You might also like
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A ReviewDocument6 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A ReviewDede Rahman AgustianNo ratings yet
- Stevens-Johnson SyndromeDocument4 pagesStevens-Johnson SyndromeBelleNo ratings yet
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A ReviewDocument6 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Reviewイアン リムホト ザナガNo ratings yet
- 303 1644 1 PB PDFDocument5 pages303 1644 1 PB PDFMahesa Diantari100% (1)
- Em IvDocument4 pagesEm IvathiyafrNo ratings yet
- Erythema Multiforme Major: Case Report and Review of LiteratureDocument6 pagesErythema Multiforme Major: Case Report and Review of LiteratureSasa AprilaNo ratings yet
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis - ClinicalKeyDocument21 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis - ClinicalKeyMasithaNo ratings yet
- Ijccm 25 575Document5 pagesIjccm 25 575Nandha KumarNo ratings yet
- Clinical Features, Diagnosis, and Treatment of Erythema Multiforme: A Review For The Practicing DermatologistDocument14 pagesClinical Features, Diagnosis, and Treatment of Erythema Multiforme: A Review For The Practicing DermatologistBiljana CavdarovskaNo ratings yet
- Print Jurnal 3Document7 pagesPrint Jurnal 3Amalia GrahaniNo ratings yet
- Putra,+18 Bmj.v5i1.274Document9 pagesPutra,+18 Bmj.v5i1.274noor hidayahNo ratings yet
- Jurnal KulitDocument8 pagesJurnal Kulitzak bearNo ratings yet
- Clinical Features, Diagnosis, and Treatment of Erythema Multiforme - A Review For The Practicing DermatologistDocument14 pagesClinical Features, Diagnosis, and Treatment of Erythema Multiforme - A Review For The Practicing Dermatologist2211801733No ratings yet
- Drug Induced-Stevens Johnson Syndrome: A Case ReportDocument26 pagesDrug Induced-Stevens Johnson Syndrome: A Case ReportdoktersandraNo ratings yet
- Acute Primary Herpetic Gingivostomatitis: Ravi Prakash Sasankoti Mohan, Sankalp Verma, Udita Singh, Neha AgarwalDocument3 pagesAcute Primary Herpetic Gingivostomatitis: Ravi Prakash Sasankoti Mohan, Sankalp Verma, Udita Singh, Neha AgarwalBrili AnenoNo ratings yet
- "Drug Induced Erythema Multiforme" - A ReviewDocument7 pages"Drug Induced Erythema Multiforme" - A ReviewNauroh NaurohNo ratings yet
- Successful Treatment of Herpes Simplex-Associated Erythema Multiforme With A Combination of Acyclovir and PrednisoneDocument3 pagesSuccessful Treatment of Herpes Simplex-Associated Erythema Multiforme With A Combination of Acyclovir and PrednisoneannisafebriezaNo ratings yet
- Bieber, T.Document7 pagesBieber, T.Anak Agung Ayu Ira Kharisma Buana Undiksha 2019No ratings yet
- Pharmacological Management of Common Soft Tissue Lesions of The Oral CavityDocument16 pagesPharmacological Management of Common Soft Tissue Lesions of The Oral CavityAcisum2No ratings yet
- Chronic Recurrent Multifocal Osteomyelitis of The Mandible: Report of Three CasesDocument12 pagesChronic Recurrent Multifocal Osteomyelitis of The Mandible: Report of Three CasesandrikaNo ratings yet
- Case Report 2 PDFDocument5 pagesCase Report 2 PDFSittiNurQomariahNo ratings yet
- Stevens-Johnson Syndrome and Abuse of Anabolic SteroidsDocument4 pagesStevens-Johnson Syndrome and Abuse of Anabolic SteroidsRafael SebastianNo ratings yet
- Nicotine-Induced Bullous Fixed Drug EruptionDocument3 pagesNicotine-Induced Bullous Fixed Drug Eruptionamal amanahNo ratings yet
- Paracetamol Induced Steven-Johnson Syndrome A Rare Case ReportDocument4 pagesParacetamol Induced Steven-Johnson Syndrome A Rare Case ReporthadiatussalamahNo ratings yet
- HFMD Immunocompeten AdultDocument3 pagesHFMD Immunocompeten AdultdantiNo ratings yet
- Case Study On Pemphigus VulgarisDocument2 pagesCase Study On Pemphigus VulgarisRanindya PutriNo ratings yet
- 571 FullDocument2 pages571 FullJauhari JoNo ratings yet
