You might also like
- Assessment Cover Sheet: BSB52415 Diploma of Marketing and Communication Student NameDocument11 pagesAssessment Cover Sheet: BSB52415 Diploma of Marketing and Communication Student NameChun Jiang0% (1)
- The Historical Foundations of Law. Harold BermanDocument13 pagesThe Historical Foundations of Law. Harold BermanespinasdorsalesNo ratings yet
- Assignments - 2017 09 15 182103 - PDFDocument49 pagesAssignments - 2017 09 15 182103 - PDFMena AlzahawyNo ratings yet
- Clinical Applications of Intraoral Scanning in Removable Prosthodontics: A Literature ReviewDocument16 pagesClinical Applications of Intraoral Scanning in Removable Prosthodontics: A Literature ReviewSantiago ParedesNo ratings yet
- Guided Surgery in Dental ImplantologyDocument5 pagesGuided Surgery in Dental Implantologynarendra singhNo ratings yet
- Digitalized ProsthodonticsDocument3 pagesDigitalized ProsthodonticsSg100% (1)
- Comparison of Different Impression Techniques ForDocument8 pagesComparison of Different Impression Techniques ForQabas MustafaNo ratings yet
- Comparison of The Clinical Accuracy of DDocument9 pagesComparison of The Clinical Accuracy of DDoctor JackNo ratings yet
- Comparison of Digital and Conventional Impressions Based on the 3D Fit of CrownsDocument9 pagesComparison of Digital and Conventional Impressions Based on the 3D Fit of CrownsMathias SchottNo ratings yet
- PatintspecificmotionDocument8 pagesPatintspecificmotionchorv0No ratings yet
- Optical Impressions Dental Carbajal MejiaDocument8 pagesOptical Impressions Dental Carbajal MejiajcNo ratings yet
- 1 s2.0 S002239131630600X MainDocument8 pages1 s2.0 S002239131630600X Mainangi trujilloNo ratings yet
- CJDR 2019 01 s0021Document8 pagesCJDR 2019 01 s0021Faisal hayatNo ratings yet
- Digital WorkflowsDocument14 pagesDigital Workflowsmoji_puiNo ratings yet
- Recent Advances in Dental Optics - Part I: 3D Intraoral Scanners For Restorative DentistryDocument20 pagesRecent Advances in Dental Optics - Part I: 3D Intraoral Scanners For Restorative DentistryCristobalVeraNo ratings yet
- CAD CAM Altered CastDocument6 pagesCAD CAM Altered CastnoneoneoneNo ratings yet
- Uso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaDocument7 pagesUso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaPaola Alexandra LaguadoNo ratings yet
- Digital Technology in Implant Dentistry: Journal of Dentistry & Oral DisordersDocument3 pagesDigital Technology in Implant Dentistry: Journal of Dentistry & Oral DisordersSkAliHassanNo ratings yet
- Alejandro Lanis Full Mouth Oral Rehabilitation of ADocument13 pagesAlejandro Lanis Full Mouth Oral Rehabilitation of AAARON DIAZ RONQUILLONo ratings yet
- Digital Work Flow of Custom AbutmentDocument10 pagesDigital Work Flow of Custom AbutmentmustafaNo ratings yet
- 265-Article Text-1516-2-10-20200110 PDFDocument5 pages265-Article Text-1516-2-10-20200110 PDFmarwaNo ratings yet
- Comparison of the Accuracy of Optical Impression Systems in Three Different Clinical SituationsDocument8 pagesComparison of the Accuracy of Optical Impression Systems in Three Different Clinical SituationsMathias SchottNo ratings yet
- Joda 2016Document6 pagesJoda 2016Juan MusanNo ratings yet
- Transforming Pediatric Dentistry With Digital TechDocument4 pagesTransforming Pediatric Dentistry With Digital TechswayampradeepmohapatraNo ratings yet
- DIGITAL DENTISTRY & OverviewDocument37 pagesDIGITAL DENTISTRY & Overviewrupak biswas67% (3)
- Intraoral Scanning To Fabricate Complete Dentures With Functional Borders: A Proof-Of-Concept Case ReportDocument7 pagesIntraoral Scanning To Fabricate Complete Dentures With Functional Borders: A Proof-Of-Concept Case ReportVeronica Regina RosselleNo ratings yet
