You might also like
- Immo Off FilesDocument6 pagesImmo Off Filesاليزيد بن توهامي100% (1)
- BA JapanesePG PDFDocument7 pagesBA JapanesePG PDFIan IskandarNo ratings yet
- Vdocument - in LRT Design GuidelinesDocument490 pagesVdocument - in LRT Design GuidelinesAlly KhooNo ratings yet
- @MedicalBooksStore Mayo Clinic Body MRI Case Review (2014) PDFDocument881 pages@MedicalBooksStore Mayo Clinic Body MRI Case Review (2014) PDFKahkashan Hameed100% (1)
- Tad2 - Functional Concepts and The Interior EnvironmentDocument10 pagesTad2 - Functional Concepts and The Interior EnvironmentJay Reyes50% (2)
- CH 13 Lecture PresentationDocument97 pagesCH 13 Lecture PresentationDalia M. MohsenNo ratings yet
- Smart AntennasDocument40 pagesSmart AntennasMeeraNo ratings yet
- ALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020Document3 pagesALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020محمد نبيل الدعيس100% (1)
- Ultrasound in Obstet Gyne - 2023 - Prayer - ISUOG Practice Guidelines Updated Performance of Fetal Magnetic ResonanceDocument10 pagesUltrasound in Obstet Gyne - 2023 - Prayer - ISUOG Practice Guidelines Updated Performance of Fetal Magnetic ResonanceAndres Cardenas OsorioNo ratings yet
- Post Fcps Fellowship Options For Radiology Residents: Resident'S SectionDocument4 pagesPost Fcps Fellowship Options For Radiology Residents: Resident'S SectionAkhtar AbbasNo ratings yet
- Kenigsberg 2015Document12 pagesKenigsberg 2015Fernando Silva RivasNo ratings yet
- Morris2012 - Correlation of Dental Maturity With Skeletal Maturity From Radiographic AssessmentDocument6 pagesMorris2012 - Correlation of Dental Maturity With Skeletal Maturity From Radiographic Assessmentcruzjulio480No ratings yet
- Habib y 1995Document4 pagesHabib y 1995adeNo ratings yet
- Disfunctie Perete Pelvin - Articulatii GhidDocument19 pagesDisfunctie Perete Pelvin - Articulatii GhidClaudia MoldovanuNo ratings yet
- Tu of The OrbitDocument12 pagesTu of The OrbitChavdarNo ratings yet
- Forensic Age Estimation - Experience of A General Hospital: Poster No.: Congress: Type: Authors: KeywordsDocument20 pagesForensic Age Estimation - Experience of A General Hospital: Poster No.: Congress: Type: Authors: KeywordsCirnu AlinaNo ratings yet
- Neurophysiological Intraoperative Monitoring in Neurosurgery: Aid or Handicap?Document7 pagesNeurophysiological Intraoperative Monitoring in Neurosurgery: Aid or Handicap?PratyushGarewalNo ratings yet
- Original ArticleDocument13 pagesOriginal ArticleDhaniNo ratings yet
- Monn - 2013 - Trends in Robot-Assisted Laparoscopic Pyeloplasty in Pediatric PatientsDocument6 pagesMonn - 2013 - Trends in Robot-Assisted Laparoscopic Pyeloplasty in Pediatric PatientsAntonio López MolláNo ratings yet
- Incidence of Congenital Malformations in TokyoDocument4 pagesIncidence of Congenital Malformations in TokyoJAMILA SajidNo ratings yet
- Embarazo EctopicoDocument10 pagesEmbarazo EctopicocfsaludNo ratings yet
- Low and High Grade Gliom in MRSDocument8 pagesLow and High Grade Gliom in MRSHuyen NguyenNo ratings yet
- Ultrasound in Obstet Gyne - 2015 - Van Den Bosch - Terms Definitions and Measurements To Describe Sonographic FeaturesDocument15 pagesUltrasound in Obstet Gyne - 2015 - Van Den Bosch - Terms Definitions and Measurements To Describe Sonographic FeaturesGiuliana Cuadros PeñalozaNo ratings yet
