You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- '05 Sullivan B.Document36 pages'05 Sullivan B.Geo Navarro100% (1)
- Healing The Broken HeartDocument260 pagesHealing The Broken HeartSean Lee100% (1)
- Management of Acute Pancreatitis - UpToDateDocument28 pagesManagement of Acute Pancreatitis - UpToDateJulieth QuinteroNo ratings yet
- J Gastro 2020 10 044Document20 pagesJ Gastro 2020 10 044Julieth QuinteroNo ratings yet
- Ear, Nose, ThroatDocument15 pagesEar, Nose, ThroatJulieth QuinteroNo ratings yet
- Lactated Ringer Solution Is Superior To Normal Saline Solution in Managing Acute PancreatitisDocument7 pagesLactated Ringer Solution Is Superior To Normal Saline Solution in Managing Acute PancreatitisJulieth QuinteroNo ratings yet
- Acute Colonic Diverticulitis - Medical Management - UpToDateDocument30 pagesAcute Colonic Diverticulitis - Medical Management - UpToDateJulieth QuinteroNo ratings yet
- Pain Management and Unani MedicineDocument1 pagePain Management and Unani MedicineMSKCNo ratings yet
- NP1 Nursing Board Exam December 2006 Answer Key OKDocument13 pagesNP1 Nursing Board Exam December 2006 Answer Key OKSam ParkNo ratings yet
- Sesamoidectomy For Hallux Sesamoid FracturesDocument3 pagesSesamoidectomy For Hallux Sesamoid FracturesPublicPublicationsNo ratings yet
- Guidance Ergonomics enDocument28 pagesGuidance Ergonomics enpavilamNo ratings yet
- Edukasi NyeriDocument52 pagesEdukasi NyeriEko Dakholal FirdausNo ratings yet
- Pain Management in LaborDocument33 pagesPain Management in LaborSmriti Thapa100% (1)
- Basic Ericksonian Hypnosis Ebook PDFDocument155 pagesBasic Ericksonian Hypnosis Ebook PDFFelipe Osorio100% (4)
- Trigeminal Autonomic CephalgiasDocument15 pagesTrigeminal Autonomic Cephalgiasheni taridaNo ratings yet
- Earthing - Chronic InflammationDocument13 pagesEarthing - Chronic Inflammationsamui11No ratings yet
- Scientific Basis Magnet TherapyDocument4 pagesScientific Basis Magnet TherapySuganya BalachandranNo ratings yet
- Podiatry Res ManualDocument180 pagesPodiatry Res ManualJacob Dougherty50% (2)
- Cryotherapy SRS PDFDocument20 pagesCryotherapy SRS PDFSreeraj S RNo ratings yet
- Induction of General Anesthesia - OverviewDocument40 pagesInduction of General Anesthesia - Overviewmayteveronica1000No ratings yet
- Mulligan PDFDocument6 pagesMulligan PDFAlexandru IordacheNo ratings yet
- NCPDocument14 pagesNCPRaidis Pangilinan0% (1)
- Instructions To NAET Patient Before Beginning TreatmentDocument8 pagesInstructions To NAET Patient Before Beginning TreatmentRicard Revuelto Orengo100% (1)
- Homeopathy For The Home Prescriber by Melissa KupschDocument17 pagesHomeopathy For The Home Prescriber by Melissa KupschCaroline D.No ratings yet
- Adult Cancer Pain, Version 3.2019: NCCN Clinical Practice Guidelines in OncologyDocument31 pagesAdult Cancer Pain, Version 3.2019: NCCN Clinical Practice Guidelines in Oncologyhusni gunawanNo ratings yet
- (PPT11/12-Ib-1.1) : Difference Between Holistic Thinking and Partial ThinkingDocument3 pages(PPT11/12-Ib-1.1) : Difference Between Holistic Thinking and Partial ThinkingMenjie AntiportaNo ratings yet
- Pain and Pain Gate Control MechanismDocument17 pagesPain and Pain Gate Control MechanismKapil LakhwaraNo ratings yet
- The Relief of Various Pain Symptoms Via Faradarmani: SciencedirectDocument4 pagesThe Relief of Various Pain Symptoms Via Faradarmani: SciencedirectPandaNo ratings yet
- Lester, P. Gaynor, J. S. Management of Cancer Pain. Veterinary Clinics of North America Small Animal Practice, v.30, n.4, p.951-966. 2000 PDFDocument16 pagesLester, P. Gaynor, J. S. Management of Cancer Pain. Veterinary Clinics of North America Small Animal Practice, v.30, n.4, p.951-966. 2000 PDFFran WermannNo ratings yet
- 4832 Concept Map Bri Lytle OriginalDocument6 pages4832 Concept Map Bri Lytle Originalapi-602756847No ratings yet
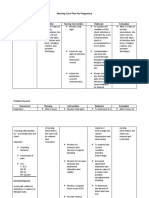
- Nursing Care Plan For Pregnancy: Risk Diagnosis Nursing Diagnosis Objective Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan For Pregnancy: Risk Diagnosis Nursing Diagnosis Objective Nursing Intervention Rationale EvaluationCheska PalomaNo ratings yet
- Annotated Bibliography NR 501Document6 pagesAnnotated Bibliography NR 501writer topNo ratings yet
- Anesthesia PlainDocument39 pagesAnesthesia PlainMIKAELA DAVIDNo ratings yet
- Pathology For The Physical Therapist Assistant 1st Edition Lescher Test BankDocument14 pagesPathology For The Physical Therapist Assistant 1st Edition Lescher Test Bankturnmiddayu0ppsx100% (29)