You might also like
- Caterpillar Global Solutions: 50/60 HZ Switchable Genset Ipp Application (Wiring)Document19 pagesCaterpillar Global Solutions: 50/60 HZ Switchable Genset Ipp Application (Wiring)Jonathan Javier Ceballos Bonilla100% (2)
- A320 TakeoffDocument17 pagesA320 Takeoffpp100% (1)
- Motion To Release AccusedDocument3 pagesMotion To Release AccusedStef OcsalevNo ratings yet
- PLC Work BookDocument15 pagesPLC Work BookAsrarLoonNo ratings yet
- Sephora Brand AuditDocument30 pagesSephora Brand Auditapi-294767507100% (2)
- The Return of Population Control: Incentives, Targets, and The Backlash Against CairoDocument4 pagesThe Return of Population Control: Incentives, Targets, and The Backlash Against CairoPopulation & Development Program (PopDev)100% (1)
- Midrand Montessori Preschool EnrolmentDocument8 pagesMidrand Montessori Preschool Enrolmentanarki85No ratings yet
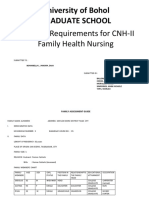
- Family Assessment Guide: Family Member'S ChartDocument6 pagesFamily Assessment Guide: Family Member'S ChartJULIANNE BAYHONNo ratings yet
- Power Distribution Systems and Its Characteristics IDocument16 pagesPower Distribution Systems and Its Characteristics IMohammedSaadaniHassani100% (1)
- Configuration Steps - Settlement Management in S - 4 HANA - SAP BlogsDocument30 pagesConfiguration Steps - Settlement Management in S - 4 HANA - SAP Blogsenza100% (4)
- Deped - Health Declaration Form 2020Document1 pageDeped - Health Declaration Form 2020Dadz Inocente80% (5)
- Tyco Hypermist - Full Manual (Recvd 22.04.2013)Document40 pagesTyco Hypermist - Full Manual (Recvd 22.04.2013)Rachit100% (2)
- Cool for School: A Guide to Ensuring Your Child’s Success in School.From EverandCool for School: A Guide to Ensuring Your Child’s Success in School.No ratings yet
- Action Plan For School-Based Learning Action Cell (Slac)Document5 pagesAction Plan For School-Based Learning Action Cell (Slac)rosario lanzadoNo ratings yet
- Endorsement Papers For Maternity LeaveDocument1 pageEndorsement Papers For Maternity LeaveMariel EfrenNo ratings yet
- Region Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolDocument2 pagesRegion Iv-A Calabarzon Division of Batangas Sto. Niño Formation and Science SchoolHUMSS 11-BNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormQuantum XavierNo ratings yet
- Department of Education: Health Declaration FormDocument2 pagesDepartment of Education: Health Declaration FormMaysie BiraquitNo ratings yet
- Health ChecklistDocument14 pagesHealth ChecklistClark Kent BatucanNo ratings yet
- Andabuen National High School: Benito Soliven South DistrictDocument3 pagesAndabuen National High School: Benito Soliven South DistrictRonalyn ColladoNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJilli JardiolinNo ratings yet
- Travel History Disclosure FormDocument5 pagesTravel History Disclosure FormMarianne Christie RagayNo ratings yet
- Health Dec.Document2 pagesHealth Dec.Gienniva FulgencioNo ratings yet
- Deped - Health Declaration Form 2020Document1 pageDeped - Health Declaration Form 2020LHEYA AQUINO100% (5)
- Health Declaration Form LoveDocument1 pageHealth Declaration Form LoveRen Ren MartinezNo ratings yet
- Deped Health Declaration Form 2020Document1 pageDeped Health Declaration Form 2020Mitzi Faye CabbabNo ratings yet
- Parent Consent and Health Screening FormsDocument6 pagesParent Consent and Health Screening FormsJohn Paulo RamosNo ratings yet
- Visitors Health Declaration FormDocument1 pageVisitors Health Declaration FormRobei May BedolidoNo ratings yet
- LearnersprofileDocument1 pageLearnersprofileC YamixtheGamerNo ratings yet
- (Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureDocument1 page(Nakakaranas Ka Ba NG?) Masakit Lumunok) : Health Declaration TemperatureNatividad Jo Ann CuadroNo ratings yet
- Cecilio Apostol Elementary School Attendees' Health ChecklistDocument1 pageCecilio Apostol Elementary School Attendees' Health ChecklistMikoy Fordan AntolinoNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formasansur esNo ratings yet
- ACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DEDocument1 pageACFrOgDQCRWX - vfxXPYGLNrZUsJXQw9CzGCMTZkGyEx aN5Riz4zIOh7yeJsLmXZUVRr0wPBruB2hiRdJgwtk7INI8tSSDe9jRp9TpxKG5JMu0 XLGhMMThT9 - 19DERoden BernardoNo ratings yet
- Anecdotal-New (Child - S Personal Data)Document3 pagesAnecdotal-New (Child - S Personal Data)Belinda JeresanoNo ratings yet
- HEALTH DECLARATION FORM For CovidDocument2 pagesHEALTH DECLARATION FORM For CovidRenato Urolaza IgnacioNo ratings yet
- Family Health AssessmentDocument6 pagesFamily Health AssessmentSitti Shayra LandasanNo ratings yet
- Forms 1 5 For Registration 2021 Mame 1Document15 pagesForms 1 5 For Registration 2021 Mame 1Emma DionedaNo ratings yet
- Department of Education: Republic of The PhilippinesDocument3 pagesDepartment of Education: Republic of The PhilippinesJulianne Jane Diongson100% (1)
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration Formmalaki ang titik ONo ratings yet
- Individual Student Inventory FormDocument2 pagesIndividual Student Inventory Formmahinaybabyjean32No ratings yet
- Parent'S/Guardian'S Consent: Departmentof EducationDocument1 pageParent'S/Guardian'S Consent: Departmentof Educationrosario lanzadoNo ratings yet
- Waiver Sosial WorkDocument1 pageWaiver Sosial Workian macadangdangNo ratings yet
- Parents Permit - SurveyDocument2 pagesParents Permit - SurveyGeneve GarzonNo ratings yet
- COVID 19 Health Declaration and Liability Waiver For New Normal CampingDocument2 pagesCOVID 19 Health Declaration and Liability Waiver For New Normal CampingTelapatio Elementary School (R III - Bulacan)No ratings yet
- Health DEclaration Form SET ADocument26 pagesHealth DEclaration Form SET AROLLY BALONo ratings yet
- Republic of The Philippines: Lyn-Lyn M. YuDocument2 pagesRepublic of The Philippines: Lyn-Lyn M. YuLYN-LYN YUNo ratings yet
- New Registration Form (1236)Document10 pagesNew Registration Form (1236)Diana BalanuţaNo ratings yet
- Health Declaration Form1Document2 pagesHealth Declaration Form1JULCON ARAIZNo ratings yet
- FC - Observation FormDocument6 pagesFC - Observation FormGlenda Ang BacomoNo ratings yet
- Individual Inventory Record FormDocument2 pagesIndividual Inventory Record Formapple joyce casayuranNo ratings yet
- School Covid Response Limited Face-To-Face Covid Referral Flowchart SY 2021 - 2022Document5 pagesSchool Covid Response Limited Face-To-Face Covid Referral Flowchart SY 2021 - 2022Jayson LambanicioNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlintana JobelleNo ratings yet
- Health FormDocument2 pagesHealth FormChristine BacordoNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration FormYanna AbarquezNo ratings yet
- Deed of DonationsDocument2 pagesDeed of DonationsDANA FE RAGATNo ratings yet
- Learners Profile FormDocument2 pagesLearners Profile FormMarie KenNo ratings yet
- Consent Letter For VaccinationDocument2 pagesConsent Letter For VaccinationNesslee Jane Alberastine TigasNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesMhary Angel100% (1)
- Learner'S Health Record: Gen. A. Luna ST., Ususan, Taguig CityDocument1 pageLearner'S Health Record: Gen. A. Luna ST., Ususan, Taguig CityArianne B. CabañezNo ratings yet
- Cervantes, C.Document48 pagesCervantes, C.LG NiegasNo ratings yet
- SURVEY FORM Back To Back PDFDocument2 pagesSURVEY FORM Back To Back PDFDan Christian BlanceNo ratings yet
- Home Visitation Form: Department of Education Division of General Santos CityDocument1 pageHome Visitation Form: Department of Education Division of General Santos Citymarvin susminaNo ratings yet
- Notification LetterDocument1 pageNotification LetterBonifacio Jr GianganNo ratings yet
- Family Assessment GuideDocument22 pagesFamily Assessment GuideVance ArztNo ratings yet
- 2X2 Latest Picture (With NAMETAG)Document2 pages2X2 Latest Picture (With NAMETAG)Athena ChoNo ratings yet
- Health Declaration Form: Respondent InformationDocument2 pagesHealth Declaration Form: Respondent Informationmyzzle mendarosNo ratings yet
