You might also like
- Mind Power SecretsDocument38 pagesMind Power SecretsIan Faian92% (52)
- Beeswax Craft RecipesDocument19 pagesBeeswax Craft RecipesCpetrean100% (3)
- Mcqs of Family LawDocument24 pagesMcqs of Family LawVenugopal Mantraratnam32% (19)
- Barbecue Sauce HomadeDocument22 pagesBarbecue Sauce HomadeLiza NasrNo ratings yet
- Royal Enfield Crusader Engine RebuildDocument11 pagesRoyal Enfield Crusader Engine Rebuildbill_wattNo ratings yet
- Prenatal Development (Child Psychology)Document37 pagesPrenatal Development (Child Psychology)Yel BaldemorNo ratings yet
- Embryogenesis (Week 4-8) & Fetal Period (Week 9-Birth)Document30 pagesEmbryogenesis (Week 4-8) & Fetal Period (Week 9-Birth)مالك مناصرةNo ratings yet
- Washing Machine Service ManualDocument67 pagesWashing Machine Service ManualMalay K Ghosh100% (2)
- Fetal DevelopmentDocument51 pagesFetal DevelopmentLhiet Aguilar Hipolito50% (2)
- VR-ForM-F06.10 (Hot Work Permit Request Form)Document1 pageVR-ForM-F06.10 (Hot Work Permit Request Form)imtz2013No ratings yet
- Development of FaceDocument121 pagesDevelopment of FaceArun Shalini SinghNo ratings yet
- IELTS Speaking Topics Jan-Apr 2019Document191 pagesIELTS Speaking Topics Jan-Apr 2019Frenchyard80% (163)
- Service - Manual - CLASSIC 500 - 350 PDFDocument229 pagesService - Manual - CLASSIC 500 - 350 PDFsandystays100% (1)
- Service - Manual - CLASSIC 500 - 350 PDFDocument229 pagesService - Manual - CLASSIC 500 - 350 PDFsandystays100% (1)
- Development of FetusDocument12 pagesDevelopment of FetusmOHAN.SNo ratings yet
- Organogenesis HighlightsDocument99 pagesOrganogenesis HighlightsTimmyNo ratings yet
- Ibsen in PracticeDocument17 pagesIbsen in PracticevictorkalkaNo ratings yet
- Foldings of Embryo Foetal Period 1Document22 pagesFoldings of Embryo Foetal Period 1Riya SinghNo ratings yet
- Prenatal Development and Birth AutosavedDocument74 pagesPrenatal Development and Birth AutosavedEuvanie Bualan RusteNo ratings yet
- Bullet Classic EfiDocument220 pagesBullet Classic EfiGS MeenaNo ratings yet
- BD 1050 PartesDocument26 pagesBD 1050 PartesFelipe RojasNo ratings yet
- Growth and Development of Cranial and Facial RegionDocument81 pagesGrowth and Development of Cranial and Facial RegionSwati PawarNo ratings yet
- UCE Service ManualDocument220 pagesUCE Service ManualAmitabhSaxena100% (1)
- Handling Silica in Cooling WaterDocument17 pagesHandling Silica in Cooling WaterLekhamani YadavNo ratings yet
- Effects of Cutting Classes For Grade 11 TEC Students of AMA Computer College Las PiñasDocument5 pagesEffects of Cutting Classes For Grade 11 TEC Students of AMA Computer College Las PiñasGgssNo ratings yet
- Prenatal GrowthDocument56 pagesPrenatal GrowthnavjotsinghjassalNo ratings yet
- Nitrogen BlanketingDocument21 pagesNitrogen Blanketingrvkumar61No ratings yet
- Embryology of EARDocument43 pagesEmbryology of EARdharmendra kirarNo ratings yet
- Pregnancy and Fetal Development: Shumaila Rani Nursing Instructor (SNC)Document95 pagesPregnancy and Fetal Development: Shumaila Rani Nursing Instructor (SNC)sadia ahmadNo ratings yet
- Embryology, Yolk Sac - StatPearls - NCBI BookshelfDocument10 pagesEmbryology, Yolk Sac - StatPearls - NCBI Bookshelfr9fch8mws7No ratings yet
- Lab Exercise 2Document4 pagesLab Exercise 2Angela Robles0% (1)
- Laporan Nbss ...Document88 pagesLaporan Nbss ...Nita AndriyaniNo ratings yet
