You might also like
- A Field Guide To Medicinal Plants Eastern and Central North America Peterson Field Guide SeriesDocument892 pagesA Field Guide To Medicinal Plants Eastern and Central North America Peterson Field Guide SeriesExness Việt Nam0% (1)
- Contamination Control Basics Risk and ResolutionDocument86 pagesContamination Control Basics Risk and ResolutionBLUEPRINT Integrated Engineering Services100% (2)
- Basic Edgewise TechniqueDocument109 pagesBasic Edgewise TechniqueRajshekhar Banerjee100% (1)
- Programming of ArticulatorsDocument3 pagesProgramming of ArticulatorsSHAILJA KATIYAR83% (6)
- Rui Silva Monaco TPS Webinar PresentationDocument18 pagesRui Silva Monaco TPS Webinar PresentationHidajeta ĐedovićNo ratings yet
- Health Declaration Form - A1Document1 pageHealth Declaration Form - A1TOPNOTCHER Philippines71% (7)
- Deped - Health Declaration Form 2020Document1 pageDeped - Health Declaration Form 2020Dadz Inocente80% (5)
- Askep Ppok - Kelompok 1Document17 pagesAskep Ppok - Kelompok 1super manggis100% (1)
- Covid FormDocument3 pagesCovid FormGena Fe L. JagusNo ratings yet
- Health Declaration With Covid VaccinationDocument1 pageHealth Declaration With Covid Vaccinationchiaruuh tNo ratings yet
- Region Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolDocument2 pagesRegion Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolHUMSS 11-BNo ratings yet
- Cecilio Apostol Elementary School Attendees' Health ChecklistDocument1 pageCecilio Apostol Elementary School Attendees' Health ChecklistMikoy Fordan AntolinoNo ratings yet
- HD - Reception SantierraDocument1 pageHD - Reception SantierraAnezka Danett CortinaNo ratings yet
- Deped RequirementsDocument1 pageDeped RequirementsWelmie Unasco GregorioNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration Formmalaki ang titik ONo ratings yet
- Visitor Health Declaration FormDocument2 pagesVisitor Health Declaration FormKaryl Eunice Macabale IboniaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formasansur esNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJilli JardiolinNo ratings yet
- Deped Monitoring ChecklistDocument1 pageDeped Monitoring ChecklistWelmie Unasco GregorioNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- Department of Education: Health Declaration FormDocument2 pagesDepartment of Education: Health Declaration FormMaysie BiraquitNo ratings yet
- Health Checklist Health ChecklistDocument2 pagesHealth Checklist Health ChecklistMaria Rhoda C. FontanillaNo ratings yet
- Barangay Employee Health Declaration FormDocument2 pagesBarangay Employee Health Declaration FormBarangay CentroNo ratings yet
- Visitors Health Checklist Form (From DTI and DOLE)Document1 pageVisitors Health Checklist Form (From DTI and DOLE)melbaNo ratings yet
- Health-Declaration-Form 2Document1 pageHealth-Declaration-Form 2menchieNo ratings yet
- Health Declaration FinalDocument1 pageHealth Declaration FinalFRANZI ALYANNA MUGARNo ratings yet
- Health Declaration Form 1Document2 pagesHealth Declaration Form 1Elorde M. ShalaniNo ratings yet
- Health Dec.Document2 pagesHealth Dec.Gienniva FulgencioNo ratings yet
- ISO Health ChecklistDocument1 pageISO Health ChecklistRonnel SaludezNo ratings yet
- (Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureDocument1 page(Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureJayl 22No ratings yet
- Students Health SurveyDocument1 pageStudents Health SurveyJulie Basbas-CruzNo ratings yet
- Health Declaration Form: Department of EducationDocument5 pagesHealth Declaration Form: Department of Educationrosario lanzadoNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesMhary Angel100% (1)
- Health Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Document1 pageHealth Checklist Form: (Nakakaranas Ka Ba NG:) (Pananakit NG Lalamunan / Masakit Lumunok)Jhon Micheal AlicandoNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesJameena MagallanesNo ratings yet
- Temperature:: Signature Over Printed NameDocument2 pagesTemperature:: Signature Over Printed NameBarangay CentroNo ratings yet
- Employee (S) Health Checklists Employee (S) Health ChecklistsDocument2 pagesEmployee (S) Health Checklists Employee (S) Health ChecklistsRollie MimisNo ratings yet
- Health Checklist Employees 1 Converted 1Document2 pagesHealth Checklist Employees 1 Converted 1the7thAliceNo ratings yet
- Health DEclaration Form SET ADocument26 pagesHealth DEclaration Form SET AROLLY BALONo ratings yet
- Health Declaration Form - 1606903543Document1 pageHealth Declaration Form - 1606903543Patrick GregorioNo ratings yet
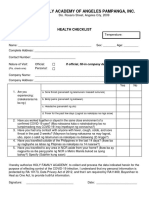
- Holy Family Academy of Angeles Pampanga, Inc.: Health ChecklistDocument1 pageHoly Family Academy of Angeles Pampanga, Inc.: Health ChecklistKarlNo ratings yet
- Health DeclarationDocument1 pageHealth DeclarationVanessa MendezNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormNrc A.No ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PagemarieleNo ratings yet
- Health Declaration: YES NODocument1 pageHealth Declaration: YES NOEliezal Dean B. CardeñoNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageJoezerk CarpioNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageFedelyn SemenianoNo ratings yet