- Case Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseDocument4 pagesCase Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseYeni PuspitasariNo ratings yet
- Drug-Mediated Rash: Erythema Multiforme Versus Stevens-Johnson SyndromeDocument4 pagesDrug-Mediated Rash: Erythema Multiforme Versus Stevens-Johnson SyndromeMădălina ŞerbanNo ratings yet
- 8 Bains A (49-52) PDFDocument4 pages8 Bains A (49-52) PDFWa JulianiNo ratings yet
- 7692-Article Text-30295-3-10-20200319 PDFDocument4 pages7692-Article Text-30295-3-10-20200319 PDFHata BotonjicNo ratings yet
- Pemphigus Vulgaris 1Document3 pagesPemphigus Vulgaris 1Yeni PuspitasariNo ratings yet
- Primary Conjunctival Tuberculosis-2Document3 pagesPrimary Conjunctival Tuberculosis-2puutieNo ratings yet
- PDM Os4Document3 pagesPDM Os4Erdinawira RizkianiNo ratings yet
- Stevens Johnson SyndromeDocument9 pagesStevens Johnson SyndromeMrslidyaNo ratings yet
- Chronic Recurrent Multifocal Osteomyelitis of The Mandible: Report of Three CasesDocument12 pagesChronic Recurrent Multifocal Osteomyelitis of The Mandible: Report of Three CasesandrikaNo ratings yet
- Erythema MultiformeDocument16 pagesErythema MultiformeGuen ColisNo ratings yet
- Recent Updates in the Treatment of Erythema MultiformeDocument8 pagesRecent Updates in the Treatment of Erythema MultiformeimantikachristinaaaNo ratings yet
- SJSInJPharPract 12 2 133 PDFDocument3 pagesSJSInJPharPract 12 2 133 PDFRidho Nugroho Wahyu AkbarNo ratings yet
- Herpetic) : Titis Virus13Document10 pagesHerpetic) : Titis Virus13John Michael VicenteNo ratings yet
- ClinRevSJsyndrome PDFDocument5 pagesClinRevSJsyndrome PDFMuhammad Nur Ardhi LahabuNo ratings yet
- Erythema Multiforme: A Case Series and Review of Literature: November 2018Document8 pagesErythema Multiforme: A Case Series and Review of Literature: November 2018Nurlina NurdinNo ratings yet
- PV 1Document4 pagesPV 1Aing ScribdNo ratings yet
- Erythema Multiforme-Oral Variant: Case Report and Review of LiteratureDocument4 pagesErythema Multiforme-Oral Variant: Case Report and Review of LiteratureMarniati JohanNo ratings yet
- BullousDocument3 pagesBullousLjubomirErdoglijaNo ratings yet
- Tugas BacaDocument20 pagesTugas BacaAyu WulansariNo ratings yet
- Autoinflammatory Syndromes Associated With Hidradenitis Suppurativa and or AcneDocument8 pagesAutoinflammatory Syndromes Associated With Hidradenitis Suppurativa and or AcneFreddy RojasNo ratings yet
- Mockenhaupt Eemm Sjs TenDocument6 pagesMockenhaupt Eemm Sjs TengratianusbNo ratings yet
- Recurrent Erythema Multiforme: A Dental Case Report: ReviewDocument4 pagesRecurrent Erythema Multiforme: A Dental Case Report: Reviewjenn_1228No ratings yet
- Epidermodysplasia Verruciformis Tree Man Syndrome A Brief Review With Case Reports 177Document3 pagesEpidermodysplasia Verruciformis Tree Man Syndrome A Brief Review With Case Reports 177Medtext PublicationsNo ratings yet
- Herpes Zoster: A Case ReportDocument3 pagesHerpes Zoster: A Case ReportAhmad HaikalNo ratings yet
- Jawt 11 I 2 P 48Document3 pagesJawt 11 I 2 P 48Irma NoviantiNo ratings yet
- Journal Rosacea Report Lain PDFDocument5 pagesJournal Rosacea Report Lain PDFtesaNo ratings yet
- Pi Is 0190962214011566Document2 pagesPi Is 0190962214011566LewishoppusNo ratings yet
- Cheilitis Granulomatosa of Melkersson-Rosenthal Syndrome: Treatment With Intralesional Corticosteroid InjectionsDocument3 pagesCheilitis Granulomatosa of Melkersson-Rosenthal Syndrome: Treatment With Intralesional Corticosteroid InjectionsTatiana OrdoñezNo ratings yet
- 2 em 1Document1 page2 em 1Érica MarianoNo ratings yet
- Herpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseDocument5 pagesHerpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseClodeyaRizolaNo ratings yet
- Rash and Fever After Sulfasalazine UseDocument5 pagesRash and Fever After Sulfasalazine UseChistian LassoNo ratings yet