- The 55 Hour Chick EmbryoDocument6 pagesThe 55 Hour Chick EmbryoAndrei AlvaradoNo ratings yet
- Prenatal Development and Birth: Prepared by Ms. Sana AslamDocument12 pagesPrenatal Development and Birth: Prepared by Ms. Sana AslamAmatul MusawarNo ratings yet
- Embryology ObgDocument36 pagesEmbryology ObgsamrusangaliNo ratings yet
- Embryology of Genital System & Congenital Anomalies: Kenbon S. (MS) January 30,2021Document56 pagesEmbryology of Genital System & Congenital Anomalies: Kenbon S. (MS) January 30,2021gimNo ratings yet
- Embryological Development of The Human BrainDocument17 pagesEmbryological Development of The Human BrainErika LmNo ratings yet
- Embryology of the Anus and Rectum DevelopmentDocument7 pagesEmbryology of the Anus and Rectum DevelopmentKity PurryNo ratings yet
- Sofie R Krisnadi, Dr. SpogDocument82 pagesSofie R Krisnadi, Dr. SpogYogi OktiandiNo ratings yet
- Embryology of Ear & Temporal BoneDocument37 pagesEmbryology of Ear & Temporal BonefitsumalemayehudNo ratings yet
- Maji Jose - Essentials of Oral Biology - 2nd EditionDocument598 pagesMaji Jose - Essentials of Oral Biology - 2nd EditionRavi RajNo ratings yet
- EmbryogenesisDocument9 pagesEmbryogenesisSanchita SabatNo ratings yet
- Prenatalandpostnatalgrowthofmandible 140127014116 Phpapp02Document26 pagesPrenatalandpostnatalgrowthofmandible 140127014116 Phpapp02HAMIDNo ratings yet
- Department of Orthodontics: Made By: Shayoni Sen Bds Ivthyear Roll No: 23Document26 pagesDepartment of Orthodontics: Made By: Shayoni Sen Bds Ivthyear Roll No: 23HAMIDNo ratings yet
- Vi Semester B. SC Zoology Practicals Study of Embryological Slides Frog BlastulaDocument11 pagesVi Semester B. SC Zoology Practicals Study of Embryological Slides Frog BlastulaSuchitra SharmaNo ratings yet
- Prenatal Growth of Head and Face: Presented by Amritha. Vasudevan First Year PG Department of OrthodonticsDocument50 pagesPrenatal Growth of Head and Face: Presented by Amritha. Vasudevan First Year PG Department of OrthodonticsReenaChauhanNo ratings yet
- Development of Face &it's Applied AspectsDocument95 pagesDevelopment of Face &it's Applied AspectsHansa KunduNo ratings yet
- Ana 209Document15 pagesAna 209ADELAJA SAMUELNo ratings yet
- 4 Development of The EarDocument38 pages4 Development of The EarBryan AtasNo ratings yet
- Embryonic Folding MBBS - 1stDocument30 pagesEmbryonic Folding MBBS - 1stSubham YadavNo ratings yet
- Biophysical Aspects of PregnancyDocument34 pagesBiophysical Aspects of PregnancyRucrispi VirayoNo ratings yet
- Enlarged Vestibular AqueductDocument86 pagesEnlarged Vestibular AqueductGhada WageihNo ratings yet
- Development of The EarDocument16 pagesDevelopment of The Earnapoleon tesfayeNo ratings yet
- DEVELOPMENT OF THE EARDocument33 pagesDEVELOPMENT OF THE EARMuskan IsmailNo ratings yet
- Head and Neck. Embryology. Topographic RegionsDocument56 pagesHead and Neck. Embryology. Topographic RegionsXerox medNo ratings yet
- ANA TOMI Vestibular 2004 0414Document4 pagesANA TOMI Vestibular 2004 0414Nazwa AlhadarNo ratings yet
- The Prenatal Development.. PPT PresentationDocument38 pagesThe Prenatal Development.. PPT PresentationalexandravisteriaNo ratings yet
- 2dev of MaxillaDocument78 pages2dev of MaxillapriyaNo ratings yet
- Growth 1Document10 pagesGrowth 1ng7gmh578qNo ratings yet
- Development of Face and Oral Cavity 05042014Document47 pagesDevelopment of Face and Oral Cavity 05042014Jamal NaimNo ratings yet
