You might also like
- Critical Care Study Guide: Text and ReviewFrom EverandCritical Care Study Guide: Text and ReviewGerard J. CrinerNo ratings yet
- Surgical Critical Care Therapy: A Clinically Oriented Practical ApproachFrom EverandSurgical Critical Care Therapy: A Clinically Oriented Practical ApproachAli SalimNo ratings yet
- Clinical Review: Care of The Dying Patient: The Last Hours or Days of LifeDocument5 pagesClinical Review: Care of The Dying Patient: The Last Hours or Days of LifevabcunhaNo ratings yet
- End of Life CareDocument6 pagesEnd of Life CareraraNo ratings yet
- Nurse Involvement in End of Life DecisionDocument4 pagesNurse Involvement in End of Life Decisiontri hardaniNo ratings yet
- End-Of-Life Care in The Pediatric ICU: ReviewDocument5 pagesEnd-Of-Life Care in The Pediatric ICU: ReviewarisNo ratings yet
- It Is Not The Fading Candle That One Expects General Practitioners Perspectives On Life Preserving Versus Letting Go Decision Making in End of LifeDocument14 pagesIt Is Not The Fading Candle That One Expects General Practitioners Perspectives On Life Preserving Versus Letting Go Decision Making in End of LifeHerfanus DuhaNo ratings yet
- EUTHADocument10 pagesEUTHAJena WoodsNo ratings yet
- Circumstances of Death in Hospitalized Patients and Nurses' PerceptionsDocument9 pagesCircumstances of Death in Hospitalized Patients and Nurses' PerceptionsMatthew PackaNo ratings yet
- Pon 3346Document8 pagesPon 3346Laura GilNo ratings yet
- Chochinov 1999Document4 pagesChochinov 1999Thatiana GimenesNo ratings yet
- Resuscitation Decisions at The End of Life: The Final DecisionsDocument3 pagesResuscitation Decisions at The End of Life: The Final DecisionsDaniela DanaNo ratings yet
- Do Not Resuscitate Orders and Ethical Decisions in A Neonatal Intensive Care Unit in A Muslim CommunityDocument5 pagesDo Not Resuscitate Orders and Ethical Decisions in A Neonatal Intensive Care Unit in A Muslim CommunityzakyNo ratings yet
- Attitudes and Views of The General Public Towards Research ParticipationDocument10 pagesAttitudes and Views of The General Public Towards Research ParticipationditeABCNo ratings yet
- Week 13 & 14 - DEATH AND DYINGDocument36 pagesWeek 13 & 14 - DEATH AND DYINGون توNo ratings yet
- Analysis: Palliative Care From Diagnosis To DeathDocument5 pagesAnalysis: Palliative Care From Diagnosis To DeathFernanda FerreiraNo ratings yet
- CC PresentationDocument16 pagesCC Presentationapi-602756847No ratings yet
- AutreDocument6 pagesAutreWijdane El YoumniNo ratings yet
- A Pain-Free' Death: Fiona Hicks and Elizabeth ReesDocument19 pagesA Pain-Free' Death: Fiona Hicks and Elizabeth Reesbdalcin5512No ratings yet
- Loss Qo DyingDocument8 pagesLoss Qo Dyingsiti nurjanahNo ratings yet
- NIH Public Access: Author ManuscriptDocument11 pagesNIH Public Access: Author ManuscriptmartingomezrNo ratings yet
- Patrickqodd1 PDFDocument10 pagesPatrickqodd1 PDFHamza TayyabNo ratings yet
- Pandini Et Al., 2016Document6 pagesPandini Et Al., 2016mackenzie.lacey28No ratings yet
- Johansson2017 Diários Nos ÓbitosDocument8 pagesJohansson2017 Diários Nos ÓbitosGabriela LealNo ratings yet
- A Communication Strategy and Brochure For Relatives of Patients Dying in The ICU - Nejm - Lautrette - 469sa1Document79 pagesA Communication Strategy and Brochure For Relatives of Patients Dying in The ICU - Nejm - Lautrette - 469sa1Manuel PernetasNo ratings yet
- Symptom Clusters in Men and Women With Heart Failure and Their Impact On Cardiac Eventyfree SurvivalDocument10 pagesSymptom Clusters in Men and Women With Heart Failure and Their Impact On Cardiac Eventyfree Survivalabraham rumayaraNo ratings yet
