You might also like
- G2 BTLED Acceptability of Vacuum Fried Squash Cucurbita Maxima Chips With Different Flavors. FinalDocument28 pagesG2 BTLED Acceptability of Vacuum Fried Squash Cucurbita Maxima Chips With Different Flavors. FinalMyka Mae Edep LasernaNo ratings yet
- Jonathan Edwards TrainingDocument8 pagesJonathan Edwards TrainingMark100% (1)
- Chapter 14 Neurodevelopmental DisordersDocument13 pagesChapter 14 Neurodevelopmental DisordersAra Grace Monsanto100% (1)
- English 9-Quarter 4-Week 3Document8 pagesEnglish 9-Quarter 4-Week 3Cleo PabloNo ratings yet
- Situation Analysis of Children in The PhilippinesDocument6 pagesSituation Analysis of Children in The PhilippinesShe NnaNo ratings yet
- Adult OrthodonticsDocument70 pagesAdult OrthodonticsTruppti SononeNo ratings yet
- Artrosis Glenohumeral Despues de Artroscopia Bankart Repair A Long-Term Follow-Up of 13 YearsDocument6 pagesArtrosis Glenohumeral Despues de Artroscopia Bankart Repair A Long-Term Follow-Up of 13 Yearsmarcelogascon.oNo ratings yet
- Open Reduction and Internal Fixation ORIF of ComplDocument6 pagesOpen Reduction and Internal Fixation ORIF of ComplAnnisa AnggrainiNo ratings yet
- Surgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009Document6 pagesSurgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009agus sukarnaNo ratings yet
- 53 - Changes in Arthroscopic Findings in The Anterior Cruciate Ligament Deficient Knee Prior To Reconstructive SurgeryDocument3 pages53 - Changes in Arthroscopic Findings in The Anterior Cruciate Ligament Deficient Knee Prior To Reconstructive SurgeryrandocalNo ratings yet
- 5 6201509562231555914Document7 pages5 6201509562231555914Rahul ReddyNo ratings yet
- Triple Arthrodesis in Rheumatoid ArthritisDocument5 pagesTriple Arthrodesis in Rheumatoid ArthritisZahrotul Fitria SuryawanNo ratings yet
- Fifteen-Year To 19-Year Follow-Up of The Insall-Burstein-1 Total Knee ArthroplastyDocument6 pagesFifteen-Year To 19-Year Follow-Up of The Insall-Burstein-1 Total Knee ArthroplastyFajar BascNo ratings yet
- Evaluation of The Results From Surgical Treatment of The Terrible Triad of The ElbowDocument8 pagesEvaluation of The Results From Surgical Treatment of The Terrible Triad of The ElbowBruno FellipeNo ratings yet
- A Long Term Follow Up Study of Total Meniscectomy.30Document5 pagesA Long Term Follow Up Study of Total Meniscectomy.30Anshal GuptaNo ratings yet
- Chalmers 2019Document6 pagesChalmers 2019Spoti PremiNo ratings yet
- Polesello 2014Document7 pagesPolesello 2014moonwalker2099No ratings yet
- Spori ArticleDocument12 pagesSpori ArticleKyla Agbon ArbaniaNo ratings yet
- Talar Neck FracturesDocument6 pagesTalar Neck FracturesherpthederpNo ratings yet
- 2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceDocument8 pages2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceJacob DoughertyNo ratings yet
- Elmoumni2012 Long-Term Functional Outcome Following Intramedullary Nailing ofDocument5 pagesElmoumni2012 Long-Term Functional Outcome Following Intramedullary Nailing ofJian Wei LowNo ratings yet
- Range of Motion and Strength After Surgery For Brachial Plexus Birth PalsyDocument7 pagesRange of Motion and Strength After Surgery For Brachial Plexus Birth PalsydespNo ratings yet
