You might also like
- Rice Diet Kempner PDFDocument33 pagesRice Diet Kempner PDFDebra100% (4)
- Good Housekeeping - Easy KetoDocument98 pagesGood Housekeeping - Easy KetoStefan HNo ratings yet
- Syndromes Associated With Nutritional Deficiency and ExcessDocument17 pagesSyndromes Associated With Nutritional Deficiency and ExcessBlu Punto ArtNo ratings yet
- Vitamin D PPT Final 1Document53 pagesVitamin D PPT Final 1NisargNo ratings yet
- Dunes Cake KICADocument8 pagesDunes Cake KICARia100% (3)
- Three Oils and The MitochondriaDocument5 pagesThree Oils and The MitochondriaFUAAD HASSANNo ratings yet
- Laboratory Activity No 2 - GLOVA-NDDocument4 pagesLaboratory Activity No 2 - GLOVA-NDandreyou99No ratings yet
- Stand Out 5 Test 4 2019 2020Document8 pagesStand Out 5 Test 4 2019 2020Fatima SilvaNo ratings yet
- 12 Patients Bill of RightsDocument1 page12 Patients Bill of RightsDennis John Villaraza89% (9)
- Grade 9 Lo3Document14 pagesGrade 9 Lo3Joyzann Cellan100% (1)
- InggDocument9 pagesInggCut Sarah FaradillaNo ratings yet
- BITOT'S SPOTS: EVALUATION AND TREATMENT OF VITAMIN A DEFICIENCYDocument2 pagesBITOT'S SPOTS: EVALUATION AND TREATMENT OF VITAMIN A DEFICIENCYEsther EunikeNo ratings yet
- Rickets AafpDocument8 pagesRickets AafpAndrea RivaNo ratings yet
- Deficiencia A D eDocument5 pagesDeficiencia A D eIvan Emerson Huanca AñamuroNo ratings yet
- Hair, Nails, and Skin: Differentiating Cutaneous Manifestations of Micronutrient DeficiencyDocument14 pagesHair, Nails, and Skin: Differentiating Cutaneous Manifestations of Micronutrient DeficiencyIrving EuanNo ratings yet
- 2012 33 339 Bryon Lauer and Nancy Spector: Pediatrics in ReviewDocument16 pages2012 33 339 Bryon Lauer and Nancy Spector: Pediatrics in ReviewFernanda SierraNo ratings yet
- Scurvy in Pediatric Age Group E A Disease Often Forgotten?: SciencedirectDocument7 pagesScurvy in Pediatric Age Group E A Disease Often Forgotten?: SciencedirectDavy JonesNo ratings yet
- ScccvyDocument7 pagesScccvyDavy JonesNo ratings yet
- Rickets and Hypervitaminosis D: Causes, Symptoms and TreatmentDocument11 pagesRickets and Hypervitaminosis D: Causes, Symptoms and TreatmentElvisNo ratings yet
- Atypical Presentation of Cystic Fibrosis in An InfantDocument3 pagesAtypical Presentation of Cystic Fibrosis in An InfantBandya SahooNo ratings yet
- Nutritional Disorders Review - Part 2 - and Primary Immunodeficiency DisordersDocument20 pagesNutritional Disorders Review - Part 2 - and Primary Immunodeficiency DisordersJessica MooreNo ratings yet
- The FASEB Journal - 1996 - Underwood - The Contribution of Vitamin A To Public HealthDocument9 pagesThe FASEB Journal - 1996 - Underwood - The Contribution of Vitamin A To Public HealthCarlos BareaNo ratings yet
- Hidden HungerDocument12 pagesHidden HungerHuzaifa CHNo ratings yet
- PDF 6Document26 pagesPDF 6Ajeng Nur NabillahNo ratings yet
- Skin Manifestations of Nutritional Disorders: November 2019Document11 pagesSkin Manifestations of Nutritional Disorders: November 2019Saadat muneerNo ratings yet
- Nutritional Support Critical for IBD PatientsDocument9 pagesNutritional Support Critical for IBD PatientsJEFFERSON MUÑOZNo ratings yet
- A Narrative Review On Pediatric Scurvy - The Last Twenty YearsDocument12 pagesA Narrative Review On Pediatric Scurvy - The Last Twenty YearsgistaluvikaNo ratings yet