- Chochinov Dignity TherapyDocument6 pagesChochinov Dignity TherapyAdrian FermanelliNo ratings yet
- Chochinov Dignity TherapyDocument6 pagesChochinov Dignity TherapySimona DavidNo ratings yet
- Clinical Exemplar PaperDocument6 pagesClinical Exemplar Paperapi-606157505No ratings yet
- chung2017Document9 pageschung2017drabellollinasNo ratings yet
- Care of The Adult Cancer Patient at The End of Life: ESMO Clinical Practice GuidelinesDocument13 pagesCare of The Adult Cancer Patient at The End of Life: ESMO Clinical Practice GuidelinesDewi SunnnNo ratings yet
- One-Year Outcomes in CaregiversDocument11 pagesOne-Year Outcomes in Caregiversgiovanni311094No ratings yet
- Jurnal PenelitianDocument6 pagesJurnal PenelitianRuli MaulanaNo ratings yet
- Dutch Physicians On The Role of The Family in Continuous SedationDocument5 pagesDutch Physicians On The Role of The Family in Continuous Sedationdiradosta_1992No ratings yet
- What Matters Most For End-Of-Life Care? Perspectives From Community-Based Palliative Care Providers and AdministratorsDocument8 pagesWhat Matters Most For End-Of-Life Care? Perspectives From Community-Based Palliative Care Providers and AdministratorsPutri Tamara DasantosNo ratings yet
- GP-led improvements cut cancer diagnosis timeDocument2 pagesGP-led improvements cut cancer diagnosis timeMj ManuelNo ratings yet
- Fridh 2009Document9 pagesFridh 2009ABIENo ratings yet
- Nursing Diagnoses and Interventions For Cardiological Patients in Palliative Care Original ArticleDocument9 pagesNursing Diagnoses and Interventions For Cardiological Patients in Palliative Care Original ArticleMaginta Resy DianaNo ratings yet
- 13.the Effect of A Comprehensive Dementia Care Management Program On End-of-Life CareDocument6 pages13.the Effect of A Comprehensive Dementia Care Management Program On End-of-Life CareBadRahnaNo ratings yet
- Ebn 2Document8 pagesEbn 2Abadilla LANo ratings yet
- Palliative DocumentDocument21 pagesPalliative DocumentTaikoNo ratings yet
- BMJ c1345 FullDocument9 pagesBMJ c1345 FullJude PanlaanNo ratings yet
- 2013 Sharp ACP Frail OlderDocument12 pages2013 Sharp ACP Frail OlderdrabellollinasNo ratings yet
- Ethics and The Legalization of Physician-Assisted Suicide - An American College of Physicians Position PaperDocument12 pagesEthics and The Legalization of Physician-Assisted Suicide - An American College of Physicians Position PaperRoberto López MataNo ratings yet
- 2014 Development of A Tool For DefiningDocument13 pages2014 Development of A Tool For DefiningSugeng JitowiyonoNo ratings yet
- End-Of-Life Communication in The Intensive Care UnitDocument10 pagesEnd-Of-Life Communication in The Intensive Care UnitAzkiya Ulki FadhillaNo ratings yet
- JCM 10 04900Document14 pagesJCM 10 04900Chistian LassoNo ratings yet
- (Pubmed) Protocolised Approach To End-Of-Life Care in The ICU-the ICU PALCare Pilot ProjectDocument6 pages(Pubmed) Protocolised Approach To End-Of-Life Care in The ICU-the ICU PALCare Pilot ProjectRahmida RahmyNo ratings yet
- Jurnal 3Document9 pagesJurnal 3Edwin Pasha Jr.No ratings yet
- Yamaguchi 2017Document33 pagesYamaguchi 2017Maria FreitasNo ratings yet
- Pengkajian Riwayat Dan Pemeriksaan Fisik Pasian PaliatifDocument7 pagesPengkajian Riwayat Dan Pemeriksaan Fisik Pasian PaliatifnrjNo ratings yet
- InnovativeSolutions FamilyProgressNoteDocument8 pagesInnovativeSolutions FamilyProgressNotem mNo ratings yet