- External Rotator Sparing W KL in Post Acetab FX Hindawi14Document7 pagesExternal Rotator Sparing W KL in Post Acetab FX Hindawi14Antonio PáezNo ratings yet
- Necrosis Avascular de Humero Criterios de HertelDocument7 pagesNecrosis Avascular de Humero Criterios de Hertelluis perezNo ratings yet
- Foot & Ankle International: Minimal Incision Surgery For Tibiotalocalcaneal ArthrodesisDocument14 pagesFoot & Ankle International: Minimal Incision Surgery For Tibiotalocalcaneal Arthrodesisapi-241264935No ratings yet
- 1 The Prevalence, Zone, and Type of The Meniscus TearDocument7 pages1 The Prevalence, Zone, and Type of The Meniscus TearnguyenthanhsangydsNo ratings yet
- Low Thoracic and Lumbar Burst Fractures - Radiographic and Functional OutcomesDocument10 pagesLow Thoracic and Lumbar Burst Fractures - Radiographic and Functional Outcomesmuhammad bayu wicaksonoNo ratings yet
- Laprade 2012Document11 pagesLaprade 2012Aaron BNo ratings yet
- 2002 Scarf FundaDocument9 pages2002 Scarf FundaRuth Aydeé SoláNo ratings yet
- Short Versus Long Outcome RadiologisDocument7 pagesShort Versus Long Outcome Radiologisandy ardiansyahNo ratings yet
- Clinical Outcome After Undisplaced Femoral Neck FracturesDocument7 pagesClinical Outcome After Undisplaced Femoral Neck FracturesCraciun Ana-MariaNo ratings yet
- Fractures of The Scapular Neck: Diagnosis, Classifications and TreatmentDocument11 pagesFractures of The Scapular Neck: Diagnosis, Classifications and Treatmentsoheil ostovanNo ratings yet
- 10 Aligizakis HadjipavlouDocument9 pages10 Aligizakis HadjipavlouI Made Dhita PriantharaNo ratings yet
- Our Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteDocument11 pagesOur Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteAthenaeum Scientific PublishersNo ratings yet
- Evaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramDocument13 pagesEvaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramZzDel VerdeNo ratings yet
- 1 s2.0 S0749806317312173 MainDocument8 pages1 s2.0 S0749806317312173 MaindragaancaNo ratings yet
- Bulut 2018Document5 pagesBulut 2018José Luis Velasquez UrregoNo ratings yet
- Association of Pars Defect Type With Clinical Outcome After Smiley Face Rod Methods For Terminal-Stage SpondylolysisDocument8 pagesAssociation of Pars Defect Type With Clinical Outcome After Smiley Face Rod Methods For Terminal-Stage SpondylolysisUzm.Dr.Burhan ORAL GÜDÜNo ratings yet
- 264 2013 Article 2112Document6 pages264 2013 Article 2112Anil KumarNo ratings yet
- The Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklDocument5 pagesThe Modified Brostr M Gould Procedure - Early Results Usi - 2014 - Foot and AnklFyodorovich Makarov NikolaiNo ratings yet
- Effects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric StudyDocument8 pagesEffects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric Studysiti hanifahNo ratings yet
- Functional Treatment Versus Plaster For Simple Elbow Dislocations (Funcsie) : A Randomized TrialDocument7 pagesFunctional Treatment Versus Plaster For Simple Elbow Dislocations (Funcsie) : A Randomized TrialTekhaDwiNo ratings yet
- Avascular Necrosis As A Complication of The Treatment of Dislocation of The Hip in Children With Cerebral PalsyDocument7 pagesAvascular Necrosis As A Complication of The Treatment of Dislocation of The Hip in Children With Cerebral PalsyDeepak NemaniNo ratings yet
