You might also like
- Stem Cells in Regenerative Medicine: Carpe Diem – Carpe Vitam!From EverandStem Cells in Regenerative Medicine: Carpe Diem – Carpe Vitam!Rating: 2.5 out of 5 stars2.5/5 (3)
- @anesthesia Books 2016 The Final PDFDocument435 pages@anesthesia Books 2016 The Final PDFMinaz Patel100% (2)
- Manual Equus 810 070Document10 pagesManual Equus 810 070Juan Ramón100% (1)
- DES-3611.prepaway - Premium.exam.65q: Number: DES-3611 Passing Score: 800 Time Limit: 120 Min File Version: 1.1Document22 pagesDES-3611.prepaway - Premium.exam.65q: Number: DES-3611 Passing Score: 800 Time Limit: 120 Min File Version: 1.1Emre Halit POLATNo ratings yet
- Event Management Study Material Free PDFDocument2 pagesEvent Management Study Material Free PDFKim0% (1)
- PDF Post Stroke Scalp Acupuncture DLDocument64 pagesPDF Post Stroke Scalp Acupuncture DLyohan100% (2)
- 20 Lemeur2017 PDFDocument13 pages20 Lemeur2017 PDFHarsya LuthfiNo ratings yet
- Siller 2018Document9 pagesSiller 2018Alin CiubotaruNo ratings yet
- ALS Symptoms, Causes, Prognosis ExplainedDocument14 pagesALS Symptoms, Causes, Prognosis ExplainedJohn SmithNo ratings yet
- Nejme 2400102Document3 pagesNejme 2400102linjingwang912No ratings yet
- DaleBredesen Final AlzheimersDocument42 pagesDaleBredesen Final AlzheimersJohn William Sugden100% (5)
- A Review On Spinal Muscular Atrophy Clinical Classification, Etiology, Diagnosis and TreatmentDocument4 pagesA Review On Spinal Muscular Atrophy Clinical Classification, Etiology, Diagnosis and TreatmentEditor IJTSRDNo ratings yet
- Botulinum Toxin A For Upper Limb SpasticityDocument3 pagesBotulinum Toxin A For Upper Limb SpasticityTerrence ChanNo ratings yet
- ECT in Schizophrenia Need For ReappraisalDocument3 pagesECT in Schizophrenia Need For ReappraisalanettewillNo ratings yet
- Recent Advances in Histopathology 23 (2015) (PDF) (UnitedVRG) PDFDocument192 pagesRecent Advances in Histopathology 23 (2015) (PDF) (UnitedVRG) PDFsargonNo ratings yet
- The Role of Magnetic Resonance Imaging in Acute Transverse MyelitisDocument4 pagesThe Role of Magnetic Resonance Imaging in Acute Transverse MyelitisHồ NguyễnNo ratings yet
- VV 1Document9 pagesVV 1alexiafiguerascNo ratings yet
- En A04v86n4Document10 pagesEn A04v86n4Florentina NastaseNo ratings yet
- Sleep Disruption in Hematopoietic Cell Transplantation Recipients Prevalence Severity and Clinical ManagementDocument20 pagesSleep Disruption in Hematopoietic Cell Transplantation Recipients Prevalence Severity and Clinical ManagementJohn RonquilloNo ratings yet
- AAN 2023 Day 1-2 Mind Next OriginalDocument21 pagesAAN 2023 Day 1-2 Mind Next Originalmpm8471No ratings yet
- Main 70Document7 pagesMain 70pokharelriwaj82No ratings yet
- Case 31 - 2019Document12 pagesCase 31 - 2019Gustavo AngelesNo ratings yet
- Shortness of Breath in A 74-Year-Old WomanDocument5 pagesShortness of Breath in A 74-Year-Old WomanNicole Villanueva, BSN - Level 3ANo ratings yet
- Japanese StudyDocument11 pagesJapanese StudyР. МөнхжинNo ratings yet
- Effect of Blood-letting Puncture on Consciousness in Apoplexy PatientsDocument5 pagesEffect of Blood-letting Puncture on Consciousness in Apoplexy Patientsyushfa baharNo ratings yet
- Caso 2Document10 pagesCaso 2Luanna DávilaNo ratings yet
- Mitochondrial Autism-A Unique Subpopulation and Piece of The Puzzle?Document27 pagesMitochondrial Autism-A Unique Subpopulation and Piece of The Puzzle?autismoneNo ratings yet