- Health Form For Civil Service ExamDocument1 pageHealth Form For Civil Service Examralph sabaNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageMiamor NatividadNo ratings yet
- HDF PDFDocument1 pageHDF PDFJhon Rey GonsalezNo ratings yet
- Tanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormDocument4 pagesTanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormKurt VillaNo ratings yet
- Workplace Prevention and Control of CovidDocument1 pageWorkplace Prevention and Control of Coviddee dee sevachNo ratings yet
- SMI COVID-19 Health Survey Form - RevisedDocument2 pagesSMI COVID-19 Health Survey Form - RevisedJess Rey Q. BaranNo ratings yet
- Covid ChecklistDocument1 pageCovid ChecklistAnnabe L. GabalesNo ratings yet
- Orca Share Media1659750221349 6961496992414198469Document1 pageOrca Share Media1659750221349 6961496992414198469Vladd DreiNo ratings yet
- Health Declaration Form1Document2 pagesHealth Declaration Form1JULCON ARAIZNo ratings yet
- Health Form Health FormDocument2 pagesHealth Form Health FormMarielou BunielNo ratings yet
- (Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureDocument1 page(Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureNatividad Jo Ann CuadroNo ratings yet
- Health Declaration Form - A1 Whole Page - ADocument1 pageHealth Declaration Form - A1 Whole Page - AMARCK JOHN EUSTAQUIONo ratings yet
- Deped Vigan City Covid19 Health ChecklistDocument1 pageDeped Vigan City Covid19 Health ChecklistLemmor ObarNo ratings yet
- Screening Questionnaire (Workplace Prevention and Control)Document1 pageScreening Questionnaire (Workplace Prevention and Control)Tristan BabaylanNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormQuantum XavierNo ratings yet
- Health Declaration Temperature: Temperature:: (Nakakaranas Ka Ba NG?) Lumunok)Document3 pagesHealth Declaration Temperature: Temperature:: (Nakakaranas Ka Ba NG?) Lumunok)Jenica LulunanNo ratings yet
- Deped - Health Declaration Form 2020Document1 pageDeped - Health Declaration Form 2020LHEYA AQUINO100% (5)
- ACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DEDocument1 pageACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DERoden BernardoNo ratings yet
- Your Best Is yet to Come!: Believe-Educate-Stand-Tall Information on the Covid-19 Vaccination, Inhalation, or PillFrom EverandYour Best Is yet to Come!: Believe-Educate-Stand-Tall Information on the Covid-19 Vaccination, Inhalation, or PillNo ratings yet
- Microbiology 3M All 333Document55 pagesMicrobiology 3M All 333deeksha.ivannaNo ratings yet
- Desain GTSL SangryDocument53 pagesDesain GTSL SangrySanggry Mutiara PardedeNo ratings yet
- ფიზიოლოგიური მშობიარობის მართვაDocument30 pagesფიზიოლოგიური მშობიარობის მართვაAchi BeridzeNo ratings yet
- Daftar Obat Lasa Dan High Alert Yang Diberi LabelDocument3 pagesDaftar Obat Lasa Dan High Alert Yang Diberi LabelNila Permata SariNo ratings yet
- End of Life Care DiscussionDocument2 pagesEnd of Life Care Discussionalexander abasNo ratings yet
- SVU TestDocument23 pagesSVU TestkawarolanNo ratings yet
- Scenario Presentation Newborn in Need of PPV and IntubationDocument3 pagesScenario Presentation Newborn in Need of PPV and IntubationMaria PârghieNo ratings yet
- National External Quality Assessment SchemeDocument3 pagesNational External Quality Assessment SchemeGlysa MaeNo ratings yet
- Analysis and Interpretation of The Epidaurian IamataDocument16 pagesAnalysis and Interpretation of The Epidaurian IamataKrupeninNo ratings yet
- DRHDocument3 pagesDRHMaulana Malik IbrahimNo ratings yet
- ObhkvhbbDocument82 pagesObhkvhbbNoviana Mardha Tilla HaryantoNo ratings yet
- Company Profile Indo Medika InternationalDocument12 pagesCompany Profile Indo Medika InternationalshavinravizaNo ratings yet
- ULLURUDocument5 pagesULLURUTho SagarNo ratings yet
- Nama: Karina Chania Dan Amalia Lenanda Kelas/Prodi: 2B/D3 Keperawatan Topic 4 General Assessment ConversationDocument3 pagesNama: Karina Chania Dan Amalia Lenanda Kelas/Prodi: 2B/D3 Keperawatan Topic 4 General Assessment ConversationKarina ChaniaNo ratings yet
- An Evaluation of Four Decades of Cuban Healthcare: Felipe Eduardo SixtoDocument19 pagesAn Evaluation of Four Decades of Cuban Healthcare: Felipe Eduardo SixtoAvicenna AkbarNo ratings yet
- Technical Data Sheet: Infusion Administration Sets For Gravity, VentedDocument9 pagesTechnical Data Sheet: Infusion Administration Sets For Gravity, VentedhalaberawanNo ratings yet
- A Brief Analysis of The Connection Between EBP and The Quadruple AimDocument5 pagesA Brief Analysis of The Connection Between EBP and The Quadruple AimChacha PeterNo ratings yet
- Lista Gratuidade EAN 14.02.2020Document10 pagesLista Gratuidade EAN 14.02.2020Lidia Dias GonçalvesNo ratings yet
- LP 1 Lesson 7Document5 pagesLP 1 Lesson 7Bainaot Abdul SumaelNo ratings yet
- Magsaysay v. NLRCDocument17 pagesMagsaysay v. NLRCJohn BernalNo ratings yet
- Borang Ambulans CallDocument2 pagesBorang Ambulans Callleo89azman100% (1)
- 2497-Article Text-5889-1-10-20230628Document12 pages2497-Article Text-5889-1-10-20230628rodu5648No ratings yet
- Jesna James Resume PDFDocument4 pagesJesna James Resume PDFapi-566615902No ratings yet
- 001 240506964 Ce8 117 3Document1 page001 240506964 Ce8 117 3sadiahas2014No ratings yet