You might also like
- Quiz Anatomy Part 3 of 3Document56 pagesQuiz Anatomy Part 3 of 3MedShare75% (4)
- Mineire'sDocument16 pagesMineire'sShaykh Evangelista BacualNo ratings yet
- Hearing LossDocument31 pagesHearing LossDat boi100% (1)
- B 22-Rs-Anatomy - Saq AnswersDocument22 pagesB 22-Rs-Anatomy - Saq Answersapi-516879364No ratings yet
- Osce Notes in OtolaryngologyDocument94 pagesOsce Notes in OtolaryngologyDr. T. Balasubramanian92% (39)
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Neurological ExaminationDocument73 pagesNeurological Examinationkhorrami4No ratings yet
- Absite January2014 ReviewDocument1,226 pagesAbsite January2014 ReviewAnnTran100% (12)
- FULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF Ebookjennifer.lawver532100% (42)
- Neurogenic Disorders of The LarynxDocument37 pagesNeurogenic Disorders of The LarynxSyaffira SalsabilaNo ratings yet
- Skull ProjectionsDocument66 pagesSkull Projectionsron reteracionNo ratings yet
- Deafness: Lahore College For Women UniversityDocument25 pagesDeafness: Lahore College For Women Universityjames_sk8734No ratings yet
- DLP in Science 3 - 4 Q2 WK 1 ValidatedDocument14 pagesDLP in Science 3 - 4 Q2 WK 1 ValidatedSalve Serrano100% (4)
- 18sleep Apnea and Sleep DisordersDocument23 pages18sleep Apnea and Sleep Disordersnikita ester100% (1)
- Dysphonia: The Voice of Change: Phonation 63Document3 pagesDysphonia: The Voice of Change: Phonation 63Ali Arridha MolahellaNo ratings yet
- Inflammatory Infection and Trauma of The Middle EarDocument27 pagesInflammatory Infection and Trauma of The Middle EarChristelle Ann FarralesNo ratings yet
- Bab 91Document10 pagesBab 91Syaffira SalsabilaNo ratings yet
- Hearing Impairment in Older People: A Review: Lisa Fook, Rosemary MorganDocument5 pagesHearing Impairment in Older People: A Review: Lisa Fook, Rosemary MorganMANGKAGENo ratings yet
- Sensorineural Hearing LossDocument19 pagesSensorineural Hearing LossBenitaNo ratings yet
- Snoring - Harmful Effects: S Ramnathan Iyer, Revati R IyerDocument4 pagesSnoring - Harmful Effects: S Ramnathan Iyer, Revati R IyerDefitaria PermatasariNo ratings yet
- Muscle TensionDocument6 pagesMuscle TensionFabián Basaes OlmosNo ratings yet
- Hearing Loss SMT IV44Document94 pagesHearing Loss SMT IV44abdul fattah mufidNo ratings yet
- Presbycusis: Dr. George Backleh Dept. of Otolaryngology/ Head and Neck Surgery Hadassah University Hospital JerusalemDocument16 pagesPresbycusis: Dr. George Backleh Dept. of Otolaryngology/ Head and Neck Surgery Hadassah University Hospital Jerusalemrezky_oktarianti_syahputriNo ratings yet
- Prevention and Rehabilitation of Old Age DeafnessDocument8 pagesPrevention and Rehabilitation of Old Age DeafnessXilena HerreraNo ratings yet
- Northwestern Medicine Benign Vocal Lesions PDFDocument5 pagesNorthwestern Medicine Benign Vocal Lesions PDFHata MujadzicNo ratings yet
- CH 39Document13 pagesCH 39KoasNo ratings yet
- Ha - Asssessing EarsDocument6 pagesHa - Asssessing EarsKenneth Andre Batuyog TecsonNo ratings yet
