You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- McKenzie Mechanical Syndromes Coincide With Biopsychosocial InfluencesDocument14 pagesMcKenzie Mechanical Syndromes Coincide With Biopsychosocial InfluencesTomáš KrajíčekNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- PE066 Treatment of Calf Pain in Runners HandoutDocument3 pagesPE066 Treatment of Calf Pain in Runners HandoutTomáš KrajíčekNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- PE067 Handout Shoulder Special Tests and The Rotator Cuff With DR Chris LittlewoodDocument5 pagesPE067 Handout Shoulder Special Tests and The Rotator Cuff With DR Chris LittlewoodTomáš KrajíčekNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Tendinopathy Rehabilitation - PhysiopediaDocument11 pagesTendinopathy Rehabilitation - PhysiopediaTomáš KrajíčekNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- PE064 Calf Pain in Runners HandoutDocument3 pagesPE064 Calf Pain in Runners HandoutTomáš KrajíčekNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
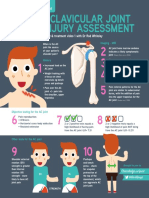
- AC Joint InfographicDocument1 pageAC Joint InfographicTomáš KrajíčekNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- PE 065 InfographicDocument1 pagePE 065 InfographicTomáš KrajíčekNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 08 Reliability and ValidityDocument2 pages08 Reliability and ValidityTomáš KrajíčekNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- 1 PE 067 InfographicDocument1 page1 PE 067 InfographicTomáš KrajíčekNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Ef Cacy of Systematic Active Conservative Treatment For Patients With Severe SciaticaDocument12 pagesThe Ef Cacy of Systematic Active Conservative Treatment For Patients With Severe SciaticaTomáš KrajíčekNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Construct Validity of Lumbar Extension Measures in Mckenzie'S Derangement SyndromeDocument7 pagesConstruct Validity of Lumbar Extension Measures in Mckenzie'S Derangement SyndromeTomáš KrajíčekNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Interpreting Outcomes 3 - Clinical Meaningfulness: Linking Evidence To PracticeDocument2 pagesInterpreting Outcomes 3 - Clinical Meaningfulness: Linking Evidence To PracticeTomáš KrajíčekNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Confidence Intervals: Linking Evidence To PracticeDocument2 pagesConfidence Intervals: Linking Evidence To PracticeTomáš KrajíčekNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Generalizability: Linking Evidence To PracticeDocument2 pagesGeneralizability: Linking Evidence To PracticeTomáš KrajíčekNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 07 Fundamentals of MeasurementDocument2 pages07 Fundamentals of MeasurementTomáš KrajíčekNo ratings yet
- Control Groups: Linking Evidence To PracticeDocument2 pagesControl Groups: Linking Evidence To PracticeTomáš KrajíčekNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Blinding: Linking Evidence To PracticeDocument2 pagesBlinding: Linking Evidence To PracticeTomáš KrajíčekNo ratings yet
- Randomization: Linking Evidence To PracticeDocument2 pagesRandomization: Linking Evidence To PracticeTomáš KrajíčekNo ratings yet
- Engaging With Research: Linking Evidence With PracticeDocument2 pagesEngaging With Research: Linking Evidence With PracticeTomáš KrajíčekNo ratings yet
- Bias: Linking Evidence With PracticeDocument2 pagesBias: Linking Evidence With PracticeTomáš KrajíčekNo ratings yet
- Gufoni Maneuver: Horizontal Canal BPPVDocument19 pagesGufoni Maneuver: Horizontal Canal BPPVTomáš KrajíčekNo ratings yet
- Social Impact Wheel: Community EmpowermentDocument1 pageSocial Impact Wheel: Community EmpowermentDe LanchasNo ratings yet
- IjdaDocument5 pagesIjdaSyed NooraniNo ratings yet