- Bennett 2016Document3 pagesBennett 2016Nabila ChakourNo ratings yet
- Behavioural and Psychiatric Symptoms in People With Dementia Admitted To The Acute Hospital Prospective Cohort StudyDocument8 pagesBehavioural and Psychiatric Symptoms in People With Dementia Admitted To The Acute Hospital Prospective Cohort StudyJosue GarciaNo ratings yet
- Awareness of Medical Orders For Life Sustaining Treatmen - 2016 - Journal of PaiDocument1 pageAwareness of Medical Orders For Life Sustaining Treatmen - 2016 - Journal of PaiDipendra PratapNo ratings yet
- Improved Quality of Death and Dying in Care Homes - A Palliative Care Stepped Wedge Randomized Control Trial in AustraliaDocument8 pagesImproved Quality of Death and Dying in Care Homes - A Palliative Care Stepped Wedge Randomized Control Trial in AustraliacharmyshkuNo ratings yet
- Aged Care (Silver Book) - Part ADocument25 pagesAged Care (Silver Book) - Part AXin gNo ratings yet
- Gero ReportDocument6 pagesGero ReportLen PinedaNo ratings yet
- End-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareDocument5 pagesEnd-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Caring for Patients at the End of Life: Palliative Care and HospiceFrom EverandCaring for Patients at the End of Life: Palliative Care and HospiceNo ratings yet
- Improving Caregivers' Perceptions Regarding Patient Goals of Care/End-of-Life Issues For The Multidisciplinary Critical Care TeamDocument9 pagesImproving Caregivers' Perceptions Regarding Patient Goals of Care/End-of-Life Issues For The Multidisciplinary Critical Care TeamSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Family Meetings at End of Life ReviewDocument10 pagesFamily Meetings at End of Life ReviewSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Improving Attitudes and Perceptions About End-of-Life Nursing On A Hospital-Based Palliative Care UnitDocument8 pagesImproving Attitudes and Perceptions About End-of-Life Nursing On A Hospital-Based Palliative Care UnitSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Experiences of Dying, Death and Bereavement in Motor Neurone Disease: A Qualitative StudyDocument11 pagesExperiences of Dying, Death and Bereavement in Motor Neurone Disease: A Qualitative StudySERGIO ANDRES CESPEDES GUERRERONo ratings yet
- General Nurses' Experiences of End-Of-Life Care in The Acute Hospital Setting: A Literature ReviewDocument7 pagesGeneral Nurses' Experiences of End-Of-Life Care in The Acute Hospital Setting: A Literature ReviewSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- End-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareDocument5 pagesEnd-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Evaluation of A Continuous Quality Improvement Initiative For End-of-Life Care For Older Noncancer PatientsDocument9 pagesEvaluation of A Continuous Quality Improvement Initiative For End-of-Life Care For Older Noncancer PatientsSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Extending Palliative Care To Patients With Parkinson's DiseaseDocument5 pagesExtending Palliative Care To Patients With Parkinson's DiseaseSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Pediatric Palliative CareDocument36 pagesPediatric Palliative CareIndonesian Journal of Cancer100% (1)
- Assessment of Palliative Care ServicesDocument46 pagesAssessment of Palliative Care ServicesOSGFNo ratings yet
- Test Bank 19Document48 pagesTest Bank 19Tala AlaminNo ratings yet
- End of Life Care BrochureDocument2 pagesEnd of Life Care BrochureNoraNo ratings yet