- Obstetrics 4 1084Document2 pagesObstetrics 4 1084Irma NoviantiNo ratings yet
- Toxic Epidermal Necrolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandToxic Epidermal Necrolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 1a - 607 Acc - Research Article - LNDocument5 pages1a - 607 Acc - Research Article - LNromyNo ratings yet
- Neurofibromatosis Type 2: Review ArticlesDocument9 pagesNeurofibromatosis Type 2: Review ArticlesPaviliuc RalucaNo ratings yet
- Oral Manifestations of Gardner's Syndrome in Young Patients: Report of Three CasesDocument5 pagesOral Manifestations of Gardner's Syndrome in Young Patients: Report of Three Casesromy100% (1)
- 4 Determinants of Family Independence in Caring For Hebephrenic Schizophrenia Patients-MinDocument9 pages4 Determinants of Family Independence in Caring For Hebephrenic Schizophrenia Patients-MinromyNo ratings yet
- Cirrhotic Ascites: A Review of Pathophysiology and ManagementDocument10 pagesCirrhotic Ascites: A Review of Pathophysiology and ManagementromyNo ratings yet
- 1608 04192 PDFDocument13 pages1608 04192 PDFromyNo ratings yet
- Neurofibromatosis Type 1: ClinicalpictureDocument1 pageNeurofibromatosis Type 1: ClinicalpictureromyNo ratings yet
- BPJ Vol 11 No 1 P 167-170Document4 pagesBPJ Vol 11 No 1 P 167-170indrayaniNo ratings yet
- Hepatic Encephalopathy: Peter FerenciDocument10 pagesHepatic Encephalopathy: Peter FerenciromyNo ratings yet
- PIIS0953620519303413Document7 pagesPIIS0953620519303413romyNo ratings yet
- Pharmaceuticals: Critical Overview On The Benefits and Harms of AspirinDocument16 pagesPharmaceuticals: Critical Overview On The Benefits and Harms of AspirinromyNo ratings yet
- Imj 13735Document6 pagesImj 13735romyNo ratings yet
- Dentistry: Gardener Syndrome: A Rare Case ReportDocument3 pagesDentistry: Gardener Syndrome: A Rare Case ReportromyNo ratings yet
- v09p0137 PDFDocument5 pagesv09p0137 PDFromyNo ratings yet
- Walking Is More Efficient Than Thought For Threatened Polar BearsDocument1 pageWalking Is More Efficient Than Thought For Threatened Polar BearsromyNo ratings yet
- Gingivitis A Silent Disease PDFDocument4 pagesGingivitis A Silent Disease PDFPragita Ayu SaputriNo ratings yet
- The Diagnosis and Management of Atypical Types of Diabetes: Kathryn Evans Kreider, DNP, FNP-BCDocument7 pagesThe Diagnosis and Management of Atypical Types of Diabetes: Kathryn Evans Kreider, DNP, FNP-BCromyNo ratings yet
- Bird predation by praying mantisesDocument14 pagesBird predation by praying mantisesromyNo ratings yet
- Fulminant Hepatitis: Definitions, Causes and Management: Vincenzo Morabito, Danielle AdebayoDocument11 pagesFulminant Hepatitis: Definitions, Causes and Management: Vincenzo Morabito, Danielle AdebayoIvan Yoseph SaputraNo ratings yet
- Concise Clinical Review: Anthrax InfectionDocument9 pagesConcise Clinical Review: Anthrax Infectionaulia rahadianNo ratings yet
- QUT Digital Repository: 29984Document15 pagesQUT Digital Repository: 29984romyNo ratings yet
- 2017-Colibri MAVDocument14 pages2017-Colibri MAVromyNo ratings yet
- Why and How We Are Not ZombiesDocument4 pagesWhy and How We Are Not ZombiesromyNo ratings yet
- Anticipating The Zombie Apocalypse Using ImprobabiDocument13 pagesAnticipating The Zombie Apocalypse Using ImprobabiromyNo ratings yet
- Zombie PublicationDocument20 pagesZombie PublicationJordan MoshcovitisNo ratings yet
- Seizures in COVID 19Document2 pagesSeizures in COVID 19romyNo ratings yet
- The Magical Power of Blood: The Curse of The Vampire From An Anthropological Point of WievDocument35 pagesThe Magical Power of Blood: The Curse of The Vampire From An Anthropological Point of WievromyNo ratings yet
- COVID19-and-Epilepsy FAQ 040920 v3Document4 pagesCOVID19-and-Epilepsy FAQ 040920 v3romyNo ratings yet