- Reliability of Classification For Post Traumatic Ankle OsteoarthritisDocument6 pagesReliability of Classification For Post Traumatic Ankle OsteoarthritisDewi RoziqoNo ratings yet
- Brief Resume of Intended WorkDocument7 pagesBrief Resume of Intended WorkNavin ChandarNo ratings yet
- Surgical Treatment of Dorsal Perilunate Fracture-DislocationsDocument7 pagesSurgical Treatment of Dorsal Perilunate Fracture-DislocationsJuanHoyosNo ratings yet
- DL TPSFDocument5 pagesDL TPSFPramod N KNo ratings yet
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDocument8 pagesMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersNo ratings yet
- FAI DiagnosisDocument6 pagesFAI DiagnosisRudolfGerNo ratings yet
- 義大醫學雜誌 - 78 - Non-periarticular locking plates for complicated and - or geriatric olecranon fractures - V2Document17 pages義大醫學雜誌 - 78 - Non-periarticular locking plates for complicated and - or geriatric olecranon fractures - V2bigben9262No ratings yet
- Surgical Treatment of Winged ScapulaDocument10 pagesSurgical Treatment of Winged ScapulamamshivaNo ratings yet
- Chloros2008 231022 130529Document12 pagesChloros2008 231022 130529Cristian SanchezNo ratings yet
- Bessire 2014Document7 pagesBessire 2014andrei3cucuNo ratings yet
- U01 Clavicle InjuriesDocument121 pagesU01 Clavicle Injuriesadrian_mogosNo ratings yet
- Journal Analysis of Fractured MandibleDocument5 pagesJournal Analysis of Fractured MandiblePrazna ShafiraNo ratings yet
- Art:10.1186/1756 0500 7 569Document6 pagesArt:10.1186/1756 0500 7 569Fuioaga Codrin-PaulNo ratings yet
- Magnusson 2006 Absorbable Implants For Open Shoulder Stabilization. A 7-8-Year Clinical and Radiographic Follow-UpDocument7 pagesMagnusson 2006 Absorbable Implants For Open Shoulder Stabilization. A 7-8-Year Clinical and Radiographic Follow-UptheorthopaedistNo ratings yet
- Asensio, JA, (2020) - Tratamiento Quirúrgico de Las Lesiones de La Arteria Braquial y Predictores de Resultado.Document12 pagesAsensio, JA, (2020) - Tratamiento Quirúrgico de Las Lesiones de La Arteria Braquial y Predictores de Resultado.Edgar Geovanny Cardenas FigueroaNo ratings yet
- Percutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsDocument7 pagesPercutaneous Endoscopic Decompression Via Transforaminal Approach For Lumbar Lateral Recess Stenosis in Geriatric PatientsAmina GoharyNo ratings yet
- Functional Outcome of Ipsilateral Intertrochanteric and Femoral Shaft FracturesDocument5 pagesFunctional Outcome of Ipsilateral Intertrochanteric and Femoral Shaft Fracturesbutterflybaby04No ratings yet
- Revisit To Scapular Dyskinesis - Three-Dimensional Wing Computed Tomography in Prone PositionDocument8 pagesRevisit To Scapular Dyskinesis - Three-Dimensional Wing Computed Tomography in Prone PositionDaniel CarcamoNo ratings yet
- Modi Ed Percutaneous Kirschner Wire With Mutual Linking Technique in Proximal Humeral Fracture: A Technique Note and Preliminary ResultsDocument14 pagesModi Ed Percutaneous Kirschner Wire With Mutual Linking Technique in Proximal Humeral Fracture: A Technique Note and Preliminary ResultsRahul ReddyNo ratings yet
- Tur CicaDocument8 pagesTur CicazubayetarkoNo ratings yet
