You might also like
- Peritoneal Dialysis Manual: A Guide for Understanding the TreatmentFrom EverandPeritoneal Dialysis Manual: A Guide for Understanding the TreatmentRating: 5 out of 5 stars5/5 (1)
- 12 Strokes: A Case-based Guide to Acute Ischemic Stroke ManagementFrom Everand12 Strokes: A Case-based Guide to Acute Ischemic Stroke ManagementFerdinand K. HuiNo ratings yet
- 1 s2.0 S1053077022009168 MainDocument8 pages1 s2.0 S1053077022009168 MainOttofianus Alvedo Hewick KalangiNo ratings yet
- Research Article: Early Tracheostomy May Reduce The Length of Hospital StayDocument4 pagesResearch Article: Early Tracheostomy May Reduce The Length of Hospital Stayusus sapiNo ratings yet
- Ivac 176Document5 pagesIvac 176Issa AbuzeidNo ratings yet
- Long-Term Outcome Following Tracheostomy in Critical Care: A Systematic ReviewDocument12 pagesLong-Term Outcome Following Tracheostomy in Critical Care: A Systematic ReviewsemnasNo ratings yet
- 3association of Early Vs Late Tracheostomy Placement 2021Document10 pages3association of Early Vs Late Tracheostomy Placement 2021Cường Nguyễn HùngNo ratings yet
- Effect of Early Tracheostomy in Mechanically Ventilated PatientsDocument8 pagesEffect of Early Tracheostomy in Mechanically Ventilated PatientsManuel Cuevas EspinozaNo ratings yet
- Timing of Tracheostomy in Patients With Prolonged Endotracheal Intubation: A Systematic ReviewDocument12 pagesTiming of Tracheostomy in Patients With Prolonged Endotracheal Intubation: A Systematic ReviewCassie AbernathNo ratings yet
- Hubungan Antara Jarak Waktu Trakeostomi Dengan Mortalitas Pasien Kritis Ter20200505-4830-19g01dw-With-cover-page-V2Document10 pagesHubungan Antara Jarak Waktu Trakeostomi Dengan Mortalitas Pasien Kritis Ter20200505-4830-19g01dw-With-cover-page-V2IswandiNo ratings yet
- Treatment of Chronic Lateral Epicondylosis RCT 2022-1Document11 pagesTreatment of Chronic Lateral Epicondylosis RCT 2022-1chan kyoNo ratings yet
- Jurnal Cts 2Document10 pagesJurnal Cts 2Muhammad Hanafi QNo ratings yet
- 12Hiệu quả mở kq sớm pt gộp 2015Document10 pages12Hiệu quả mở kq sớm pt gộp 2015Cường Nguyễn HùngNo ratings yet
- 2022-10# (PEERJ) RR in ECMODocument17 pages2022-10# (PEERJ) RR in ECMOjycntuNo ratings yet
- Operative Treatment of Terrible Triad of TheDocument8 pagesOperative Treatment of Terrible Triad of TheAndrea OsborneNo ratings yet
- Impact On Survival On Interval Between Surgery andDocument10 pagesImpact On Survival On Interval Between Surgery andZamekile LukheleNo ratings yet
- 268 2017 Article 4420Document6 pages268 2017 Article 4420Naily Nuzulur RohmahNo ratings yet
- Mertens2021 Article TransthoracicVersusTranshiatalDocument9 pagesMertens2021 Article TransthoracicVersusTranshiatalDr Shiv ChopraNo ratings yet
- Craniectomia DescompresivaDocument51 pagesCraniectomia DescompresivaVlady78No ratings yet
- Journal of Trauma & Treatment: Lateral Thoracostomy Tubes: Is Outcome Affected by Level of Intercostal Space?Document3 pagesJournal of Trauma & Treatment: Lateral Thoracostomy Tubes: Is Outcome Affected by Level of Intercostal Space?Divara SyautaNo ratings yet
- Jamaneurology Jiang 2018 Oi 180048Document9 pagesJamaneurology Jiang 2018 Oi 180048jonas lopetNo ratings yet
- Long-Term Fate of The Truncal ValveDocument15 pagesLong-Term Fate of The Truncal Valvehuynhtruongthinh1998No ratings yet
- Treatment of Benign Tracheal Stenosis Using Endoluminal Spray CryotherapyDocument6 pagesTreatment of Benign Tracheal Stenosis Using Endoluminal Spray CryotherapyVania Dwi AndhaniNo ratings yet
- Sobrevida en Timomas Con Resección IncompletaDocument7 pagesSobrevida en Timomas Con Resección Incompletacarlos corrales zamoraNo ratings yet
- Nonsedation or Light Sedation in Critically IllDocument9 pagesNonsedation or Light Sedation in Critically IllPutra SetiawanNo ratings yet
- WJC 7 86Document16 pagesWJC 7 86misbahNo ratings yet