- Transes Pre Final HematologyDocument20 pagesTranses Pre Final HematologyMrdy CaiNo ratings yet
- Deficiencias Doenças CeliacaDocument18 pagesDeficiencias Doenças CeliacaFernanda MoreiraNo ratings yet
- Fat Soluble Vitamin RevisedDocument80 pagesFat Soluble Vitamin RevisedsumitNo ratings yet
- Ateneo School of Medicine and Public Health Nutrition Guide For Clerks SCHOOL YEAR 2019-2020Document12 pagesAteneo School of Medicine and Public Health Nutrition Guide For Clerks SCHOOL YEAR 2019-2020Jeff AguilarNo ratings yet
- A_Rare_Presentation_of_Scurvy_in_a_Well-Nourished_Document4 pagesA_Rare_Presentation_of_Scurvy_in_a_Well-Nourished_nyanta.efuaNo ratings yet
- CHAPTER 63 and 64 Vitamin CDocument41 pagesCHAPTER 63 and 64 Vitamin CJosselle Sempio CalientaNo ratings yet
- Dietary Approaches for Managing Inflammatory Bowel DiseaseDocument10 pagesDietary Approaches for Managing Inflammatory Bowel DiseaseRebeca EspinoNo ratings yet
- Malnutrition and Vaccination in Developing Countries: ReviewDocument8 pagesMalnutrition and Vaccination in Developing Countries: ReviewFerry HartonoNo ratings yet
- B12 Deficency NEJM 2013Document12 pagesB12 Deficency NEJM 2013Aída Fernanda100% (1)
- Benefits of Vitamin B12 and Its Nutritional SourcesDocument2 pagesBenefits of Vitamin B12 and Its Nutritional SourcesasclepiuspdfsNo ratings yet
- Micronutrient Defi Ciency Conditions: Global Health Issues: Public Health Reviews, Vol. 32, No 1, 243-255Document13 pagesMicronutrient Defi Ciency Conditions: Global Health Issues: Public Health Reviews, Vol. 32, No 1, 243-255TariqNo ratings yet
- Peran Vitamin Dalam New Normal Dr. Yoga Devara, SpAKDocument31 pagesPeran Vitamin Dalam New Normal Dr. Yoga Devara, SpAKfadil rulianNo ratings yet
- Treatment of Small Intestine Bacterial Overgrowth: M. Di Stefano, E. Miceli, A. Missanelli, G.R. CorazzaDocument6 pagesTreatment of Small Intestine Bacterial Overgrowth: M. Di Stefano, E. Miceli, A. Missanelli, G.R. CorazzaIgor FerreiraNo ratings yet
- Essentials of Clinical Periodontology and Periodontics 5th Ed (1) - Pages-2Document3 pagesEssentials of Clinical Periodontology and Periodontics 5th Ed (1) - Pages-2Diana AjengNo ratings yet
- Rasmussen Fernhoff Scanlon B12 Deficiencyinchildrenandadolescents JPediatrics 2001Document9 pagesRasmussen Fernhoff Scanlon B12 Deficiencyinchildrenandadolescents JPediatrics 2001Navatha MorthaNo ratings yet
- Nutrition Lecture 4. Protein Energy Malnutrition Edited Caparro Melgar Candido Panganoron Espeso Maceda 3Document8 pagesNutrition Lecture 4. Protein Energy Malnutrition Edited Caparro Melgar Candido Panganoron Espeso Maceda 3Charisse Angelica MacedaNo ratings yet
- ORAL MANIFESTATIONS OF VITAMIN DEFICIENCIESDocument9 pagesORAL MANIFESTATIONS OF VITAMIN DEFICIENCIESKrupali JainNo ratings yet
- Bruising As The First Sign of Exocrine Pancreatic Insufficiency in InfancyDocument5 pagesBruising As The First Sign of Exocrine Pancreatic Insufficiency in InfancyIrina SerpiNo ratings yet
- 4 Infección Neonatal C. DifficileDocument5 pages4 Infección Neonatal C. DifficileLuis Astudillo MedinaNo ratings yet
- Vitamin D DefeciencyDocument6 pagesVitamin D DefeciencyMaryam FadahNo ratings yet
- Nutrients 14 01168Document18 pagesNutrients 14 01168oscarNo ratings yet