- City University Nursing DissertationDocument4 pagesCity University Nursing DissertationCustomizedWritingPaperSingapore100% (1)
- Guideline For Alzheimer'S Disease Management: Final Report 2008Document122 pagesGuideline For Alzheimer'S Disease Management: Final Report 2008Chaddia MoresNo ratings yet
- Jurnal Internasional 2020 The - RoleDocument5 pagesJurnal Internasional 2020 The - RoleNely Noer SofwatiNo ratings yet
- Ethics and Medico Legal AspectsDocument5 pagesEthics and Medico Legal AspectsmkumNo ratings yet
- Hesr 51 352Document26 pagesHesr 51 352Naja nigricollisNo ratings yet
- From Frustration To Coping With Caring For Death by Nurse TechniciansDocument7 pagesFrom Frustration To Coping With Caring For Death by Nurse TechniciansC. R. PintoNo ratings yet
- Lisa Barrett: N438 Assignment Marking Record For Discussion Paper Instructor: Mark: 58Document10 pagesLisa Barrett: N438 Assignment Marking Record For Discussion Paper Instructor: Mark: 58Assignment &ExamsNo ratings yet
- Module 3 - Death, Dignity and Death With DignityDocument24 pagesModule 3 - Death, Dignity and Death With DignityKatie HolmesNo ratings yet
- Tutorial Assignment Week 14 With AnswerDocument4 pagesTutorial Assignment Week 14 With AnswerCik Wynn100% (1)
- Final EvaluationDocument17 pagesFinal Evaluationapi-603938769No ratings yet
- Jurnal InternasionalDocument4 pagesJurnal InternasionalMuhammad SalehNo ratings yet
- Marcia AngellDocument2 pagesMarcia AngellselvamuthukumarNo ratings yet
- Nursing Home Social Worker Resume ExampleDocument1 pageNursing Home Social Worker Resume ExampleBibin JamesNo ratings yet
- Instant Download Ebook PDF Ethics and Issues in Contemporary Nursing 3rd by Margaret A Burkhardt 2 PDF ScribdDocument41 pagesInstant Download Ebook PDF Ethics and Issues in Contemporary Nursing 3rd by Margaret A Burkhardt 2 PDF Scribddouglas.phillips233100% (41)
- Coa CfuDocument20 pagesCoa CfuZymer Lee AbasoloNo ratings yet
- Nursing Dissertation, Nursing Essay, Nursing Project, Nursing Assignment, Nursing Homework, Nursing Writing, Nursing Outline, Nursing Abstract, Nursing DissertationDocument10 pagesNursing Dissertation, Nursing Essay, Nursing Project, Nursing Assignment, Nursing Homework, Nursing Writing, Nursing Outline, Nursing Abstract, Nursing DissertationiWanttutor.com100% (1)
- TFN Week 13 14Document43 pagesTFN Week 13 14mccaberto1061cabNo ratings yet
- Palliative Care 101Document51 pagesPalliative Care 101Grape JuiceNo ratings yet
- NCM 114 LEC PHARMACODYNAMICS ETHICO-LEGAL CONSIDERATIONSDocument4 pagesNCM 114 LEC PHARMACODYNAMICS ETHICO-LEGAL CONSIDERATIONSChrisnel Caoile0% (1)
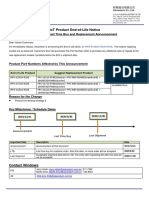
- Product Phase Out Notice IPPC 6152 6172 6192 R2AEDocument1 pageProduct Phase Out Notice IPPC 6152 6172 6192 R2AEguruh anindraNo ratings yet
- Adult CHD Heart Failure Nonpharmacologic TreatmentDocument10 pagesAdult CHD Heart Failure Nonpharmacologic TreatmentAndhika DNo ratings yet
- The Basis, Ethics and Provision of Palliative Care of Dementia - A ReviewDocument5 pagesThe Basis, Ethics and Provision of Palliative Care of Dementia - A ReviewMaria VasquezNo ratings yet
- Music Therapy For End-Of-Life Care (Review)Document36 pagesMusic Therapy For End-Of-Life Care (Review)Andrea BarresiNo ratings yet
- A View of Spirituality and Spiritual Care in A Sample of Spanish NursesDocument12 pagesA View of Spirituality and Spiritual Care in A Sample of Spanish NursesJulia TintingNo ratings yet
- Chapter 36 Death Study GuideDocument25 pagesChapter 36 Death Study GuideDaniel McVayNo ratings yet