- JURNALDocument6 pagesJURNALPutu erwanNo ratings yet
- Thoracoscopic Drainage of EmpyemaDocument5 pagesThoracoscopic Drainage of EmpyemaDr Nilesh NagdeveNo ratings yet
- 2012 Article 220Document5 pages2012 Article 220Ines Riera MoyaNo ratings yet
- Comparison of The Effect of Three Treatment Interventions For The Control of Meniere 'S Disease: A Randomized Control TrialDocument6 pagesComparison of The Effect of Three Treatment Interventions For The Control of Meniere 'S Disease: A Randomized Control Trialian danarkoNo ratings yet
- 76 FullDocument12 pages76 FullRodrigo Navia ValenzuelaNo ratings yet
- Meretoja 2017Document6 pagesMeretoja 2017dvkhvbbds7No ratings yet
- 8early vs. Late Tracheostomy in Intensive Care Settings Impact On ICU and Hospital Costs 2018Document4 pages8early vs. Late Tracheostomy in Intensive Care Settings Impact On ICU and Hospital Costs 2018Cường Nguyễn HùngNo ratings yet
- JCVJS 8 44Document6 pagesJCVJS 8 44Rvo ProductionNo ratings yet
- 10 36516-Jocass 1240290-2908682Document5 pages10 36516-Jocass 1240290-2908682yyyyx842No ratings yet
- Early Use of TIPS in Cirrhosis and Variceal BleedingDocument10 pagesEarly Use of TIPS in Cirrhosis and Variceal Bleedingray liNo ratings yet
- Medscimonit 27 E931597Document7 pagesMedscimonit 27 E931597kedelai pilihanNo ratings yet
- f194 DikonversiDocument5 pagesf194 DikonversiFarizka Dwinda HNo ratings yet
- JTD 10 06 3216Document9 pagesJTD 10 06 3216madeNo ratings yet
- Impact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsDocument6 pagesImpact of Time To Surgery After Neoadjuvant Chemotherapy in Operable Breast Cancer PatientsPani lookyeeNo ratings yet
- Predictor de ExtubacionDocument10 pagesPredictor de Extubacionmomis_92No ratings yet
- Tenecteplase To Replace Alteplase Comparing ThromDocument2 pagesTenecteplase To Replace Alteplase Comparing ThromAlex DegraciaNo ratings yet
- 2019-Prolotherapy-Vs-Eswt-For-Lateral-Epicondylosis VS ONDAS DE CHOQUEDocument5 pages2019-Prolotherapy-Vs-Eswt-For-Lateral-Epicondylosis VS ONDAS DE CHOQUEDuilio GuzzardoNo ratings yet
- Pone 0190952Document14 pagesPone 0190952SangiliNo ratings yet
- Pi Is 1078588417304057Document8 pagesPi Is 1078588417304057Dede MarizalNo ratings yet
- Wu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalDocument4 pagesWu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalcharlaayasyafefiNo ratings yet
- Phlebology 2015 CatarinellaDocument6 pagesPhlebology 2015 CatarinellaAnonymous xt0nbJa2iSNo ratings yet
- DAF6 FE97 D 01Document33 pagesDAF6 FE97 D 01Lorelyn DelfinNo ratings yet
- Management of Pneumothorax in Emergency Medicine Departments: Multicenter TrialDocument6 pagesManagement of Pneumothorax in Emergency Medicine Departments: Multicenter TrialYuliana WiralestariNo ratings yet
- AJPON HNN QOL 2021Document9 pagesAJPON HNN QOL 2021wangyjNo ratings yet
- 27 10 Year Survival After Breast-Conserving Surgery Plus Radiotherapy Compared With Mastectomy in Early Breast Cancer in The Netherlands - A Population-Based StudyDocument13 pages27 10 Year Survival After Breast-Conserving Surgery Plus Radiotherapy Compared With Mastectomy in Early Breast Cancer in The Netherlands - A Population-Based StudyAnonymous 34158U5pNo ratings yet
- Case Pres PTB NewDocument32 pagesCase Pres PTB NewJuan MiguelNo ratings yet
- Effect of Endobronchial Coils Vs Usual Care On Exercise Tolerance in Patients With Severe Emphysema The RENEW Randomized Clinical TrialDocument12 pagesEffect of Endobronchial Coils Vs Usual Care On Exercise Tolerance in Patients With Severe Emphysema The RENEW Randomized Clinical TrialCésarNo ratings yet
- 2017-Earlier Versus Later Initiation of Renal Replacement Therapy Among Critically Ill Patients With Acute Kidney Injury PDFDocument14 pages2017-Earlier Versus Later Initiation of Renal Replacement Therapy Among Critically Ill Patients With Acute Kidney Injury PDFClaudioLagosNo ratings yet