- Vitamin A Deficiency Document SummaryDocument42 pagesVitamin A Deficiency Document SummaryGupta JiNo ratings yet
- The Pathophysiology of Elevated Vitamin B12 in Clinical PracticeDocument11 pagesThe Pathophysiology of Elevated Vitamin B12 in Clinical PracticePanagiotis-Sokratis LoumakisNo ratings yet
- Vitamin B12 (Cobalamin) Deficiency in The Older Adult: C. Christine Orton, PHD, FNP-BCDocument7 pagesVitamin B12 (Cobalamin) Deficiency in The Older Adult: C. Christine Orton, PHD, FNP-BCAnis RanisNo ratings yet
- Rare but Devastating Micronutrient Deficiencies in RYGB PatientsDocument10 pagesRare but Devastating Micronutrient Deficiencies in RYGB PatientsYazen JoudehNo ratings yet
- Nutrition and MalocclusionDocument2 pagesNutrition and Malocclusionsrishti jainNo ratings yet
- Malnutrition-Cause and ConsequencesDocument4 pagesMalnutrition-Cause and ConsequencesHusdup NarcisaNo ratings yet
- WebPath - NutritionDocument6 pagesWebPath - NutritiondNo ratings yet
- Fatsolublevitamin Assessmentand SupplementationincholestasisDocument17 pagesFatsolublevitamin Assessmentand Supplementationincholestasisarvinjay solisNo ratings yet
- Jurnal InternasionalDocument8 pagesJurnal InternasionalBrivita PopyNo ratings yet
- A Practical Approach To Diagnose and Treat Rickets: Journal of Clinical Medicine of Kazakhstan (E-ISSN 2313-1519)Document7 pagesA Practical Approach To Diagnose and Treat Rickets: Journal of Clinical Medicine of Kazakhstan (E-ISSN 2313-1519)goppalNo ratings yet
- Vitamin D and Child Health: Part 2 (Extraskeletal and Other Aspects)Document6 pagesVitamin D and Child Health: Part 2 (Extraskeletal and Other Aspects)drsaleemNo ratings yet
- Exam Community & Applied Nutrition IiDocument13 pagesExam Community & Applied Nutrition IiLeslie Ann MesolisNo ratings yet
- Study of Vitamin D Status Among Postmenopausal Women: 10.5005/jp-Journals-10032-1101Document7 pagesStudy of Vitamin D Status Among Postmenopausal Women: 10.5005/jp-Journals-10032-1101Riya RawatNo ratings yet
- Pernicious Anemia Refers To A Lack of Vitamin b12 in The Body That Resulted To An Autoimmune Condition in Which The Body Does Not Produce Intrinsic Factor That Can Be AbsorbedDocument2 pagesPernicious Anemia Refers To A Lack of Vitamin b12 in The Body That Resulted To An Autoimmune Condition in Which The Body Does Not Produce Intrinsic Factor That Can Be AbsorbedJuan Miguel Caspe MangayaNo ratings yet
- Updates on Managing Severe Acute MalnutritionDocument74 pagesUpdates on Managing Severe Acute MalnutritionAbdi KebedeNo ratings yet
- MicronutrientesDocument12 pagesMicronutrientesRoger santa cruz zamoraNo ratings yet
- History and importance of vitamin C in human healthDocument24 pagesHistory and importance of vitamin C in human healthSantiago Jara RodriguezNo ratings yet
- Obesity Medicine: Irina A. Lapik, Alexey V. Galchenko, Kamilat M. Gapparova TDocument9 pagesObesity Medicine: Irina A. Lapik, Alexey V. Galchenko, Kamilat M. Gapparova TMakbule ERÇAKIRNo ratings yet
- PlicationsDocument9 pagesPlicationsMuthu KumarNo ratings yet
- Draft Charter On Rights of Patients in IndiaDocument28 pagesDraft Charter On Rights of Patients in IndiaKranthi ChirumamillaNo ratings yet
- Tamil Nadu Hospital Protection Act, 2008 (In p225-226)Document53 pagesTamil Nadu Hospital Protection Act, 2008 (In p225-226)Dr.Sagindar100% (2)