- Alzheimer's Disease: Mark N. Levine, M.DDocument2 pagesAlzheimer's Disease: Mark N. Levine, M.Dlala_bojaNo ratings yet
- Cyclosporine A in Reperfused Myocardial Infarction: The Multicenter, Controlled, Open-Label CYCLE TrialDocument1 pageCyclosporine A in Reperfused Myocardial Infarction: The Multicenter, Controlled, Open-Label CYCLE TrialTaniaNo ratings yet
- Neurosciences 26-4-392Document4 pagesNeurosciences 26-4-392esinsubozatliNo ratings yet
- Stem cell therapy for spinal cord repair: a review of the past 10 yearsDocument6 pagesStem cell therapy for spinal cord repair: a review of the past 10 yearsOkhuarobo SamuelNo ratings yet
- Perbedaan Kualitas Hidup Pasien Usia Lanjut Sebelum Dan Setelah Operasi Katarak Adelia Lisnawati, Nur Khoma Fatmawati, Meiliati AminyotoDocument6 pagesPerbedaan Kualitas Hidup Pasien Usia Lanjut Sebelum Dan Setelah Operasi Katarak Adelia Lisnawati, Nur Khoma Fatmawati, Meiliati AminyotoEfrinaldo PardedeNo ratings yet
- Encefalitis LimbicaDocument11 pagesEncefalitis LimbicaRandy UlloaNo ratings yet
- Giant Skull Base Osteoblastoma CaseDocument2 pagesGiant Skull Base Osteoblastoma CaseLarisjoursNo ratings yet
- Cutaneous Sensitivity Changes in Bell's Palsy PatientsDocument6 pagesCutaneous Sensitivity Changes in Bell's Palsy PatientsLuqmanul HakimNo ratings yet
- 2012-European Journal of Neurology IMPRIMIR PAGINA 141Document368 pages2012-European Journal of Neurology IMPRIMIR PAGINA 141Francisco A. Villegas-LópezNo ratings yet
- Act TrialDocument34 pagesAct Trialapi-668691030No ratings yet
- Jurnal Keperawatan-Neti MesriDocument5 pagesJurnal Keperawatan-Neti MesriMuhammad ZahranNo ratings yet
- New Pathways in The Treatment For Menopausal Hot Flushes: CommentDocument3 pagesNew Pathways in The Treatment For Menopausal Hot Flushes: CommentAlifia DamayantiNo ratings yet
- NLR Bells PalsyDocument4 pagesNLR Bells PalsyIskandar HasanNo ratings yet
- Vitamin D Deficiency Linked to Newly Diagnosed Idiopathic Epilepsy in ChildrenDocument5 pagesVitamin D Deficiency Linked to Newly Diagnosed Idiopathic Epilepsy in ChildrenFihzanNo ratings yet
- Paediatric Respiratory Reviews: Ruth Grychtol, Francois Abel, Dominic A. FitzgeraldDocument8 pagesPaediatric Respiratory Reviews: Ruth Grychtol, Francois Abel, Dominic A. FitzgeraldMarina FerreiraNo ratings yet
- Atlas of Neuromuscular DiseasesDocument364 pagesAtlas of Neuromuscular Diseasesandy sotoNo ratings yet
- Dutta Et Al Mitochondrial Dysfunction in MS AnnNeurol06Document12 pagesDutta Et Al Mitochondrial Dysfunction in MS AnnNeurol06WZNo ratings yet
- AA BloodDocument10 pagesAA BloodsilviaNo ratings yet
- MRI and 2D-CSI MR Spectroscopy of The BrainDocument10 pagesMRI and 2D-CSI MR Spectroscopy of The BrainСергей ЛесорубNo ratings yet
- Early Detection Key for SMA TreatmentDocument55 pagesEarly Detection Key for SMA TreatmentSnezana MihajlovicNo ratings yet
- Aringhieri 2018Document92 pagesAringhieri 2018Mariana PestanaNo ratings yet
- Selective Atrophy of Left Hemisphere and Frontal LDocument11 pagesSelective Atrophy of Left Hemisphere and Frontal LPaulNo ratings yet
- Chronic Traumatic Encephalopathy - 2019 - Disease A MonthDocument4 pagesChronic Traumatic Encephalopathy - 2019 - Disease A MonthBruno MañonNo ratings yet
- Sportiche2016 PDFDocument7 pagesSportiche2016 PDFRavi KumarNo ratings yet
- Sport I Che 2016Document7 pagesSport I Che 2016Ravi KumarNo ratings yet
- NRF2 PathwayDocument15 pagesNRF2 PathwayMagnusAngeltveitKjølenNo ratings yet
- I2211 4599 14 5 706Document7 pagesI2211 4599 14 5 706Jasper CubiasNo ratings yet