- Integrated Pest Management of The German Cockroach (Blattodea: Blattellidae) in Manufactured Homes in Rural North CarolinaDocument7 pagesIntegrated Pest Management of The German Cockroach (Blattodea: Blattellidae) in Manufactured Homes in Rural North CarolinaromyNo ratings yet
- Internal Medicine (I) Log Book Black Color TypingDocument48 pagesInternal Medicine (I) Log Book Black Color TypingQasim HaleimiNo ratings yet
- Megaloblastic Anemia PPTDocument2 pagesMegaloblastic Anemia PPTmoncalshareen3No ratings yet
- Aspek Medis Bedah (Perioperatif) Dan Enteral - Parenteral NutrisiDocument56 pagesAspek Medis Bedah (Perioperatif) Dan Enteral - Parenteral NutrisiJashmine RachlyNo ratings yet
- Week 7. Renal Pathology Continued.Document9 pagesWeek 7. Renal Pathology Continued.Amber LeJeuneNo ratings yet
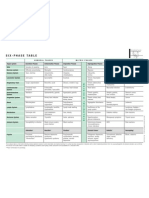
- Six-Phase Table: International Society of HomotoxicologyDocument1 pageSix-Phase Table: International Society of HomotoxicologyPablo Matas SoriaNo ratings yet
- Drug Study (Loxapine, Haloperidol)Document5 pagesDrug Study (Loxapine, Haloperidol)kuro hanabusa100% (2)
- 4 6030444038488853198 PDFDocument110 pages4 6030444038488853198 PDFSyeda Seri RazaNo ratings yet
- Gestational Choriocarcinoma OranuDocument8 pagesGestational Choriocarcinoma Oranuapi-3705046No ratings yet
- Recognition and Interpretation of Skin 1Document6 pagesRecognition and Interpretation of Skin 1Veterinarios de ArgentinaNo ratings yet
- SSM-11th Edn Full IndexDocument62 pagesSSM-11th Edn Full Indexece142No ratings yet
- Controlling asthma with AlbuterolDocument2 pagesControlling asthma with AlbuterolVinz Khyl G. CastillonNo ratings yet
- Koding Icd 10 & Icd 9 NewwDocument30 pagesKoding Icd 10 & Icd 9 NewwJar Jar79% (14)
- Musculoskeletal RadiologyDocument5 pagesMusculoskeletal Radiologyapi-3743483No ratings yet
- Pocket Book of Hospital Care For Children - Guidleines For The Management of Common Illnesses With Limited Resources. (2012, World Health Organization)Document442 pagesPocket Book of Hospital Care For Children - Guidleines For The Management of Common Illnesses With Limited Resources. (2012, World Health Organization)Sadia YousafNo ratings yet
- Eyelid Disorders Guide: Ptosis, Blepharitis, Hordeolum & MoreDocument48 pagesEyelid Disorders Guide: Ptosis, Blepharitis, Hordeolum & MoreUdaif BabuNo ratings yet
- Drug StudyDocument3 pagesDrug StudySoniaMarieBalanayNo ratings yet
- Fitzpatricks Dermatology 9th Edition 3123Document1 pageFitzpatricks Dermatology 9th Edition 3123DennisSujayaNo ratings yet
- Ileus Obstruksi - Anggi Eka ForendaDocument12 pagesIleus Obstruksi - Anggi Eka ForendaNadya ZahraNo ratings yet
- Biomo306 Quiz One QuestionsDocument5 pagesBiomo306 Quiz One QuestionsAdrianNo ratings yet
- BOTOXDocument12 pagesBOTOXJanani KrishnanNo ratings yet
- Drugs Acting On The AnsDocument57 pagesDrugs Acting On The AnsAnonymous iG0DCOfNo ratings yet
- Treatment For Subdural HygromaDocument3 pagesTreatment For Subdural HygromaEka NataNo ratings yet
- Fish Diseases (Jorge C. Eiras, Helmut Segner, Thomas Wahli Etc.) (Z-Library)Document1,327 pagesFish Diseases (Jorge C. Eiras, Helmut Segner, Thomas Wahli Etc.) (Z-Library)Iryna ZapekaNo ratings yet
- Red Man SyndromeDocument3 pagesRed Man Syndrome林唐宇No ratings yet
- PTH 725 - Multiple-Sclerosis-Case StudyDocument19 pagesPTH 725 - Multiple-Sclerosis-Case StudyEnrique Guillen InfanteNo ratings yet
- Q&A Pharmacology 2Document19 pagesQ&A Pharmacology 2api-3818438No ratings yet
- Common Lab Tests & Their Use in Diagnosis & Treatment PDFDocument17 pagesCommon Lab Tests & Their Use in Diagnosis & Treatment PDFChAwaisNo ratings yet
- Jurnal Amalgam TatoDocument2 pagesJurnal Amalgam TatoLu'luatul WidadNo ratings yet
- Curs VII - Terapii SistemiceDocument229 pagesCurs VII - Terapii SistemiceHucay EduardNo ratings yet
- 2 PDFDocument297 pages2 PDFTaj KoyyodeNo ratings yet