- A Penile Torsion With A Fistula Due To Previous Hypospadias Surgery: A Case ReportDocument5 pagesA Penile Torsion With A Fistula Due To Previous Hypospadias Surgery: A Case ReportMuthu KumarNo ratings yet
- Guidelines on Paediatric Urology DiseasesDocument14 pagesGuidelines on Paediatric Urology DiseasesEndang Yulia AngrainiNo ratings yet
- Background.: PEDIATRICS Vol. 116 No. 3 September 2005Document10 pagesBackground.: PEDIATRICS Vol. 116 No. 3 September 2005Muthu KumarNo ratings yet
- RappaportL LBTStudy PEC2016Document11 pagesRappaportL LBTStudy PEC2016Muthu KumarNo ratings yet
- Haematology: Complete Blood Cell CountDocument2 pagesHaematology: Complete Blood Cell CountMuthu KumarNo ratings yet
- Wa0040Document12 pagesWa0040Muthu KumarNo ratings yet
- Wa0001Document7 pagesWa0001Muthu KumarNo ratings yet
- BLUE RegulationsNovember2017v01CleanDocument10 pagesBLUE RegulationsNovember2017v01CleanashkeraiNo ratings yet
- Wa0033Document4 pagesWa0033Muthu KumarNo ratings yet
- Draft Charter On Rights of Patients in IndiaDocument28 pagesDraft Charter On Rights of Patients in IndiaKranthi ChirumamillaNo ratings yet
- SM Rehab OatsDocument6 pagesSM Rehab OatsMuthu KumarNo ratings yet
- Wa0041Document2 pagesWa0041Muthu KumarNo ratings yet
- L &itijld: Rj6Itfhj&LoDocument1 pageL &itijld: Rj6Itfhj&LoMuthu KumarNo ratings yet
- CV - Tapan KR GhoshDocument1 pageCV - Tapan KR GhoshMuthu KumarNo ratings yet
- CV - Suhas PrabhuDocument1 pageCV - Suhas PrabhuMuthu KumarNo ratings yet
- PEDIATRIC DRUG CHART FOR EMERGENCY MEDICAL SERVICESDocument6 pagesPEDIATRIC DRUG CHART FOR EMERGENCY MEDICAL SERVICESDimas Bayu FirdausNo ratings yet
- 10th National Conference of Pediatric Infectious Diseases Curriculum VitaeDocument1 page10th National Conference of Pediatric Infectious Diseases Curriculum VitaeMuthu KumarNo ratings yet
- CV - Ranbir Singh LDocument1 pageCV - Ranbir Singh LMuthu KumarNo ratings yet
- 10th National Conference of Pediatric Infectious DiseasesDocument1 page10th National Conference of Pediatric Infectious DiseasesMuthu KumarNo ratings yet
- CV - Deepak UgraDocument1 pageCV - Deepak UgraMuthu KumarNo ratings yet
- CV - Neelam VermaDocument1 pageCV - Neelam VermaMuthu KumarNo ratings yet
- CV - Maiya P PDocument1 pageCV - Maiya P PMuthu Kumar0% (1)
- CV - Deepak UgraDocument1 pageCV - Deepak UgraMuthu KumarNo ratings yet
- CV - Deepak UgraDocument1 pageCV - Deepak UgraMuthu KumarNo ratings yet
- CV - Digant ShastriDocument2 pagesCV - Digant ShastriMuthu Kumar100% (1)
- Formula Feeding Peparation Sheet StudentsDocument5 pagesFormula Feeding Peparation Sheet StudentsYaser ZaherNo ratings yet
- Digestive SystemDocument7 pagesDigestive Systemmuli.michaelNo ratings yet
- IGCSE Coordinated Sciences Animal NutritionDocument10 pagesIGCSE Coordinated Sciences Animal NutritionSeonaid McDonaldNo ratings yet
- Adherence To Iron Folic Acid Supplementation and Associated Factors Among Antenatal CARE Attending Women in Sire District Primary Health Care UnitsDocument8 pagesAdherence To Iron Folic Acid Supplementation and Associated Factors Among Antenatal CARE Attending Women in Sire District Primary Health Care Unitsmeless gebrieNo ratings yet
- Microbiology of Fermented Milk Product Ass Bscag4Document3 pagesMicrobiology of Fermented Milk Product Ass Bscag4Shailesh Singh PatelNo ratings yet