- Total Hip Arthroplasty in Patients With DwarfismDocument7 pagesTotal Hip Arthroplasty in Patients With DwarfismDhecy Pngent PergydaridunianieNo ratings yet
- Jarvis 2017Document5 pagesJarvis 2017drelvNo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- EssayDocument14 pagesEssaysurajplplusNo ratings yet
- SLFRF Recovery Plan Performance Report TemplateDocument11 pagesSLFRF Recovery Plan Performance Report TemplateEdwin L. ColonNo ratings yet
- Financial Management Has An Impact On People of All AgesDocument8 pagesFinancial Management Has An Impact On People of All AgesElizabeth OlarteNo ratings yet
- Anino NG Kahapon Reflection Paper - CarandangDocument2 pagesAnino NG Kahapon Reflection Paper - Carandangkarl.carandangNo ratings yet
- NDT Lec FinalsDocument25 pagesNDT Lec FinalsAkashi SilvanoNo ratings yet
- Test Bank For Anatomy Physiology and Disease An Interactive Journey For Health Professions 2nd Edition ColbertDocument26 pagesTest Bank For Anatomy Physiology and Disease An Interactive Journey For Health Professions 2nd Edition ColbertMarvin Moore100% (40)
- Test Description Value(s) Unit Reference RangeDocument5 pagesTest Description Value(s) Unit Reference RangeGalaxys KitchensNo ratings yet
- Comparative Study of Tooth Size and Arch Dimensions in Class I Crowded, Proclined Malocclusion and Class I Normal OcclusionDocument5 pagesComparative Study of Tooth Size and Arch Dimensions in Class I Crowded, Proclined Malocclusion and Class I Normal OcclusionSyed Mohammad Osama AhsanNo ratings yet
- Herbal MedicinesDocument22 pagesHerbal Medicineszaynab.20903008No ratings yet
- Cse205Document25 pagesCse205Aman SinghNo ratings yet
- Surgical Complications of Minor Oral SurgeryDocument53 pagesSurgical Complications of Minor Oral SurgeryDrNagendra Dutt Sharma100% (1)
- Case Study "John Rick Corpuz"Document2 pagesCase Study "John Rick Corpuz"sir jjNo ratings yet
- Human Resources For Health: What Difference Does ("Good") HRM Make?Document7 pagesHuman Resources For Health: What Difference Does ("Good") HRM Make?Shah NewazNo ratings yet
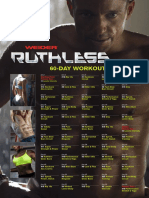
- Ruthless Workout Calendar PDFDocument1 pageRuthless Workout Calendar PDF陳韋佳No ratings yet
- Food Safety in Bangladesh PDFDocument8 pagesFood Safety in Bangladesh PDFSaleh AhmedNo ratings yet
- Pengetahuan, Sikap, Dan Perilaku Terhadap Pencegahan Serta Penanggulangan Hipertensi Di Kabupaten BogorDocument9 pagesPengetahuan, Sikap, Dan Perilaku Terhadap Pencegahan Serta Penanggulangan Hipertensi Di Kabupaten BogorIntan OktavianiNo ratings yet
- Case Study SMALLPOX ERADICATIONDocument3 pagesCase Study SMALLPOX ERADICATIONSimran WaghelaNo ratings yet
- Aesculap Pedicle Screw Supply Chain Study PDFDocument1 pageAesculap Pedicle Screw Supply Chain Study PDFJasonNo ratings yet
- McClelland 2014 Intimate JusticeDocument4 pagesMcClelland 2014 Intimate JusticeCristóbal AstorgaNo ratings yet
- DF Premium Engine 10W-40 (2014)Document1 pageDF Premium Engine 10W-40 (2014)Florin TomaNo ratings yet
- Top PrefDocument4 pagesTop PrefCamae Snyder GangcuangcoNo ratings yet
- Hospital SettingDocument20 pagesHospital SettingDwi Syahrani TaufiqNo ratings yet
- DLL FebDocument3 pagesDLL FebHomemade BarquillosNo ratings yet
- Midlife Crisis - Signs, Causes, and Coping TipsDocument13 pagesMidlife Crisis - Signs, Causes, and Coping TipsMonyesmaNo ratings yet