- Current TrendsDocument14 pagesCurrent TrendsEsper SorianoNo ratings yet
- 3D Printed Coping for Dental Restoration EvaluationDocument5 pages3D Printed Coping for Dental Restoration EvaluationAriz Habiiballah AstsaqiifNo ratings yet
- 1 s2.0 S1991790220301495 MainDocument6 pages1 s2.0 S1991790220301495 MainMarielEsmeraldaNo ratings yet
- Computerized Casts For Orthodontic Purpose Using Powder-Free Intraoral Scanners - Accuracy, Execution Time, and Patient FeedbackDocument8 pagesComputerized Casts For Orthodontic Purpose Using Powder-Free Intraoral Scanners - Accuracy, Execution Time, and Patient FeedbackCassiana SilvaNo ratings yet
- Clinical Evaluation Comparing The Fit of PDFDocument8 pagesClinical Evaluation Comparing The Fit of PDFScribeNo ratings yet
- Digital Impression 2022Document23 pagesDigital Impression 2022AseelNo ratings yet
- Intraoral ScannersDocument22 pagesIntraoral Scannersheena malikNo ratings yet
- Digital Dentures A Protocol Based On Intraoral SCDocument6 pagesDigital Dentures A Protocol Based On Intraoral SCirfan dNo ratings yet
- Conventional Vs Digital Impression Technique For Manufacturing of Three-Unit Zirconia Bridges: Clinical Time EfficiencyDocument7 pagesConventional Vs Digital Impression Technique For Manufacturing of Three-Unit Zirconia Bridges: Clinical Time EfficiencyAron FotocopyNo ratings yet
- Using Intraoral Scanning To Fabricate Complete Dentures: First ExperiencesDocument5 pagesUsing Intraoral Scanning To Fabricate Complete Dentures: First ExperiencesgermanpuigNo ratings yet
- In Vivo Aging-Induced Surface Roughness Alterations of Invisalign and 3d-Printed AlignersDocument9 pagesIn Vivo Aging-Induced Surface Roughness Alterations of Invisalign and 3d-Printed AlignerslekomundoNo ratings yet
- Digi Tal Technologies Fo R Restorative DentistryDocument24 pagesDigi Tal Technologies Fo R Restorative Dentistrydaniela vallejosNo ratings yet
- Custom Fabrication of Try-In Wax Complete DentureDocument5 pagesCustom Fabrication of Try-In Wax Complete DentureAruna WijayaNo ratings yet
- I Tero Article As PublishedDocument10 pagesI Tero Article As PublishedAldrinNo ratings yet
- Buap 6Document11 pagesBuap 6WawawaNo ratings yet
- Rehabilitación de Un Paciente Con Esclerodermia Con Microstomía Grave Mediante Métodos Digitales y ConvencionalesDocument8 pagesRehabilitación de Un Paciente Con Esclerodermia Con Microstomía Grave Mediante Métodos Digitales y ConvencionalescinthiaNo ratings yet
- Digital Impressions - Paving Path Towards Green Dentistry: A ReviewDocument8 pagesDigital Impressions - Paving Path Towards Green Dentistry: A ReviewIJAR JOURNALNo ratings yet
- Thermocycling Effect On Implant Supported Overdenture Using 3D Printed Peek Bar Following All-On-4 Concept: Randomized Trial-In Vitro StudyDocument16 pagesThermocycling Effect On Implant Supported Overdenture Using 3D Printed Peek Bar Following All-On-4 Concept: Randomized Trial-In Vitro StudyAliaa Wameedh Ramzi AL-OmariNo ratings yet
- UntitledDocument28 pagesUntitledJuan MusanNo ratings yet
- 3D Workflows in Orthodontics Maxillofacial Surgery and ProsthodonticsDocument182 pages3D Workflows in Orthodontics Maxillofacial Surgery and ProsthodonticsA ANo ratings yet
- A Clinician's Guide To Modern Removable Workflows and MaterialsDocument12 pagesA Clinician's Guide To Modern Removable Workflows and MaterialsYun De LinNo ratings yet
- Virtual Evaluation For CAD-CAM-fabricated Complete DenturesDocument6 pagesVirtual Evaluation For CAD-CAM-fabricated Complete DenturesDanny Eduardo RomeroNo ratings yet
