You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Friction VS Frictionless MechanicsDocument195 pagesFriction VS Frictionless MechanicsDayal Sharan100% (5)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Top Fiber-Rich Foods ListDocument8 pagesThe Top Fiber-Rich Foods ListSabina Alic100% (1)
- Alveolar Bone GraftingDocument13 pagesAlveolar Bone GraftingDayal SharanNo ratings yet
- Seminar Canine Impaction: Dr. Shubham Sharan Post-Graduate Student Department of Orthodontics &dentofacialorthopaedicsDocument24 pagesSeminar Canine Impaction: Dr. Shubham Sharan Post-Graduate Student Department of Orthodontics &dentofacialorthopaedicsDayal SharanNo ratings yet
- Rite Up PDFDocument66 pagesRite Up PDFDayal SharanNo ratings yet
- Seminar Friction Vs Frictionless MechanicsDocument64 pagesSeminar Friction Vs Frictionless MechanicsDayal SharanNo ratings yet
- Dental SurveyorDocument133 pagesDental SurveyorDayal Sharan100% (1)
- Muscle Re-Education: BY DR - Eswar Kolli, MPTDocument42 pagesMuscle Re-Education: BY DR - Eswar Kolli, MPTShubha DiwakarNo ratings yet
- Chapter 1 3 GHWDocument40 pagesChapter 1 3 GHWDINO DIZONNo ratings yet
- Training/Workshop Report (TWR) : L&D Activity Title / Initiated & Conducted by Date/s VenueDocument2 pagesTraining/Workshop Report (TWR) : L&D Activity Title / Initiated & Conducted by Date/s VenueAna Carla de CastroNo ratings yet
- Jurnal UPN Bina Widya OlivDocument17 pagesJurnal UPN Bina Widya OlivoliviafabitaNo ratings yet
- Proprioceptive Neuromuscular Facilitation (PNF) Exercise After Acl ReconstructionDocument22 pagesProprioceptive Neuromuscular Facilitation (PNF) Exercise After Acl ReconstructionMukhlis SiahaanNo ratings yet
- Safeguarding Level 1 Booklet (2019)Document24 pagesSafeguarding Level 1 Booklet (2019)MubeenRahmanNo ratings yet
- 01 - Fitoterapi - D3 SMT VDocument17 pages01 - Fitoterapi - D3 SMT VMaman SuharmanNo ratings yet
- Automatic Hand Sanitizer DispenserDocument19 pagesAutomatic Hand Sanitizer Dispenserhamed razaNo ratings yet
- Carburetor Cleaner-MSDSDocument9 pagesCarburetor Cleaner-MSDSJONATHAN CASTRONo ratings yet
- Heart Rate Variability: - Dattaraj - Sansgiri - 10-548 - Raghav. Narasimhan - 11-501 - JUI - AGAM - 11-502Document27 pagesHeart Rate Variability: - Dattaraj - Sansgiri - 10-548 - Raghav. Narasimhan - 11-501 - JUI - AGAM - 11-502cloantafNo ratings yet
- Pest Control Protocol For Hospital and Related CentersDocument8 pagesPest Control Protocol For Hospital and Related CentersScribdTranslationsNo ratings yet
- Mapeh 7 (Health) - Week 5 - May 29 - June 2, 2023Document5 pagesMapeh 7 (Health) - Week 5 - May 29 - June 2, 2023Michaela LugtuNo ratings yet
- Eapp Module Weeks 3 4Document20 pagesEapp Module Weeks 3 4KaiNo ratings yet
- Lymphatic Rescue Summit 2022 Day 1Document4 pagesLymphatic Rescue Summit 2022 Day 1Paul Ioan PopescuNo ratings yet
- LearnEnglish Listening B1 at The ChemistDocument4 pagesLearnEnglish Listening B1 at The ChemistThai Nhut Hao B2000544No ratings yet
- TTEC Gasparillo RA1Document14 pagesTTEC Gasparillo RA1Geml TrinidadNo ratings yet
- d1 QuestionsDocument6 pagesd1 QuestionsaruNo ratings yet
- Urinary Tract InfectionDocument2 pagesUrinary Tract InfectionAnonymous KillerNo ratings yet
- Research MonggoDocument11 pagesResearch MonggoJed Esperidion Solivio Jumilla50% (2)
- DIASS - Q1 - Mod1 - The Applied Social Sciences and The Discipline of CounselingDocument23 pagesDIASS - Q1 - Mod1 - The Applied Social Sciences and The Discipline of CounselingLindesol Soliva100% (1)
- HOOKWORMDocument30 pagesHOOKWORMALBINUS AmbroseNo ratings yet
- Hazard Identification and Control: An Introduction To Identifying, Analyzing and Controlling Hazards in The WorkplaceDocument41 pagesHazard Identification and Control: An Introduction To Identifying, Analyzing and Controlling Hazards in The WorkplaceRASHEED YUSUF100% (1)
- Extension Services and Mobile UnitsDocument27 pagesExtension Services and Mobile UnitsNaveen Kumar100% (2)
- The Diagnosis and Treatment Dyspesia FuncionalDocument12 pagesThe Diagnosis and Treatment Dyspesia FuncionalpaulNo ratings yet
- 5108e GuideDocument1 page5108e GuideCory McCooeyeNo ratings yet
- Shryti Save DelhiDocument13 pagesShryti Save DelhiShruti KumariNo ratings yet
- 【Entry Form】 ASEAN-Japan Students Conference.xlsx - Sheet1Document2 pages【Entry Form】 ASEAN-Japan Students Conference.xlsx - Sheet1Mizter'Lar IntavanhNo ratings yet
- Teacher Rubric For Warm-Up Task: CommentsDocument1 pageTeacher Rubric For Warm-Up Task: CommentsC MorzahtNo ratings yet
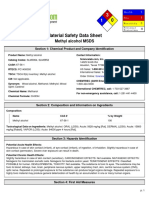
- Methyl Alcohol MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesMethyl Alcohol MSDS: Section 1: Chemical Product and Company IdentificationIriantisabdaNo ratings yet