- J Chest 2017 08 022Document30 pagesJ Chest 2017 08 022malvindersahiNo ratings yet
- Bonati 2015Document10 pagesBonati 2015valerioNo ratings yet
- CMJ 128 826Document9 pagesCMJ 128 826nadya magfiraNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument4 pagesAnnals of Medicine and Surgery: SciencedirectSafitryNo ratings yet
- Ojsadmin, 195Document8 pagesOjsadmin, 195ሀይደር ዶ.ርNo ratings yet
- HospitalisasiDocument13 pagesHospitalisasiViviNo ratings yet
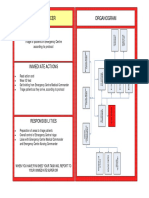
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- Health Policy and Technology: Weiwei Xu, Jing Wu, Lidan CaoDocument10 pagesHealth Policy and Technology: Weiwei Xu, Jing Wu, Lidan CaoArgonne Robert AblanqueNo ratings yet
- Sexual Harassment ComplaintDocument8 pagesSexual Harassment ComplaintJames Mulder100% (1)
- Statement On Documentation of Anesthesia CareDocument3 pagesStatement On Documentation of Anesthesia CareAzaria WNo ratings yet
- Deliverable-15 - Project ReportDocument62 pagesDeliverable-15 - Project ReportRajib Ul HaqueNo ratings yet
- Intensive Care Unit (ICU) Manual 2020-21Document146 pagesIntensive Care Unit (ICU) Manual 2020-21anithaNo ratings yet
- Nursing Interventions For Critically Ill Traumatic Brain Injury PatientsDocument7 pagesNursing Interventions For Critically Ill Traumatic Brain Injury PatientsvishwamedhiNo ratings yet
- Case Study Acute Myocardial InfarctionDocument11 pagesCase Study Acute Myocardial InfarctionChristine Elaine Batusin Ilagan91% (23)
- Level 3 Hospital Research PDF FreeDocument9 pagesLevel 3 Hospital Research PDF FreekanaNo ratings yet
- Kontrak Belajar Gadar Igd BaruDocument14 pagesKontrak Belajar Gadar Igd BaruAstridNo ratings yet
- Intensive Care UnitDocument12 pagesIntensive Care UnitAnt OnNo ratings yet
- Shree Hospital: Bidar CT Scan Bidar CT Scan Bidar CT ScanDocument8 pagesShree Hospital: Bidar CT Scan Bidar CT Scan Bidar CT ScanhattisanjayNo ratings yet
- Cost of Modern HospitalDocument9 pagesCost of Modern Hospitalrajmb16No ratings yet
- Concept of Critical CareDocument4 pagesConcept of Critical CareLohrhen Lheighh Cahreeniyow100% (6)
- 2017 Ghid PTR Rezidenti SOCCA-Residents-Guide-2017Document491 pages2017 Ghid PTR Rezidenti SOCCA-Residents-Guide-2017pasaNo ratings yet
- Nursing-Journal-Spring-2019 INNOVACIONDocument22 pagesNursing-Journal-Spring-2019 INNOVACIONMario Alberto Osorio ArlanttNo ratings yet
- New India Top-Up MediclaimDocument29 pagesNew India Top-Up MediclaimSathish ArumugamNo ratings yet
- MSI TemplateDocument3 pagesMSI TemplateKenneth LuciferNo ratings yet
- Final Case Study HospitalDocument19 pagesFinal Case Study HospitalAKASH DAYALNo ratings yet
- KarakDocument98 pagesKarakEng-Mohammed Abu NuktaNo ratings yet
- SurgeryDocument135 pagesSurgeryAndi AlfianNo ratings yet
- Generic Cover LetterDocument3 pagesGeneric Cover Letterapi-662477881No ratings yet
- Guidelines For The Design and Construction of Health Care FacilitiesDocument370 pagesGuidelines For The Design and Construction of Health Care Facilitiesmasoodae93% (15)
- Testing The Impact of Protocolized Care Of.5Document9 pagesTesting The Impact of Protocolized Care Of.5Nelson Da VegaNo ratings yet
- Resume-Lacuesta Final-1Document2 pagesResume-Lacuesta Final-1api-280661636No ratings yet
- 3 RD Year BSC NursingDocument67 pages3 RD Year BSC NursingSURAJ2792100% (1)
- American Academy of Pediatrics: ABBREVIATION. PICU, Pediatric Intensive Care UnitDocument3 pagesAmerican Academy of Pediatrics: ABBREVIATION. PICU, Pediatric Intensive Care UnitdoctorsamitNo ratings yet
- Form1 PDFDocument43 pagesForm1 PDFchrisNo ratings yet
- MGIMS Annual Report 2020-21Document213 pagesMGIMS Annual Report 2020-21Parthik ShahNo ratings yet
- Challenges and Complexities of Meeting Family.1Document2 pagesChallenges and Complexities of Meeting Family.1Tomas EvansNo ratings yet