You might also like
- Deped-National Capital Region Health Declaration Checklist: Please Provide Answer To The Following: Yes NoDocument1 pageDeped-National Capital Region Health Declaration Checklist: Please Provide Answer To The Following: Yes NoRegine P. VictorioNo ratings yet
- Visitor Health Declaration FormDocument2 pagesVisitor Health Declaration FormKaryl Eunice Macabale IboniaNo ratings yet
- Annex B - Health Screening Form For VisitorsDocument1 pageAnnex B - Health Screening Form For VisitorsReynaldo YuNo ratings yet
- Covid FormDocument3 pagesCovid FormGena Fe L. JagusNo ratings yet
- Health Screening Form For Visitors: Dear Valued Clients and VisitorsDocument1 pageHealth Screening Form For Visitors: Dear Valued Clients and VisitorsBhonNo ratings yet
- Health Declaration ChecklistDocument1 pageHealth Declaration ChecklistE Viv FuentesNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJilli JardiolinNo ratings yet
- Department of Education: Deped Region 7 Covid-19 Assessment Form (Decaf)Document2 pagesDepartment of Education: Deped Region 7 Covid-19 Assessment Form (Decaf)Goldie ParazNo ratings yet
- FORM 002 - Personal DataDocument2 pagesFORM 002 - Personal DataSholihin Syah PutraNo ratings yet
- Inbound 2251609052538566261Document1 pageInbound 2251609052538566261sam.sarip0No ratings yet
- Deped - Health Declaration Form 2020Document1 pageDeped - Health Declaration Form 2020LHEYA AQUINO100% (5)
- Student App Letter VVVVVVVVVVVDocument2 pagesStudent App Letter VVVVVVVVVVVAlyssa Leah Veloso EvangelistaNo ratings yet
- Region Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolDocument2 pagesRegion Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolHUMSS 11-BNo ratings yet
- ACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DEDocument1 pageACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DERoden BernardoNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersRE:BORN MLNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersLyrics KingNo ratings yet
- Health Declaration FormDocument3 pagesHealth Declaration FormJocelyn PepitoNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormQuantum XavierNo ratings yet
- Health Declaration Form AutorecoveredDocument2 pagesHealth Declaration Form AutorecoveredMary Anne SantosNo ratings yet
- Mta Forms Rev.01 Cy2022Document9 pagesMta Forms Rev.01 Cy2022Kristelle BrionesNo ratings yet
- Application Form: Legal Scholarship Program ACADEMIC YEAR 2020-2021Document2 pagesApplication Form: Legal Scholarship Program ACADEMIC YEAR 2020-2021Michelle RamaNo ratings yet
- Please Answer The Following Questions Truthfully. 2.: Tick Yes/NoDocument2 pagesPlease Answer The Following Questions Truthfully. 2.: Tick Yes/NoSusan Loida SorianoNo ratings yet
- Declaration Form (COVID)Document1 pageDeclaration Form (COVID)Pamela Joyce MaddumaNo ratings yet
- Training Agreement and Liability WaiverDocument4 pagesTraining Agreement and Liability WaiverOscar MirandaNo ratings yet
- Daily Health ChecklistDocument2 pagesDaily Health ChecklistMa. Charlene SisonNo ratings yet
- Genesis Academy Pre-K Program Registration Form: Child's InformationDocument7 pagesGenesis Academy Pre-K Program Registration Form: Child's InformationPhillip M JonesNo ratings yet
- Health ChecklistDocument14 pagesHealth ChecklistClark Kent BatucanNo ratings yet
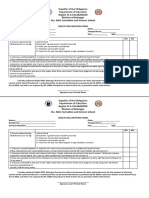
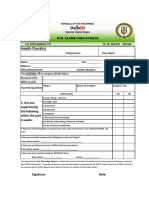
- Health Checklist: Sta. Elena High SchoolDocument1 pageHealth Checklist: Sta. Elena High SchoolAnarica Mae MendozaNo ratings yet
- Health Declaration FinalDocument1 pageHealth Declaration FinalFRANZI ALYANNA MUGARNo ratings yet