- Guidelines Form Teledentistry 2020Document5 pagesGuidelines Form Teledentistry 2020Fery AnnNo ratings yet
- English q3 Module8Document8 pagesEnglish q3 Module8rhializa78No ratings yet
- Visitor Health Declaration FormDocument2 pagesVisitor Health Declaration FormKaryl Eunice Macabale IboniaNo ratings yet
- Field Study Waiver ConsentDocument1 pageField Study Waiver ConsentMARY ANN CAGATANNo ratings yet
- School MemoDocument2 pagesSchool Memorosario lanzadoNo ratings yet
- Quarter 2 Mps and SDDocument5 pagesQuarter 2 Mps and SDrosario lanzadoNo ratings yet
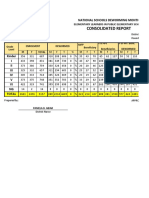
- Consolidated Report: National Schools Deworming MonthDocument74 pagesConsolidated Report: National Schools Deworming Monthrosario lanzadoNo ratings yet
- Parent'S/Guardian'S Consent: Departmentof EducationDocument1 pageParent'S/Guardian'S Consent: Departmentof Educationrosario lanzadoNo ratings yet
- EPP /TLE 6 Second Quarter: MPS: 70.5 SD: 11.43Document5 pagesEPP /TLE 6 Second Quarter: MPS: 70.5 SD: 11.43rosario lanzadoNo ratings yet
- Republic of The Philippine Department of Education Region IX, Zamboanga Peninula Division of Zamboanga Del Sur Dumalinao DistrictDocument2 pagesRepublic of The Philippine Department of Education Region IX, Zamboanga Peninula Division of Zamboanga Del Sur Dumalinao Districtrosario lanzadoNo ratings yet
- Amy Zuckerman David Biederman Exporting Importing How To Buy and Sell Profitably Across Borders AMADocument931 pagesAmy Zuckerman David Biederman Exporting Importing How To Buy and Sell Profitably Across Borders AMATro emaislivrosNo ratings yet
- Final Viewer Guide: Money and Medicine On PBSDocument57 pagesFinal Viewer Guide: Money and Medicine On PBSbponsot100% (10)
- Types and Stages of A Computer VirusDocument12 pagesTypes and Stages of A Computer VirusLeslie PerezNo ratings yet
- Mgt3219e Final ExamDocument5 pagesMgt3219e Final ExampavitthiraNo ratings yet
- Metro Jobs Clearance Form BlankDocument1 pageMetro Jobs Clearance Form BlankTj Daquigan100% (1)
- 204-05-Vehicle Dynamic Suspension 204-05Document8 pages204-05-Vehicle Dynamic Suspension 204-05Tienphat co.,ltdNo ratings yet
- Bahir Dar UniversityDocument43 pagesBahir Dar UniversityFìrœ Lōv MånNo ratings yet
- Strategies of Philippine National PoliceDocument5 pagesStrategies of Philippine National Policemichael angelo cayabyabNo ratings yet
- RC Group Brochure NEXT EVO DX Van DE WIT DatacenterkoelingDocument6 pagesRC Group Brochure NEXT EVO DX Van DE WIT Datacenterkoelingeep saepudinNo ratings yet
- Content Manager: Installation and Upgrade GuideDocument62 pagesContent Manager: Installation and Upgrade Guidedaniel emuzeNo ratings yet
- Microscan MS-3 Laser Scanner: Device Driver User GuideDocument43 pagesMicroscan MS-3 Laser Scanner: Device Driver User GuidePavan Kumar KattimaniNo ratings yet
- Release NoteDocument22 pagesRelease NoteAndi GumelarNo ratings yet
- Icje 4 3 29 34Document6 pagesIcje 4 3 29 34Akira MiyazonoNo ratings yet
- Lawn Mower Research ProposalDocument9 pagesLawn Mower Research ProposalJohn Albert BioNo ratings yet
- Admin CasesDocument35 pagesAdmin CasesAleph JirehNo ratings yet
- Form CM GSV MQP SQP Tgi WcaDocument13 pagesForm CM GSV MQP SQP Tgi WcaHasan NudinNo ratings yet
- Conveyancing Assignment Set 1Document2 pagesConveyancing Assignment Set 1deepak singhal100% (1)
- Jinko Solar Module DatasheetDocument2 pagesJinko Solar Module DatasheetSrishtiBerdeNo ratings yet
- Amlock Leading Non Banking Financial Company Building Society in The UKDocument2 pagesAmlock Leading Non Banking Financial Company Building Society in The UKNguyễn Quốc MạnhNo ratings yet
- Experiment 4. Potential of A Galvanic CellDocument2 pagesExperiment 4. Potential of A Galvanic CellChynna Kaye GregorioNo ratings yet
- Common Base Transistor Configuration (CB) : Savan MehtaDocument3 pagesCommon Base Transistor Configuration (CB) : Savan MehtaAhmad RazaNo ratings yet