- Sensors: /CAM Digital Impressions With Fferent Intraoral Scanner ParametersDocument9 pagesSensors: /CAM Digital Impressions With Fferent Intraoral Scanner ParametersbuccalNo ratings yet
- 10.1007_s40496-017-0145-zDocument9 pages10.1007_s40496-017-0145-zwaf51No ratings yet
- EPA Consensus Project Paper Accuracy of Photogrammetry Devices Intraoral Scanners and Conventional Techniques For The Full Arch Implant Impressions A Systematic ReviewDocument12 pagesEPA Consensus Project Paper Accuracy of Photogrammetry Devices Intraoral Scanners and Conventional Techniques For The Full Arch Implant Impressions A Systematic Reviewcasto.carpetasmiaNo ratings yet
- Gan2018.PdfComparison of Adaptation BetweenDocument9 pagesGan2018.PdfComparison of Adaptation BetweendentureNo ratings yet
- C.E. Credit. Effect of Steam Sterilization on Accuracy of 3D Printed Implant Surgical Guides A Pilot StudyDocument7 pagesC.E. Credit. Effect of Steam Sterilization on Accuracy of 3D Printed Implant Surgical Guides A Pilot Studymarcela fajardoNo ratings yet
- Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical StudiesDocument10 pagesAccuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical StudiesÁł ÃăNo ratings yet
- Intraoral ScannerDocument6 pagesIntraoral ScannerBelanwahidNo ratings yet
- Intraoral Scanner: An Innovative Precision Digital Impression TechnologyDocument12 pagesIntraoral Scanner: An Innovative Precision Digital Impression TechnologySushmaNo ratings yet
- 10 1016@j Ajodo 2019 12 013Document9 pages10 1016@j Ajodo 2019 12 013Ana Maria TamayoNo ratings yet
- Wajib BacaDocument9 pagesWajib BacabuccalNo ratings yet
- Inhouse Aligners-A Review ArticleDocument6 pagesInhouse Aligners-A Review ArticleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Digital Versus Conventional Impressions in Fixed Prosthodontics: A ReviewDocument7 pagesDigital Versus Conventional Impressions in Fixed Prosthodontics: A Reviewruthy arias anahuaNo ratings yet
- EBD Nature Journal-Clinical Outcomes of Implant Supported-2023Document8 pagesEBD Nature Journal-Clinical Outcomes of Implant Supported-2023NARESHNo ratings yet
- Digitization in Dentistry: Clinical ApplicationsFrom EverandDigitization in Dentistry: Clinical ApplicationsPriyanka JainNo ratings yet
- Guided EndodonticsFrom EverandGuided EndodonticsNiraj KinariwalaNo ratings yet
- Service ManualDocument84 pagesService ManualSmart Dental ClinicsNo ratings yet
- Adhesor Carbofine (Liquid) : Safety Data SheetDocument6 pagesAdhesor Carbofine (Liquid) : Safety Data SheetSmart Dental ClinicsNo ratings yet
- Merchant activity report summaryDocument1 pageMerchant activity report summarySmart Dental ClinicsNo ratings yet
- Cuda Compiler Driver NVCC: Reference GuideDocument43 pagesCuda Compiler Driver NVCC: Reference GuideSmart Dental ClinicsNo ratings yet
- International Journal of Scientific Research: Dental ScienceDocument2 pagesInternational Journal of Scientific Research: Dental ScienceSmart Dental ClinicsNo ratings yet
- Preparationofdentalphosphate Bondedinvestment2Document8 pagesPreparationofdentalphosphate Bondedinvestment2Smart Dental ClinicsNo ratings yet
- Ultra Mini Cciq Ii Color Camera Manual: PC RequirementsDocument1 pageUltra Mini Cciq Ii Color Camera Manual: PC RequirementsSmart Dental ClinicsNo ratings yet
- SEPARATING FLUID SDSDocument7 pagesSEPARATING FLUID SDSSmart Dental ClinicsNo ratings yet
- Dental Safety Data SheetDocument6 pagesDental Safety Data SheetSmart Dental ClinicsNo ratings yet
- Merchant activity report summaryDocument1 pageMerchant activity report summarySmart Dental ClinicsNo ratings yet
- Hi-545 Product FlyerDocument2 pagesHi-545 Product FlyerSmart Dental ClinicsNo ratings yet