- GOTB - Group 7 - Geriatric WorldDocument3 pagesGOTB - Group 7 - Geriatric WorldReza Afif FebriansyahNo ratings yet
- Group 3 Darlene Joyce A. Maitum Jocelyn Caleza Nathasia Raganas Coleen CabahugDocument37 pagesGroup 3 Darlene Joyce A. Maitum Jocelyn Caleza Nathasia Raganas Coleen CabahugJocelyn CalezaNo ratings yet
- Presbycusis: J. R. Kearns, MDDocument5 pagesPresbycusis: J. R. Kearns, MDnick_mdNo ratings yet
- Obstructive Sleep Apnea: Arief Fakhrizal Supervisor: Dr. Dr. Sinta Sari Ratunanda, M. Kes., Sp. T.H.T.K.L. (K)Document61 pagesObstructive Sleep Apnea: Arief Fakhrizal Supervisor: Dr. Dr. Sinta Sari Ratunanda, M. Kes., Sp. T.H.T.K.L. (K)Arief FakhrizalNo ratings yet
- Aging Voice Presbyphocia - MARTINS ET AL 2013Document5 pagesAging Voice Presbyphocia - MARTINS ET AL 2013FonoaudiologiaNo ratings yet
- Upper Airway DisordersDocument25 pagesUpper Airway DisordersIliana EsquivelNo ratings yet
- Meniere's DiseaseDocument16 pagesMeniere's DiseaseKarina BundaNo ratings yet
- CH 291 Sleep ApneaDocument4 pagesCH 291 Sleep ApneaGwen Marielle CursoNo ratings yet
- MS Continuation ofDocument13 pagesMS Continuation ofAngelica Joan SorianoNo ratings yet
- Nikolaus Ronald Indra 4Document137 pagesNikolaus Ronald Indra 4Florence StellaNo ratings yet
- Presbycusis: Sang Hoon Kim, Seung Geun YeoDocument6 pagesPresbycusis: Sang Hoon Kim, Seung Geun YeoLuluk AisyahNo ratings yet
- Clinicopathological Study of Change of Voice: ST THDocument10 pagesClinicopathological Study of Change of Voice: ST THAshokNo ratings yet
- What Is Presbycusis?: OtosclerosisDocument8 pagesWhat Is Presbycusis?: OtosclerosisIndraRukmanaHamimPartIINo ratings yet
- Unit 1 Disorders of Upper Gastrointestinal Tract: StructureDocument18 pagesUnit 1 Disorders of Upper Gastrointestinal Tract: StructureShubhendu ChattopadhyayNo ratings yet
- Obstructive Sleep Apnea: An Overview On Features, Diagnosis & Orthodontic ManagementDocument6 pagesObstructive Sleep Apnea: An Overview On Features, Diagnosis & Orthodontic Managementsajida khanNo ratings yet
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- DD PresbikusisDocument3 pagesDD PresbikusisJ KrystalNo ratings yet
- Kung 2007Document10 pagesKung 2007Sarah fadlainiNo ratings yet
- Drtbalu'S Otolaryngology Online: PresbyacusisDocument3 pagesDrtbalu'S Otolaryngology Online: PresbyacusisAnish RajNo ratings yet
- 12 P69344 Pho Kapitel 4 S47 52 PDFDocument6 pages12 P69344 Pho Kapitel 4 S47 52 PDFprofesor conanNo ratings yet
- Hearing Impairment 1 (Document)Document10 pagesHearing Impairment 1 (Document)Jocelyn CalezaNo ratings yet
- A. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthDocument6 pagesA. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthRubi MeeajanNo ratings yet
- Pemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanDocument71 pagesPemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanRilianda SimbolonNo ratings yet
- Adult and Pediatric Obstructive Sleep ApneaDocument44 pagesAdult and Pediatric Obstructive Sleep ApneaSwastik SatpathyNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Bedside Water Swallow Test ArticleDocument4 pagesBedside Water Swallow Test ArticleJU WSDNo ratings yet