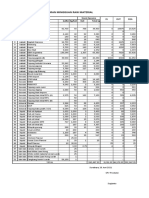
- Laporan Mingguan Raw Material: Stock Opname IN OUT Sisa Jenis Raw Material Buffer Kg/koli Koli Total KGDocument4 pagesLaporan Mingguan Raw Material: Stock Opname IN OUT Sisa Jenis Raw Material Buffer Kg/koli Koli Total KGAlfa ArnantoNo ratings yet
- Food and Nutrition Research Institute (FNRI) Food Guide PyramidDocument28 pagesFood and Nutrition Research Institute (FNRI) Food Guide PyramidWincy SalazarNo ratings yet
- Admin, Journal Manager, 5 - YuliaDocument9 pagesAdmin, Journal Manager, 5 - YuliaRizka syftriNo ratings yet
- Price List 221005 - GeneralDocument6 pagesPrice List 221005 - GeneralRisa BungaNo ratings yet
- Dissertation Topics in Food ScienceDocument7 pagesDissertation Topics in Food ScienceBuyCheapPaperOnlineEugene100% (1)
- Vegemite Triple Decker Sandwich RecipeDocument1 pageVegemite Triple Decker Sandwich RecipeJoedy-Beth Dolom0% (1)
- Antonia-Leda Matalas, Antonis Zampelas, Vassilis Stavrinos - The Mediterranean Diet - Constituents and Health Promotion-CRC Press (2001)Document379 pagesAntonia-Leda Matalas, Antonis Zampelas, Vassilis Stavrinos - The Mediterranean Diet - Constituents and Health Promotion-CRC Press (2001)Новковић АњаNo ratings yet
- Basic English Pronouns, Prepositions and Connectors PracticeDocument3 pagesBasic English Pronouns, Prepositions and Connectors PracticeYo Soy VidelNo ratings yet
- Synthesis of Silver Nanoparticles Using Combination of Beta Vulgaris A Project ReportDocument34 pagesSynthesis of Silver Nanoparticles Using Combination of Beta Vulgaris A Project ReportAshish Naval100% (1)
- The Effect of Replacing Soybean Meal With Fava Bean Seeds in Daily Ration of Lebanese Baladi Goat Kids and Awassi Sheep Lambs: 1 - Body PerformanceDocument14 pagesThe Effect of Replacing Soybean Meal With Fava Bean Seeds in Daily Ration of Lebanese Baladi Goat Kids and Awassi Sheep Lambs: 1 - Body PerformanceMamta AgarwalNo ratings yet
- Vitamins and Their Clinical Applications by Stepp Et Al 1938 German TranslationDocument207 pagesVitamins and Their Clinical Applications by Stepp Et Al 1938 German TranslationLewJr100% (1)
- Special Food ProductsDocument15 pagesSpecial Food ProductsRomnick Tubo100% (1)
- Life Sciences p1 Memo Gr11 Nov 2020 Eng DDocument10 pagesLife Sciences p1 Memo Gr11 Nov 2020 Eng Dmokoenakoketso018No ratings yet
- Safety and Influence of A Novel Powder Form of Coconut Inflorescence Sap On Glycemic Index and LipidDocument1 pageSafety and Influence of A Novel Powder Form of Coconut Inflorescence Sap On Glycemic Index and LipidPriscila CerqueiraNo ratings yet
- Banana starch and flour food applications reviewDocument13 pagesBanana starch and flour food applications reviewZenaw AntenbiyeNo ratings yet
- Milk, Dairy Products, and Their Functional Effects in HumansDocument13 pagesMilk, Dairy Products, and Their Functional Effects in HumansBrayam AlvarezNo ratings yet
- 10 Foods To Eat During ChemotherapyDocument4 pages10 Foods To Eat During ChemotherapyCrissel Kane CarpioNo ratings yet
- State of Childhood Obesity 10 14 20 Final WEB PDFDocument48 pagesState of Childhood Obesity 10 14 20 Final WEB PDFWSETNo ratings yet
- Speaking Vstep Part 1Document7 pagesSpeaking Vstep Part 1lan quynhNo ratings yet