- JurnalDocument9 pagesJurnalSiscaNo ratings yet
- 2010 Congenital Ataxia, Mental Retardation, and Dyskinesia Associated With A Novel CACNA1A MutationDocument6 pages2010 Congenital Ataxia, Mental Retardation, and Dyskinesia Associated With A Novel CACNA1A MutationJefe de Escuela PsicologiaNo ratings yet
- Journal Club EdavaroneDocument5 pagesJournal Club EdavaroneJohn Christopher RuizNo ratings yet
- 01 WNL 0000042787 51461 d1Document2 pages01 WNL 0000042787 51461 d1veronikiNo ratings yet
- Detection of Cognitive Impairment in Multiple Sclerosis Based On P300 Event-Related PotentialDocument8 pagesDetection of Cognitive Impairment in Multiple Sclerosis Based On P300 Event-Related Potentialzwecker4458No ratings yet
- 972883Document8 pages972883acNo ratings yet
- Yamaguchi 2017Document33 pagesYamaguchi 2017Maria FreitasNo ratings yet
- Improving Attitudes and Perceptions About End-of-Life Nursing On A Hospital-Based Palliative Care UnitDocument8 pagesImproving Attitudes and Perceptions About End-of-Life Nursing On A Hospital-Based Palliative Care UnitSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Improving Caregivers' Perceptions Regarding Patient Goals of Care/End-of-Life Issues For The Multidisciplinary Critical Care TeamDocument9 pagesImproving Caregivers' Perceptions Regarding Patient Goals of Care/End-of-Life Issues For The Multidisciplinary Critical Care TeamSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Family Meetings at End of Life ReviewDocument10 pagesFamily Meetings at End of Life ReviewSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- General Nurses' Experiences of End-Of-Life Care in The Acute Hospital Setting: A Literature ReviewDocument7 pagesGeneral Nurses' Experiences of End-Of-Life Care in The Acute Hospital Setting: A Literature ReviewSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- End-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareDocument5 pagesEnd-Of-Life Care in The Icu: Supporting Nurses To Provide High-Quality CareSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Evaluation of A Continuous Quality Improvement Initiative For End-of-Life Care For Older Noncancer PatientsDocument9 pagesEvaluation of A Continuous Quality Improvement Initiative For End-of-Life Care For Older Noncancer PatientsSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- End of Life Management of Adult Patients in An Australian Metropolitan Intensive Care Unit: A Retrospective Observational StudyDocument7 pagesEnd of Life Management of Adult Patients in An Australian Metropolitan Intensive Care Unit: A Retrospective Observational StudySERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Extending Palliative Care To Patients With Parkinson's DiseaseDocument5 pagesExtending Palliative Care To Patients With Parkinson's DiseaseSERGIO ANDRES CESPEDES GUERRERONo ratings yet
- Land Sale Dispute Interest Rate CaseDocument3 pagesLand Sale Dispute Interest Rate CaseAnne MiguelNo ratings yet
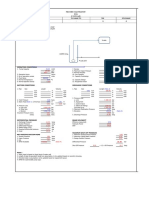
- Pump Sizing SpreadsheetDocument2 pagesPump Sizing Spreadsheetandrew rachmanNo ratings yet
- Solucionario Capitulo 1 Gruber Porque Estudiamos Finanzas PublicasDocument5 pagesSolucionario Capitulo 1 Gruber Porque Estudiamos Finanzas PublicasDemetrio Pardo HerreraNo ratings yet
- Building C# Applications: Unit - 2Document25 pagesBuilding C# Applications: Unit - 2mgsumaNo ratings yet