- Presbycusis JagadDocument34 pagesPresbycusis Jagadraja gurusingaNo ratings yet
- Asymmetrical Hearing Loss: Jessica PrasadDocument6 pagesAsymmetrical Hearing Loss: Jessica PrasadSujaya ChattopadhyayNo ratings yet
- 2.3 Voice - Disorders2Document20 pages2.3 Voice - Disorders2Fernanda MerichesNo ratings yet
- 114 Barera CsDocument15 pages114 Barera Cskaloydiaz09No ratings yet
- Meniere's DiseaseDocument50 pagesMeniere's DiseaseRaisa CleizeraNo ratings yet
- AFP Clinical Nasal ObstructionDocument5 pagesAFP Clinical Nasal ObstructionTri OktarinaNo ratings yet
- Physiology of Swallowing: Table 1Document6 pagesPhysiology of Swallowing: Table 1Nelly ElizabethNo ratings yet
- Manejo Dental ELADocument4 pagesManejo Dental ELAAline LoyolaNo ratings yet
- What Is PresbycusisDocument4 pagesWhat Is PresbycusisNisa UcilNo ratings yet
- 4 Walton2018Document6 pages4 Walton2018meeNo ratings yet
- The Relationship Between Lesion Localization and Swallowing DisordersDocument7 pagesThe Relationship Between Lesion Localization and Swallowing DisordersMala MirnaNo ratings yet
- Tinnitus: Causes and Clinical Management: ReviewDocument11 pagesTinnitus: Causes and Clinical Management: ReviewFebrina Listya AndantiNo ratings yet
- Hyperfunctional Voice DisordersDocument11 pagesHyperfunctional Voice DisordersJam PNo ratings yet
- Hoarseness: What Is The Voice Trying To Tell You?Document5 pagesHoarseness: What Is The Voice Trying To Tell You?lancealiuNo ratings yet
- Parkinsons Disease and Hearing LossDocument8 pagesParkinsons Disease and Hearing LossJohn OmandacNo ratings yet
- Extracellular Fluid VolumeDocument4 pagesExtracellular Fluid VolumeMary Dominique RomoNo ratings yet
- Anatomy and Physiology of The Nose and ParanasalDocument35 pagesAnatomy and Physiology of The Nose and ParanasalMary Dominique RomoNo ratings yet
- Trauma-Induced Coagulopathy: An Institution's 35 Year Perspective On Practice and ResearchDocument16 pagesTrauma-Induced Coagulopathy: An Institution's 35 Year Perspective On Practice and ResearchMary Dominique RomoNo ratings yet
- Script Patho Tubal PregnancyDocument10 pagesScript Patho Tubal PregnancyMary Dominique RomoNo ratings yet
- Chapter 16 SummaryDocument3 pagesChapter 16 SummaryMary Dominique RomoNo ratings yet
- Medical Infographics by SlidesgoDocument32 pagesMedical Infographics by SlidesgoMary Dominique RomoNo ratings yet
- Bullous-2018 TPDocument136 pagesBullous-2018 TPMary Dominique RomoNo ratings yet
- 2019 Acne Rosacea - Edit TPDocument114 pages2019 Acne Rosacea - Edit TPMary Dominique RomoNo ratings yet
- Community CensusDocument2 pagesCommunity CensusMary Dominique RomoNo ratings yet
- AKI Case Discussion 2.0Document3 pagesAKI Case Discussion 2.0Mary Dominique RomoNo ratings yet
- Hi CrushDocument1 pageHi CrushMary Dominique RomoNo ratings yet
- DYSMENORRHEA Hammer PDFDocument8 pagesDYSMENORRHEA Hammer PDFMary Dominique Romo100% (1)