- Embryonic Developmental Stages of A Chick EmbryoDocument16 pagesEmbryonic Developmental Stages of A Chick EmbryosugarxglossNo ratings yet
- Embryology Notes emDocument32 pagesEmbryology Notes emSavita HanamsagarNo ratings yet
- Prenatal DevelopmentDocument23 pagesPrenatal Developmentmooncrescent908006No ratings yet
- Development of Vertebra, Ribs and Skull 2007Document16 pagesDevelopment of Vertebra, Ribs and Skull 2007Qaiser InayatNo ratings yet
- 06 Stages of Brain DevelopmentDocument14 pages06 Stages of Brain DevelopmentGeminiah Eve RockerNo ratings yet
- Basic Body Plan of Young Mammalian EmbryosDocument57 pagesBasic Body Plan of Young Mammalian EmbryosWin DierNo ratings yet
- Mandible - Development and GrowthDocument58 pagesMandible - Development and GrowthAinaaMasturaNo ratings yet
- Organogenetic PeriodDocument32 pagesOrganogenetic PeriodAuza Moses IbrahimNo ratings yet
- Estimating Gestational Age in Forensic MedicineDocument23 pagesEstimating Gestational Age in Forensic MedicineRoman Mamun100% (1)
- Development of The Learners at Various Stage: Submitted byDocument22 pagesDevelopment of The Learners at Various Stage: Submitted byArly Boy TadumanNo ratings yet
- Human Embryo DevelopmentDocument14 pagesHuman Embryo DevelopmentSpidyNo ratings yet
- Prenatal and Post Natal Growth of MandibleDocument5 pagesPrenatal and Post Natal Growth of MandiblehabeebNo ratings yet
- Embryology of EarDocument32 pagesEmbryology of EarAnsuman SahuNo ratings yet
- Gastrulation - Week Three of Development: Dr. BarasaDocument37 pagesGastrulation - Week Three of Development: Dr. BarasaGrace NdutaNo ratings yet
- Development of The Male Reproductive System PDFDocument6 pagesDevelopment of The Male Reproductive System PDFJacel JacelNo ratings yet
- Genetic kidney disorder Alport syndrome explainedDocument4 pagesGenetic kidney disorder Alport syndrome explainedvipinNo ratings yet
- Genetic Approach ToDocument15 pagesGenetic Approach TovipinNo ratings yet
- Patterns of Genetic Transmission & Hereditary Hearing Loss: DR - DivyaDocument60 pagesPatterns of Genetic Transmission & Hereditary Hearing Loss: DR - DivyavipinNo ratings yet
- Equal Opportunities Monitoring FormDocument1 pageEqual Opportunities Monitoring FormvipinNo ratings yet
- Endoscopicmanagement Ofcom&tympanoplastyDocument9 pagesEndoscopicmanagement Ofcom&tympanoplastyvipinNo ratings yet
- Xray ViewsDocument81 pagesXray ViewsvipinNo ratings yet
- Features General Description: High Efficiency 1.2Mhz 2A Step Up ConverterDocument7 pagesFeatures General Description: High Efficiency 1.2Mhz 2A Step Up ConvertertugazonaNo ratings yet
- Head & Neck Manifestations of Ra, SleDocument43 pagesHead & Neck Manifestations of Ra, SlevipinNo ratings yet
- Outcomes ResearchDocument15 pagesOutcomes ResearchvipinNo ratings yet
- 100 PDFDocument104 pages100 PDFvipinNo ratings yet
- Lacrimal Apparatus Anatomy & InvestigationsDocument60 pagesLacrimal Apparatus Anatomy & InvestigationsvipinNo ratings yet
- Surgical Anatomy of Nose & PNSDocument33 pagesSurgical Anatomy of Nose & PNSvipinNo ratings yet
- PDF of COMPLETE BOOKDocument81 pagesPDF of COMPLETE BOOKvipinNo ratings yet
- LTC8205ADocument8 pagesLTC8205AChispi LoudenNo ratings yet
- Bluetooth Module Data SheetDocument21 pagesBluetooth Module Data SheetvipinNo ratings yet