- Inductive sensor technical specifications in 40 charactersDocument3 pagesInductive sensor technical specifications in 40 charactersBasarNo ratings yet
- College of Industrial Technology Bachelor of Technology and Livelihood Education (TLE) CMO. No. 78, S. 2017Document5 pagesCollege of Industrial Technology Bachelor of Technology and Livelihood Education (TLE) CMO. No. 78, S. 2017Industrial TechnologyNo ratings yet
- As 2669-1983 Sulphuric Acid For Use in Lead-Acid BatteriesDocument7 pagesAs 2669-1983 Sulphuric Acid For Use in Lead-Acid BatteriesSAI Global - APACNo ratings yet
- Lesson 3.3: The Third Wave: The Information/Knowledge AgeDocument3 pagesLesson 3.3: The Third Wave: The Information/Knowledge AgeFaith PrachayaNo ratings yet
- Central Council For Research in Ayurvedic Sciences: CCRAS Post Doctoral Fellowship Scheme (CCRAS PDF Scheme)Document2 pagesCentral Council For Research in Ayurvedic Sciences: CCRAS Post Doctoral Fellowship Scheme (CCRAS PDF Scheme)TUSHAR DASHNo ratings yet
- TABS 6SellSheetDocument4 pagesTABS 6SellSheetHernando MontenegroNo ratings yet
- 2020 Ifs InsuranceDocument262 pages2020 Ifs InsuranceSensi CTPrima100% (1)
- Global CityDocument3 pagesGlobal Citycr lamigoNo ratings yet
- Tata Cellular V UOI: So Unreasonable That No Reasonable Person Acting Reasonably Could Have Made It)Document2 pagesTata Cellular V UOI: So Unreasonable That No Reasonable Person Acting Reasonably Could Have Made It)heretostudyNo ratings yet
- 11 Core CompetenciesDocument11 pages11 Core CompetenciesrlinaoNo ratings yet
- NY B17 ATF FDR - 7-24-03 ATF Email and 10-25-01 ATF After Action Report 092Document20 pagesNY B17 ATF FDR - 7-24-03 ATF Email and 10-25-01 ATF After Action Report 0929/11 Document Archive100% (2)
- RTD Temperature Transmitter Calibration Report TemplateDocument1 pageRTD Temperature Transmitter Calibration Report TemplateSuswantoro ToroNo ratings yet
- CCST+Cybersecurity+Objecitve+Domain Cisco Final wCiscoLogoDocument3 pagesCCST+Cybersecurity+Objecitve+Domain Cisco Final wCiscoLogoQazi ZayadNo ratings yet
- Ansys Workbench Tutorial: Structural & Thermal Analysis Using The ANSYS Workbench Release 11.0 EnvironmentDocument5 pagesAnsys Workbench Tutorial: Structural & Thermal Analysis Using The ANSYS Workbench Release 11.0 EnvironmentMuhammad HaroonNo ratings yet
- Last Minute Reviewer for 2019 Bar ExamDocument19 pagesLast Minute Reviewer for 2019 Bar ExamFrances Ann Teves100% (1)
- Assignment 2Document21 pagesAssignment 2api-445531772No ratings yet
- TUTO 4 PU Sol PDFDocument21 pagesTUTO 4 PU Sol PDFVievie Le BluewberrietrufflesNo ratings yet
- Datasheet of DS 7608NI Q1 - 8P NVRD - V4.71.200 - 20220705Document5 pagesDatasheet of DS 7608NI Q1 - 8P NVRD - V4.71.200 - 20220705Gherel TocasNo ratings yet
- Newnew 151 ModelDocument1 pageNewnew 151 ModelCrestine Lily DongosaNo ratings yet
- Wiz107sr User Manual en v1.0Document29 pagesWiz107sr User Manual en v1.0Pauli Correa ArriagadaNo ratings yet
- Fnce 220: Business Finance: Lecture 6: Capital Investment DecisionsDocument39 pagesFnce 220: Business Finance: Lecture 6: Capital Investment DecisionsVincent KamemiaNo ratings yet
- Sample BudgetDocument109 pagesSample BudgetAnjannette SantosNo ratings yet
- Organophosphorus Pesticide Residues in Vegetables and Soil Samples From Alau Dam and Gongulong Agricultural Areas, Borno State, NigeriaDocument7 pagesOrganophosphorus Pesticide Residues in Vegetables and Soil Samples From Alau Dam and Gongulong Agricultural Areas, Borno State, NigeriaWiro JuangNo ratings yet