- Monitoreo 2012 PDFDocument19 pagesMonitoreo 2012 PDFDiego A. Cuadros TorresNo ratings yet
- Guías ISUOG Ecografía 2011Document11 pagesGuías ISUOG Ecografía 2011Santiago Fabian Novoa SalgadoNo ratings yet
- Prenatal Diagnosis of Fetal Abdominal Cystic Masses: Can MR Change The Outcome?Document10 pagesPrenatal Diagnosis of Fetal Abdominal Cystic Masses: Can MR Change The Outcome?salahzotoNo ratings yet
- MriCS EnglishDocument8 pagesMriCS Englishstefania caselleNo ratings yet
- Anthropometric Profile Evaluation of The Midface in Patients With Cleft Lip and PalateDocument10 pagesAnthropometric Profile Evaluation of The Midface in Patients With Cleft Lip and PalateAndy HongNo ratings yet
- The Global Lung Function Initiative - Dispelling Some Myths of Lung Function Test InterpretationDocument13 pagesThe Global Lung Function Initiative - Dispelling Some Myths of Lung Function Test InterpretationUriel ChavarriaNo ratings yet
- Alsafi ThesisDocument188 pagesAlsafi ThesisEmad AlamriNo ratings yet
- Manganaro 2017Document11 pagesManganaro 2017Raluca HabaNo ratings yet
- Approach To The Patient With Nontoxic Multinodular GoiterDocument11 pagesApproach To The Patient With Nontoxic Multinodular Goitergds ntnNo ratings yet
- High-Resolution Magnetic Resonance Imaging Can Reliably Detect Orbital Tumor Recurrence After Enucleation in Children With RetinoblastomaDocument11 pagesHigh-Resolution Magnetic Resonance Imaging Can Reliably Detect Orbital Tumor Recurrence After Enucleation in Children With RetinoblastomakarimahihdaNo ratings yet
- Short - and Long-Term Effects of The Herbst Appliance On Temporomandibular Joint FunctionDocument13 pagesShort - and Long-Term Effects of The Herbst Appliance On Temporomandibular Joint FunctionSushma Rayal SANo ratings yet
- Lorenz2009 Article Wide-fieldDigitalImagingBasedTDocument12 pagesLorenz2009 Article Wide-fieldDigitalImagingBasedTtecim3No ratings yet
- Advances in Integrative Medicine: Anne M. Jensen, Richard J. Stevens, Amanda J. BurlsDocument10 pagesAdvances in Integrative Medicine: Anne M. Jensen, Richard J. Stevens, Amanda J. BurlsmoiNo ratings yet
- Teeth Enamel Fullness Involving Maxillary Canines Examined Together With Microcomputed Tomography Scanskmntq PDFDocument1 pageTeeth Enamel Fullness Involving Maxillary Canines Examined Together With Microcomputed Tomography Scanskmntq PDFtaiwanangora83No ratings yet
- Ewing's Sarcoma Review ArticleDocument9 pagesEwing's Sarcoma Review ArticleSayan DasNo ratings yet
- Electronic Fetal MonitoringFrom EverandElectronic Fetal MonitoringXiaohui GuoNo ratings yet
- Multiple Myeloma - Cancer of The Bone Marrow (Blood Tests)Document16 pagesMultiple Myeloma - Cancer of The Bone Marrow (Blood Tests)Jawad AnsariNo ratings yet
- Deep LearningDocument6 pagesDeep Learningragou100% (1)
- Characteristics and Causes of Visual Impairment and Use of Low Vision Devices in Tertiary Hospital in IndonesiaDocument10 pagesCharacteristics and Causes of Visual Impairment and Use of Low Vision Devices in Tertiary Hospital in IndonesiaDenny EmiliusNo ratings yet
- Natural History and Outcome of Optic Pathway Gliomas in ChildrenDocument7 pagesNatural History and Outcome of Optic Pathway Gliomas in ChildrenCamilo Benavides BurbanoNo ratings yet