- Merchant activity report summaryDocument1 pageMerchant activity report summarySmart Dental ClinicsNo ratings yet
- Mobile Assisted Language Learning (MALL) Describes An Approach To Language LearningDocument7 pagesMobile Assisted Language Learning (MALL) Describes An Approach To Language Learninggusria ningsihNo ratings yet
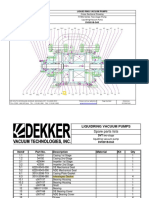
- Bomba de Vacio Part ListDocument2 pagesBomba de Vacio Part ListNayeli Zarate MNo ratings yet
- CBSE Class 10 Science Revision Notes Chapter - 2 Acids, Bases and SaltsDocument11 pagesCBSE Class 10 Science Revision Notes Chapter - 2 Acids, Bases and Saltsmilind dhamaniyaNo ratings yet
- MMC Fiori Cheat Sheet PDFDocument2 pagesMMC Fiori Cheat Sheet PDFAleksandar KNo ratings yet
- PDA Technical Documents on Sterilization ProcessesDocument3 pagesPDA Technical Documents on Sterilization ProcessesManas MishraNo ratings yet
- F 83179Document6 pagesF 83179pcmfilhoNo ratings yet
- Leaving Cert Maths ScholarshipsDocument3 pagesLeaving Cert Maths ScholarshipsJohn HayesNo ratings yet
- Analysis On Forgery Patterns For GPS Civil Spoofing SignalsDocument4 pagesAnalysis On Forgery Patterns For GPS Civil Spoofing SignalsMadhu KrishnaNo ratings yet
- Asc2104b-T I enDocument21 pagesAsc2104b-T I enELOUNDOU EVARISTE OHANDJANo ratings yet
- Advanced Guide To Digital MarketingDocument43 pagesAdvanced Guide To Digital MarketingArpan KarNo ratings yet
- Labconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualDocument77 pagesLabconco-3905503 Rev e Purifier Hepa Filtered and Class I Filtered Enclosures User ManualCalixto GrajalesNo ratings yet
- S7 - Q2 - Answer KeyDocument11 pagesS7 - Q2 - Answer KeyRaniel LacuarinNo ratings yet
- The Impact of Spiritual Intelligence, Gender and Educational Background On Mental Health Among College StudentsDocument22 pagesThe Impact of Spiritual Intelligence, Gender and Educational Background On Mental Health Among College StudentsBabar MairajNo ratings yet
- LUMIX G Camera DMC-G85HDocument9 pagesLUMIX G Camera DMC-G85HnimodisNo ratings yet
- Combining Singing and PsycologyDocument6 pagesCombining Singing and PsycologyAna luciaNo ratings yet
- BCG ReportDocument9 pagesBCG Reportjlgjlj ljglkhNo ratings yet
- Articulos 2022-2Document11 pagesArticulos 2022-2Nilser Enrique Valle HernandezNo ratings yet
- Sony STR Da80esDocument66 pagesSony STR Da80estelstarservicesNo ratings yet
- Living Together TestDocument2 pagesLiving Together TestProfu' de biologieNo ratings yet
- Computer Organization and Assembly Language: Lecture 1 - Basic ConceptsDocument13 pagesComputer Organization and Assembly Language: Lecture 1 - Basic ConceptsNosreffejDelRosarioNo ratings yet
- LAWO PI - MADI - SRC - enDocument2 pagesLAWO PI - MADI - SRC - enfjavierpoloNo ratings yet
- G.raju Reddy Resume (PDF1) PDFDocument3 pagesG.raju Reddy Resume (PDF1) PDFanon_708469687No ratings yet
- Pruebas de Certificación Lingüística in - B1 - Ce - Sol - J - 2015 Answer Key - JUNE 2015 Task 1Document2 pagesPruebas de Certificación Lingüística in - B1 - Ce - Sol - J - 2015 Answer Key - JUNE 2015 Task 1Jeru SierraNo ratings yet
- 1161 Article+Text 5225 1 4 20220712Document9 pages1161 Article+Text 5225 1 4 20220712Warman FatraNo ratings yet
- Course Code Part Sem Paper Code Paper NameDocument3 pagesCourse Code Part Sem Paper Code Paper Nameshiv mishraNo ratings yet
- Master in Public Management: Application PacketDocument6 pagesMaster in Public Management: Application PacketMark GironNo ratings yet
- Bharathidasan University UG/PG Exam ApplicationDocument2 pagesBharathidasan University UG/PG Exam ApplicationOppili yappanNo ratings yet