- Anatomi Tulang Tengkorak Manusia: Pembimbing: Dr. Fadil, SP - BSDocument28 pagesAnatomi Tulang Tengkorak Manusia: Pembimbing: Dr. Fadil, SP - BSichacloudiacNo ratings yet
- Congenital HypothyroidismDocument18 pagesCongenital Hypothyroidismcalamyl295No ratings yet
- Teeth, Vessels and Nerves of Oral CavityDocument86 pagesTeeth, Vessels and Nerves of Oral Cavityk20221163No ratings yet
- 03 Lecture DPT 4 Neuroanatomy 'FUNCTION OF CEREBRAL HEMISPHERE' 'Part A'Document48 pages03 Lecture DPT 4 Neuroanatomy 'FUNCTION OF CEREBRAL HEMISPHERE' 'Part A'Farhan HaleemNo ratings yet
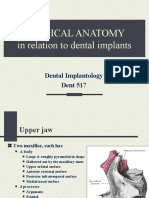
- Anatomy in Dental ImplantologyDocument29 pagesAnatomy in Dental ImplantologyZiad RabieNo ratings yet
- 3800lecture 1 - Eye AnatomyDocument17 pages3800lecture 1 - Eye AnatomyAkshay Dhawan100% (1)
- Tuning Fork Tests: Name: Roll No: Assignment: Submitted ToDocument3 pagesTuning Fork Tests: Name: Roll No: Assignment: Submitted ToFizza AliNo ratings yet
- Endotracheal Intubation: Conny Noor Afifa 12100117108 Kelompok 12Document35 pagesEndotracheal Intubation: Conny Noor Afifa 12100117108 Kelompok 12Conny Noor AfifaNo ratings yet
- 3 Nose - Paranasal Sinus (More Modified)Document28 pages3 Nose - Paranasal Sinus (More Modified)adham bani younesNo ratings yet
- 1 PBDocument8 pages1 PBMahathir Harry PermanaNo ratings yet
- Case Report: Intracranial Multiple Germ Cell Tumors: A Case Report and Review of LiteratureDocument6 pagesCase Report: Intracranial Multiple Germ Cell Tumors: A Case Report and Review of Literaturearcobaleno589No ratings yet
- Module 1 2 in Oae 113 Human Anatomy PhysiologyDocument13 pagesModule 1 2 in Oae 113 Human Anatomy PhysiologyJack ElchaNo ratings yet
- Neurological Health AssessmentDocument55 pagesNeurological Health Assessment09-bays-rhythmsNo ratings yet
- Pemeriksaan Fisik THTDocument83 pagesPemeriksaan Fisik THTClara ReginaNo ratings yet
- Case RP 1 Pleomorphic AdenomaDocument5 pagesCase RP 1 Pleomorphic AdenomaSathvika BNo ratings yet
- Approach To Pediatric Neurology - BasicDocument16 pagesApproach To Pediatric Neurology - BasicAseel AyNo ratings yet
- ANP1106 ASyllabus 2020Document5 pagesANP1106 ASyllabus 2020유우솔No ratings yet
- Chapter 2 Development of The Brain 2014 Clinical NeuroscienceDocument8 pagesChapter 2 Development of The Brain 2014 Clinical NeuroscienceMarta Casals CollNo ratings yet
- (English) The Nervous System, Part 1 - Crash Course A&P #8 (DownSub - Com)Document8 pages(English) The Nervous System, Part 1 - Crash Course A&P #8 (DownSub - Com)bank townNo ratings yet
- Dr. Kunta Setiaji (ThyroidNodule)Document17 pagesDr. Kunta Setiaji (ThyroidNodule)Hasty WahyuniNo ratings yet
- BRAINSTEM II Clinical CorrelatesDocument6 pagesBRAINSTEM II Clinical CorrelatesrizaNo ratings yet
- Pacheco Et Al Phyllotis Pearsoni TH 2014Document28 pagesPacheco Et Al Phyllotis Pearsoni TH 2014Dennisse RuelasNo ratings yet
- Medicine - Special Otorhinolarynologic - Slide11Document2 pagesMedicine - Special Otorhinolarynologic - Slide11testNo ratings yet