- (AdC) Benilde Legal Guardianship FormDocument1 page(AdC) Benilde Legal Guardianship Formjlorinserm16No ratings yet
- Waiver Sosial WorkDocument1 pageWaiver Sosial Workian macadangdangNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersLourd Juan Artuz MustafaNo ratings yet
- CGHNNNDocument2 pagesCGHNNNRobert NemoNo ratings yet
- 00062018031900958Document2 pages00062018031900958Pamela BachichaNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersJay Michael RustiaNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersImelda aquinoNo ratings yet
- Online PassportingDocument4 pagesOnline PassportingKathaliya SarcenoNo ratings yet
- Application Form For Incoming Grade 7Document1 pageApplication Form For Incoming Grade 7Gladylyn MirandaNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersMark Loui Rotersos CasipongNo ratings yet
- Important RemindersDocument2 pagesImportant RemindersNeza BrietaNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersDioneri Dag-uman MedinaNo ratings yet
- MLP Registration FormDocument6 pagesMLP Registration FormDoll JonesNo ratings yet
- Summer Youth Camp 2022 ApplicationDocument8 pagesSummer Youth Camp 2022 ApplicationErika EsquivelNo ratings yet
- Sample Dfa FormatDocument4 pagesSample Dfa FormatJohn TinNo ratings yet
- Parental Consent 1Document2 pagesParental Consent 1Crisandra Angel Coquilla CabrerosNo ratings yet
- SportsDocument4 pagesSportsWinty BandalNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersTan TanNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration Formmalaki ang titik ONo ratings yet
- (E) Hostel Form-DPSB - A4Document4 pages(E) Hostel Form-DPSB - A4ghjegjwNo ratings yet
- Registration Form For PDO's 2018Document5 pagesRegistration Form For PDO's 2018Catherine Christine HarrisNo ratings yet
- Important RemindersDocument16 pagesImportant RemindersMichael KitNo ratings yet
- Important RemindersDocument2 pagesImportant RemindersMark Anthony B. AquinoNo ratings yet
- Date: - : Health Declaration Form #COVID-19Document2 pagesDate: - : Health Declaration Form #COVID-19Hanna BananaNo ratings yet
- Little Lambs Preschool ApplicationDocument12 pagesLittle Lambs Preschool ApplicationNoopur JainNo ratings yet
- Parents PermitDocument2 pagesParents PermitJay BolanoNo ratings yet
- Important RemindersDocument4 pagesImportant Remindersrichelle salesNo ratings yet
- SwimmingPool Membership FormDocument1 pageSwimmingPool Membership FormSrujana MohantyNo ratings yet
- Alexander B. Maranguez: ObjectivesDocument3 pagesAlexander B. Maranguez: ObjectivesMhary AngelNo ratings yet
- Saturday: Signature SignatureDocument3 pagesSaturday: Signature SignatureMhary AngelNo ratings yet
- RHEADocument3 pagesRHEAMhary AngelNo ratings yet
- Cara DTRDocument1 pageCara DTRMhary AngelNo ratings yet
- Science 5 Directions: Choose The Letter of The Correct AnswerDocument1 pageScience 5 Directions: Choose The Letter of The Correct AnswerMhary AngelNo ratings yet
- Match Column A With Column BDocument1 pageMatch Column A With Column BMhary AngelNo ratings yet
- Korean Word MeaningDocument27 pagesKorean Word MeaningMhary AngelNo ratings yet
- Iesu, Panis VitaeDocument13 pagesIesu, Panis VitaeMhary AngelNo ratings yet
- Select All Letters: Click The Small Letter of (A) To Reduce The Letters You SelectedDocument3 pagesSelect All Letters: Click The Small Letter of (A) To Reduce The Letters You SelectedMhary AngelNo ratings yet
- Korean Word Meaning 2Document26 pagesKorean Word Meaning 2Mhary AngelNo ratings yet
- Tequillo, Jorge Verallo: Position Desired: Driver Personal DataDocument1 pageTequillo, Jorge Verallo: Position Desired: Driver Personal DataMhary AngelNo ratings yet