- Low-voltage N-channel power MOSFETDocument3 pagesLow-voltage N-channel power MOSFETvipinNo ratings yet
- 1000 PSC QuestionsDocument8 pages1000 PSC QuestionsmonuhfNo ratings yet
- Current Affairs Ebook 2016Document56 pagesCurrent Affairs Ebook 2016anjanaNo ratings yet
- Multi Functional Printer: User's GuideDocument97 pagesMulti Functional Printer: User's GuidevipinNo ratings yet
- SCX 4200 (Service)Document145 pagesSCX 4200 (Service)Christian FrançaNo ratings yet
- Royal Endfield UCE Fuel Injection ManualDocument13 pagesRoyal Endfield UCE Fuel Injection ManualLuis GamboaNo ratings yet
- Integrated CircuitsDocument204 pagesIntegrated CircuitsvipinNo ratings yet
- Ventilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)Document15 pagesVentilation System Comparison - Constant Air Volume (CAV) and Variable Air Volume (VAV)ankurNo ratings yet
- Listing of Equipment For Network DesignDocument3 pagesListing of Equipment For Network DesignJake D La MadridNo ratings yet
- APC Symmetra PX-2Document8 pagesAPC Symmetra PX-2drastir_777No ratings yet
- Product Overview: NCV71208: Octal Solenoid Current Controller With N-FET PredriversDocument1 pageProduct Overview: NCV71208: Octal Solenoid Current Controller With N-FET PredriversDimitar PetrovNo ratings yet
- RMO NO. 66-2016 - DigestDocument2 pagesRMO NO. 66-2016 - DigestJuliannaMendozaMaleNo ratings yet
- Denawaka GangaDocument9 pagesDenawaka GangaErandikaNo ratings yet
- GP2A25J0000F Series: Detecting Distance: 1 To 9mm OPIC Output, Refl Ective Photointerrupter With ConnectorDocument10 pagesGP2A25J0000F Series: Detecting Distance: 1 To 9mm OPIC Output, Refl Ective Photointerrupter With Connectoralias_johndeere2301No ratings yet
- Manual Book IOG ConventionDocument17 pagesManual Book IOG ConventionTaufiq MaulanaNo ratings yet
- AU440-36V-MH: DimensionsDocument2 pagesAU440-36V-MH: DimensionsJohnny FucahoriNo ratings yet
- Beginning Algebra 9th Edition Tobey Solutions Manual 1Document39 pagesBeginning Algebra 9th Edition Tobey Solutions Manual 1kyle100% (30)
- The Federal Environmental Protection Authority: May 2004 Addis Ababa EthiopiaDocument44 pagesThe Federal Environmental Protection Authority: May 2004 Addis Ababa Ethiopiayared0% (1)
- Riel Comun Fstguide2Document2 pagesRiel Comun Fstguide2Rosita TejedaNo ratings yet
- NeseritideDocument28 pagesNeseritideNavojit Chowdhury100% (1)
- Facilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaDocument64 pagesFacilitating Civic Engagement Through Consultation: Learning From Local Communities Through The NHI-Accountability Project in South AfricaOxfamNo ratings yet
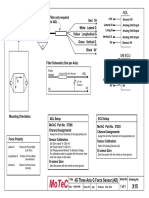
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Midterm Exam Reviewer: Surgical Handwashing QuizDocument9 pagesMidterm Exam Reviewer: Surgical Handwashing QuizOfficially RandomNo ratings yet
- From Sodomy To Safety? The Case For Defining Persecution To Include Unenforced Criminalisation of Same-Sex ConductDocument17 pagesFrom Sodomy To Safety? The Case For Defining Persecution To Include Unenforced Criminalisation of Same-Sex ConductLGBT Asylum NewsNo ratings yet
- Uganda National Urban ProfileDocument74 pagesUganda National Urban ProfileUnited Nations Human Settlements Programme (UN-HABITAT)No ratings yet
- The Suitcase ProjectDocument27 pagesThe Suitcase Projectshubhamkumar9211No ratings yet
- Help to Buy ISA GuideDocument4 pagesHelp to Buy ISA GuidefsdesdsNo ratings yet