- Module 1 Short Quiz - Classifying BlocksDocument2 pagesModule 1 Short Quiz - Classifying BlocksClaire GargaritaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Societal Security and Crisis Management by Per Lægreid, Lise H. RykkjaDocument398 pagesSocietal Security and Crisis Management by Per Lægreid, Lise H. Rykkjasabar odahNo ratings yet
- JurisprudenceDocument9 pagesJurisprudencealta graceNo ratings yet
- PR 3Document23 pagesPR 3Jaylanie MabagaNo ratings yet
- 22954017: Clinical Practice Guidelines For Hypothyroidism in Adults Cosponsored by The American Association of Clinical Endocrinologists and The American Thyroid AssociationDocument54 pages22954017: Clinical Practice Guidelines For Hypothyroidism in Adults Cosponsored by The American Association of Clinical Endocrinologists and The American Thyroid AssociationUpendra PoudelNo ratings yet
- MBCT PresentationDocument55 pagesMBCT Presentationapi-548853432No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Narayan Hrudalaya Case Study AnalysisDocument5 pagesNarayan Hrudalaya Case Study Analysisdarshak kansagraNo ratings yet
- Installation, Operation, and Maintenance ManualDocument24 pagesInstallation, Operation, and Maintenance ManualrkssNo ratings yet
- The United Nations and Global HealthDocument26 pagesThe United Nations and Global HealthIoan VoicuNo ratings yet
- Interview QuestionsDocument2 pagesInterview QuestionsTriyanti LupikartikaNo ratings yet
- Korean Journal For Food Science of Animal ResourcesDocument8 pagesKorean Journal For Food Science of Animal ResourcesJelena RadivojevicNo ratings yet
- INTERVIEW PREPARATION (Nursing) 2Document5 pagesINTERVIEW PREPARATION (Nursing) 2Safeer SefiNo ratings yet
- Global Food SecurityDocument14 pagesGlobal Food Securityfordastudy angpersonNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 마녀의+도시 10Document45 pages마녀의+도시 10sebNo ratings yet
- Effects of Unemployment To Displaced Workers in Moalboal Cebu, PhilippinesDocument9 pagesEffects of Unemployment To Displaced Workers in Moalboal Cebu, PhilippinesPsychology and Education: A Multidisciplinary JournalNo ratings yet
- UTS g7Document15 pagesUTS g7John Emerson MerelosNo ratings yet
- Speech & Language Therapy in Practice, Autumn 2007Document32 pagesSpeech & Language Therapy in Practice, Autumn 2007Speech & Language Therapy in PracticeNo ratings yet
- Ethio Tahini PLC Business PlanDocument18 pagesEthio Tahini PLC Business PlanTekta MideksaNo ratings yet
- AbstractDocument17 pagesAbstractRukmani 1011No ratings yet
- Bahasa InggrisDocument6 pagesBahasa InggrisafifNo ratings yet
- The Importance of School Volunteering and Social WorkDocument11 pagesThe Importance of School Volunteering and Social Workბარბარე ოდიკაძეNo ratings yet
- Group 7 (GIT & Hepatobiliary Case Simulation)Document41 pagesGroup 7 (GIT & Hepatobiliary Case Simulation)Zil Kamleshkumar PanchalNo ratings yet
- Literary TheoriesDocument25 pagesLiterary TheoriesAriel ChenNo ratings yet
- Articulo Asimetria Facial (05-08)Document4 pagesArticulo Asimetria Facial (05-08)CATALINA VASQUEZ LOPEZNo ratings yet
- Training and Development Program Design & Proposal: In-Service Training For Teachers 2020Document5 pagesTraining and Development Program Design & Proposal: In-Service Training For Teachers 2020Precious Idiosolo100% (1)
- Classroom Activity 3cDocument2 pagesClassroom Activity 3cAgo FunesNo ratings yet
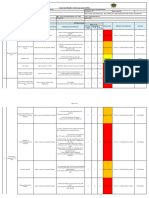
- HIRA3Document14 pagesHIRA3Gyanendra Narayan NayakNo ratings yet
- Oet 2.0 Listening Task 2: Listening Sub-Test Listening Sub-TestDocument7 pagesOet 2.0 Listening Task 2: Listening Sub-Test Listening Sub-TestKrishna Ramas-MaddiNo ratings yet
- The Bridesmaid: The addictive psychological thriller that everyone is talking aboutFrom EverandThe Bridesmaid: The addictive psychological thriller that everyone is talking aboutRating: 4 out of 5 stars4/5 (132)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1460)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)