- Systematic Review of Firsttrimester Ultrasound Screening For Detection of Fetal Structural Anomalies and Factors Affecting Screening PerformanceDocument14 pagesSystematic Review of Firsttrimester Ultrasound Screening For Detection of Fetal Structural Anomalies and Factors Affecting Screening PerformanceMariana B.No ratings yet
- Skeletal Maturity Indicators: Suchita Madhukar Tarvade (Daokar), Sheetal RamkrishnaDocument4 pagesSkeletal Maturity Indicators: Suchita Madhukar Tarvade (Daokar), Sheetal RamkrishnaGina HyginusNo ratings yet
- GUias de Practica Clinica de Ecografias de 2do TrimestreDocument11 pagesGUias de Practica Clinica de Ecografias de 2do TrimestreRodrigo BenitezNo ratings yet
- 50 Patients With OsteosarcomaDocument9 pages50 Patients With Osteosarcomarizaldy achmad kNo ratings yet
- Petuvp PDFDocument6 pagesPetuvp PDFluxmansrikanthaNo ratings yet
- 10.1515 - JPM 2015 0226Document10 pages10.1515 - JPM 2015 0226priyankafetalmedicineNo ratings yet
- Tumor de AbrikossoffDocument5 pagesTumor de AbrikossoffCirugía LarcadeNo ratings yet
- MRI for Radiotherapy: Planning, Delivery, and Response AssessmentFrom EverandMRI for Radiotherapy: Planning, Delivery, and Response AssessmentNo ratings yet
- Large Language Model (LLM) - Driven Chatbots For Neuro-Ophthalmic Medical EducationDocument3 pagesLarge Language Model (LLM) - Driven Chatbots For Neuro-Ophthalmic Medical EducationaliceNo ratings yet
- Fatty LiverDocument8 pagesFatty LiverSyaza Ecom TradingNo ratings yet
- SMFM Clinical Practice GuidelinesDocument8 pagesSMFM Clinical Practice GuidelinesJuanNo ratings yet
- 02 27058Document10 pages02 27058Gina HyginusNo ratings yet
- RO-ILS Case StudyDocument4 pagesRO-ILS Case Studyapi-458422967No ratings yet
- Endophthalmitis in Clinical Practice: Second EditionDocument235 pagesEndophthalmitis in Clinical Practice: Second Editionเทพนิมิตร สมภักดีNo ratings yet
- Bertolotto2020 Article UltrasoundEvaluationOfVaricoceDocument21 pagesBertolotto2020 Article UltrasoundEvaluationOfVaricoceAdietz satyaNo ratings yet
- Developmental Milestones in Type I Spinal Muscular 2016 Neuromuscular DisorDocument6 pagesDevelopmental Milestones in Type I Spinal Muscular 2016 Neuromuscular DisorBaronKornNo ratings yet
- Yamamoto2014 PDFDocument5 pagesYamamoto2014 PDFMunawarahNo ratings yet
- APJCP Volume 17 Issue 9 Pages 4335-4340Document6 pagesAPJCP Volume 17 Issue 9 Pages 4335-4340putriNo ratings yet
- MRI Criteria For The Diagnosis of Pleomorphic Adenoma: A Validation StudyDocument6 pagesMRI Criteria For The Diagnosis of Pleomorphic Adenoma: A Validation Studysarah iriamanaNo ratings yet
- Intrapartum Fetal Monitoring: R. EUGENE BAILEY, MD, SUNY Upstate Medical University, Syracuse, New YorkDocument9 pagesIntrapartum Fetal Monitoring: R. EUGENE BAILEY, MD, SUNY Upstate Medical University, Syracuse, New YorkOana CristinaNo ratings yet
- Amasya-Validation of Cervical Vertebral Maturation Stages Artificial Intelligence Vs Human Observer Visual AnalysisDocument7 pagesAmasya-Validation of Cervical Vertebral Maturation Stages Artificial Intelligence Vs Human Observer Visual AnalysisCatherine NocuaNo ratings yet
- Manejo de HemangiomasDocument11 pagesManejo de HemangiomasDra. Bianca Fabiola Zambrana BarrancosNo ratings yet
