743003 OT Promotion Health Well BeingDocument19 pagesAJOT 743003 OT Promotion Health Well BeingTimothy Webb JrNo ratings yet
- Health EducationDocument220 pagesHealth EducationMihretNo ratings yet
- Dasar Promosi KesehatanDocument34 pagesDasar Promosi KesehatansaintJelitaNo ratings yet
- Current Issues and Challenges of HealthDocument12 pagesCurrent Issues and Challenges of HealthSitti KcNo ratings yet
- Ottawa Charter for Health PromotionDocument4 pagesOttawa Charter for Health PromotionMayom MabuongNo ratings yet
- Community Development Approaches To Health PromotionDocument35 pagesCommunity Development Approaches To Health PromotionOana Sorina AndronicNo ratings yet
- (Leon Gordis) Epidemiology (4th Edition)Document26 pages(Leon Gordis) Epidemiology (4th Edition)Anna Dixon100% (1)
- Promoting Health Education for Sustainable Health BehaviorDocument25 pagesPromoting Health Education for Sustainable Health BehavioryuliaNo ratings yet
- The Ottawa Charter For Health PromotionDocument5 pagesThe Ottawa Charter For Health PromotionANA LILIA CALDERON YELANo ratings yet
- Health Promotion and Health EducationDocument2 pagesHealth Promotion and Health EducationYetri MulizaNo ratings yet
- Healthy Public Policy: The Five Major Areas/Strategies in Health Promotion (Ottawa Charter)Document11 pagesHealthy Public Policy: The Five Major Areas/Strategies in Health Promotion (Ottawa Charter)Johnjohn MateoNo ratings yet
- Col Zulfiquer Ahmed Amin: M Phil (HHM), MPH (HM), PGD (Health Economics), MBBS Armed Forces Medical Institute (AFMI)Document60 pagesCol Zulfiquer Ahmed Amin: M Phil (HHM), MPH (HM), PGD (Health Economics), MBBS Armed Forces Medical Institute (AFMI)Manav Suman SinghNo ratings yet
- Waterborne Diseases LectureDocument28 pagesWaterborne Diseases LectureManav Suman SinghNo ratings yet
- Waterpurificationmethods 160905063859 PDFDocument20 pagesWaterpurificationmethods 160905063859 PDFmuhammadNo ratings yet
- Purification of Water: by Sanjay GeorgeDocument26 pagesPurification of Water: by Sanjay GeorgeManav Suman Singh0% (1)
- Mini-Mental State Exam For Children (MMC) in Children With Hemiplegic Cerebral PalsyDocument10 pagesMini-Mental State Exam For Children (MMC) in Children With Hemiplegic Cerebral PalsyJéssica ArquivosNo ratings yet
- Urge Surfing HandoutDocument1 pageUrge Surfing HandoutRene McLaughlinNo ratings yet
- Date & Time Focus Data Action Response D: Into OR, A - Year Old - PerDocument2 pagesDate & Time Focus Data Action Response D: Into OR, A - Year Old - PerMichelle Gliselle Guinto MallareNo ratings yet
- UCT Postgraduate-Studies BrochureDocument27 pagesUCT Postgraduate-Studies BrochureUsman AhmedNo ratings yet
- CrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)Document5 pagesCrossFit®-Injury Prevalence and Main Risk Factors (Curiosidade)TUTOR PAULO EDUARDO REDKVANo ratings yet
- EMP 412 - Teaching - Notes - Topic - 1 - Economics - of - Education - and - Human - Capital - Theory - 1Document17 pagesEMP 412 - Teaching - Notes - Topic - 1 - Economics - of - Education - and - Human - Capital - Theory - 1Saka FelistarNo ratings yet
- Experienced Pharmacist Seeking New OpportunityDocument3 pagesExperienced Pharmacist Seeking New OpportunityIman ElshafieNo ratings yet
- Pharmaceutical Marketing: Marketing Strategy Alternative Strategic ThrustsDocument29 pagesPharmaceutical Marketing: Marketing Strategy Alternative Strategic Thrustspremoshin100% (4)
- Teen Breathe June2020Document70 pagesTeen Breathe June2020Екатерина Кедрина100% (1)
- Physical Education and Health 2 - Grade 11 NotesDocument6 pagesPhysical Education and Health 2 - Grade 11 NotesPedro HampaslupaNo ratings yet
- ABP - MPDO Lakkireddy Palli Mandal Approved LetterDocument3 pagesABP - MPDO Lakkireddy Palli Mandal Approved Letterchild development project officer lakkireddypalliNo ratings yet
- ABM Applied Economics Module 2 Examine The Utility and Application of of Applied Economics To Solve Economic Issues and ProblemsDocument29 pagesABM Applied Economics Module 2 Examine The Utility and Application of of Applied Economics To Solve Economic Issues and Problemsmara ellyn lacson100% (8)
- bài thầy thông (E)Document42 pagesbài thầy thông (E)SumaleeNo ratings yet
- Narrative ReportDocument2 pagesNarrative ReportRhisia RaborNo ratings yet
- P.E 1 - Module - First Quarter - Health Behavior and Risk FactorsDocument30 pagesP.E 1 - Module - First Quarter - Health Behavior and Risk Factorsjohn charles garaldeNo ratings yet
- Legalize ItDocument2 pagesLegalize Itaisar aisarNo ratings yet
- Csec English SbaDocument16 pagesCsec English Sbamartenio martin65% (31)
- Seligman Attributional Style QuestionnaireDocument14 pagesSeligman Attributional Style QuestionnaireAnjali VyasNo ratings yet
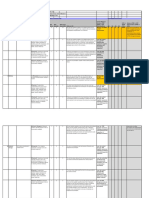
- PROCESS - Risk Assessment & HACCP Planning: Section 7.4.1Document4 pagesPROCESS - Risk Assessment & HACCP Planning: Section 7.4.1Wisnu samuel Atmaja triwarsitaNo ratings yet
- Community Engagement, Solidarity and Citizenship: Module 5 - Quarter 1Document28 pagesCommunity Engagement, Solidarity and Citizenship: Module 5 - Quarter 1Benjamin Fernandez Jr.67% (3)
- Middle East CaravanDocument20 pagesMiddle East CaravanB2B AFRICANo ratings yet
- Recruitment MSCDocument40 pagesRecruitment MSCViji MNo ratings yet
- Bionic Final PDFDocument4 pagesBionic Final PDFJasmine RaoNo ratings yet
- Vague X The Skateboard Physiotherapist - Isolation GuideDocument12 pagesVague X The Skateboard Physiotherapist - Isolation GuideKiko Lorman AlvarezNo ratings yet
- 175 Hys, Matuszek, Olejnik, BierczyńskiDocument9 pages175 Hys, Matuszek, Olejnik, BierczyńskiRadek PolonusNo ratings yet
- Immediate Dentures ExplainedDocument64 pagesImmediate Dentures ExplainedDHANASRI MOTAPARTHYNo ratings yet
- What Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasDocument24 pagesWhat Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasAisa VenturaNo ratings yet
- AL CIERRE DE Julio Del 2021: Barra COD AlfabetaDocument2 pagesAL CIERRE DE Julio Del 2021: Barra COD AlfabetaBrian Javier GomezNo ratings yet
- The Process of PhlebotomyDocument102 pagesThe Process of PhlebotomyCatherine Merilleno100% (1)
- 1st Summative Test in in English 6 Q1 Answer KeyDocument4 pages1st Summative Test in in English 6 Q1 Answer KeyGessle GamirNo ratings yet