You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Basics of Karate PDFDocument50 pagesBasics of Karate PDFc_nicu7558170% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Dressing BedsoreDocument66 pagesDressing BedsoreGirish Waru100% (1)
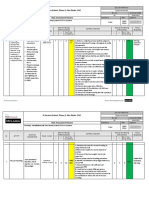
- Risk Assessment For Installation of Fire Alarm System & PAVA SystemDocument11 pagesRisk Assessment For Installation of Fire Alarm System & PAVA SystemAnandu Ashokan88% (8)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Skeletal System Lesson 4Document40 pagesSkeletal System Lesson 4Ella Nika FangonNo ratings yet
- Upper and Lower Limb Clinical Notes (Snell)Document12 pagesUpper and Lower Limb Clinical Notes (Snell)Martin Clyde100% (1)
- Toe and Foot ConditionsDocument14 pagesToe and Foot ConditionsNur InsyirahNo ratings yet
- Acute Intestinal ObstructionDocument50 pagesAcute Intestinal ObstructionDin LukbanNo ratings yet
- Ten Killing HandsDocument6 pagesTen Killing HandsKestricsNo ratings yet
- QualifiedPhysio MSK Interview Preparation Pack PDFDocument48 pagesQualifiedPhysio MSK Interview Preparation Pack PDFUkpabi GinikachiNo ratings yet
- WatsuDocument5 pagesWatsuTIME-TREVELER100% (1)
- MEDINA, JR. vs. PEOPLEDocument4 pagesMEDINA, JR. vs. PEOPLEKarmela ReyesNo ratings yet
- 2 WHO Standard Acupuncture Point Locations in The Western Part 2Document30 pages2 WHO Standard Acupuncture Point Locations in The Western Part 2Virgil Anma100% (1)
- Occupational Health and Safety ProceduresDocument15 pagesOccupational Health and Safety Proceduresmarlon felizardo100% (1)
- A Resuscitation Room Guide: Oxford Medical PublicationsDocument27 pagesA Resuscitation Room Guide: Oxford Medical PublicationsVitor Hugo G Correia0% (1)
- Affidavit Complaint Slight Physical InjuryDocument2 pagesAffidavit Complaint Slight Physical Injuryduanepo100% (1)
- Exam 2019 Answer OAPA: Criminal Law (University of London)Document5 pagesExam 2019 Answer OAPA: Criminal Law (University of London)Md. Yousuf RifatNo ratings yet
- Ins510 Group Project ReportDocument17 pagesIns510 Group Project Reportradia amalin99No ratings yet
- Anatomy of The Upper Extremities: The Shoulder ComplexDocument8 pagesAnatomy of The Upper Extremities: The Shoulder ComplexAlfred BajarNo ratings yet
- ART ACT No.1Document1 pageART ACT No.1Alfred BajarNo ratings yet
- Human Anatomy Worksheet1Document1 pageHuman Anatomy Worksheet1Alfred BajarNo ratings yet
- BAJAR, Pheodor Alfred D. 10/09/2020 PT 1-3 Sir Jed AbatayoDocument2 pagesBAJAR, Pheodor Alfred D. 10/09/2020 PT 1-3 Sir Jed AbatayoAlfred Bajar0% (1)
- 002 Cell Membrane PhysiologyDocument12 pages002 Cell Membrane PhysiologyAlfred BajarNo ratings yet
- Human Anatomy Worksheet1Document1 pageHuman Anatomy Worksheet1Alfred BajarNo ratings yet
- 004 Handout Musculoskelital - Upper Extremities PDFDocument13 pages004 Handout Musculoskelital - Upper Extremities PDFAlfred BajarNo ratings yet
- Membrane Potential Summary - FinalDocument6 pagesMembrane Potential Summary - FinalAlfred BajarNo ratings yet
- 001 HomeostasisDocument3 pages001 HomeostasisAlfred BajarNo ratings yet
- 002 Handout Basic Concepts Part 2Document8 pages002 Handout Basic Concepts Part 2Alfred BajarNo ratings yet
- Bostitch 650S4 ManualDocument32 pagesBostitch 650S4 ManualsixstringNo ratings yet
- Syndesmosis GoodDocument35 pagesSyndesmosis GoodRoger WatersNo ratings yet
- S Das 13th Edition - Medical-Downloads - Com HerniaDocument17 pagesS Das 13th Edition - Medical-Downloads - Com HerniaVishwajeet RaneNo ratings yet
- Critical Injuries Table - Critical Injury TableDocument2 pagesCritical Injuries Table - Critical Injury TableWesleyNo ratings yet
- A Game of HeartsDocument332 pagesA Game of HeartsMolly FranklynNo ratings yet
- Mucocele of The Glands of Blandin-Nuhn - Case ReportDocument5 pagesMucocele of The Glands of Blandin-Nuhn - Case ReportLjubomirErdoglijaNo ratings yet
- Ao ClassificatiDocument7 pagesAo Classificatiapi-3743776No ratings yet
- The Immediate Effects of Muscle Energy Technique On Posterior Shoulder TightnessDocument8 pagesThe Immediate Effects of Muscle Energy Technique On Posterior Shoulder Tightnesssulis tiyowatiNo ratings yet
- Edx Braquial PlexusDocument30 pagesEdx Braquial PlexusMariana GNo ratings yet
- Test 3 BDSDocument16 pagesTest 3 BDSrababNo ratings yet
- Khemri PlaybookDocument7 pagesKhemri PlaybookDaniel RadfordNo ratings yet
- Mines and Geosciences Bureau: Regional Office No. XIIDocument3 pagesMines and Geosciences Bureau: Regional Office No. XIIErmelyn Jane CelindroNo ratings yet
- Work SimplificationDocument3 pagesWork SimplificationZabNo ratings yet