- Pediatri RabdomyosarkomDocument7 pagesPediatri RabdomyosarkomDogukan DemirNo ratings yet
- Us-Conversion CycleDocument3 pagesUs-Conversion CycleThessaloe B. FernandezNo ratings yet
- Active & PASSIVE VOICE GRADE 8Document5 pagesActive & PASSIVE VOICE GRADE 8fathima sarahNo ratings yet
- Chinese Journal of Chemistry, 31 (1), 15-17 (2013) - DrospirenoneDocument3 pagesChinese Journal of Chemistry, 31 (1), 15-17 (2013) - DrospirenoneSam SonNo ratings yet
- K01299 - 20211018160945 - SBF3043 Chapter 3 - Digestive SystemDocument52 pagesK01299 - 20211018160945 - SBF3043 Chapter 3 - Digestive SystemChimChim UrkNo ratings yet
- CM (1921) Monthly Test-1 - Off LineDocument20 pagesCM (1921) Monthly Test-1 - Off Linemehul pantNo ratings yet
- Smart Manufacturing For The Oil Refining and Petrochemical IndustryDocument4 pagesSmart Manufacturing For The Oil Refining and Petrochemical IndustryMd Sultan AhemadNo ratings yet
- I. Objectives: Write The LC Code For EachDocument3 pagesI. Objectives: Write The LC Code For EachNica Joy AlcantaraNo ratings yet
- 2-Dimensional CCD Is Built In. A New Type of Displacement Sensor Utilizing The Best and Most Up-To-Date Image Processing TechnologiesDocument13 pages2-Dimensional CCD Is Built In. A New Type of Displacement Sensor Utilizing The Best and Most Up-To-Date Image Processing TechnologiesNguyễn Đức LợiNo ratings yet
- Foxconn G43M01 PDFDocument41 pagesFoxconn G43M01 PDFEduinMaracuchoFernandezChaparroNo ratings yet
- Personalized Implants Restore Smiles - EDRMedesoDocument7 pagesPersonalized Implants Restore Smiles - EDRMedesovivekanandNo ratings yet
- By: DR Evita Febriyanti Fast Track - Dual Degree 2016 Brawijaya UniversityDocument12 pagesBy: DR Evita Febriyanti Fast Track - Dual Degree 2016 Brawijaya UniversityEvitaFebriyantiPNo ratings yet
- CTR201Document2 pagesCTR201Vicente RezabalaNo ratings yet
- Paul Quennon HaikusDocument155 pagesPaul Quennon HaikusDiogo MizaelNo ratings yet
- Critec Transient Discriminating MOVTEC: FeaturesDocument2 pagesCritec Transient Discriminating MOVTEC: Featuresphu pham quocNo ratings yet
- Kratos Pitch Deck PresentationDocument14 pagesKratos Pitch Deck PresentationCS-B Dhanya Lakshmi GNo ratings yet
- Identifying, Understanding, and Analyzing: by Steven M. Rinaldi, James P. Peerenboom, and Terrence K. KellyDocument15 pagesIdentifying, Understanding, and Analyzing: by Steven M. Rinaldi, James P. Peerenboom, and Terrence K. KellySFC JGDNo ratings yet
- Dinah HWDocument6 pagesDinah HWDinah AquinoNo ratings yet
- Class6 Assignment10 2022-23Document29 pagesClass6 Assignment10 2022-23Debaprasad MukherjeeNo ratings yet
- HW 7Document3 pagesHW 7Khuram MaqsoodNo ratings yet
- Vol - CXXV-No .184Document44 pagesVol - CXXV-No .184Sonu DeogunNo ratings yet
- Study On Solar Irrigation System in BangladeshDocument61 pagesStudy On Solar Irrigation System in Bangladeshavocadocolor100% (2)
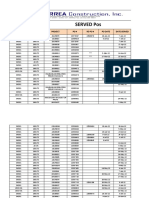
- Served POsDocument21 pagesServed POsYay DumaliNo ratings yet
- D4562-13 Avionics Service Parts Manual 74 and On 150 172 177Document365 pagesD4562-13 Avionics Service Parts Manual 74 and On 150 172 177Brian BlosserNo ratings yet
- Wind PumpDocument6 pagesWind PumpCarlos Castillo PalmaNo ratings yet