You might also like
- Rules and Directions for the Employment of Injections in Various DiseasesFrom EverandRules and Directions for the Employment of Injections in Various DiseasesNo ratings yet
- Female Urinary Catheter Insertion GuideDocument9 pagesFemale Urinary Catheter Insertion GuideIsabel AranconNo ratings yet
- 6 Urinary EliminationDocument5 pages6 Urinary EliminationkhautedameNo ratings yet
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenFrom EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenNo ratings yet
- CatheterizationDocument23 pagesCatheterizationyuuki konnoNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Urinary CatheterizationDocument35 pagesUrinary CatheterizationrnrmmanphdNo ratings yet
- Diverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookFrom EverandDiverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookNo ratings yet
- Urinary EliminationDocument9 pagesUrinary EliminationTuTitNo ratings yet
- Urinary CatheterizationDocument37 pagesUrinary CatheterizationCharles100% (2)
- CATHETERIZATIONDocument33 pagesCATHETERIZATIONClaireNo ratings yet
- Urinary-Catheterization (1)Document31 pagesUrinary-Catheterization (1)hazel jamisNo ratings yet
- Catheterization: A Guide to Proper TechniqueDocument33 pagesCatheterization: A Guide to Proper TechniqueJoseph DusichNo ratings yet
- UrologyDocument9 pagesUrologyDrmirfat AlkashifNo ratings yet
- Urinary Interventions: By: Nursing Skills Laboratory GroupDocument57 pagesUrinary Interventions: By: Nursing Skills Laboratory GroupMelinda Cariño BallonNo ratings yet
- Bladder IrrigationDocument6 pagesBladder IrrigationKent Martin AmorosoNo ratings yet
- Organizing supplies before beginning theprocedure promotes efficiency and preventscontaminationDocument71 pagesOrganizing supplies before beginning theprocedure promotes efficiency and preventscontaminationlouie roderosNo ratings yet
- Foley Catheter PlacementDocument16 pagesFoley Catheter PlacementAlana CaballeroNo ratings yet
- Bedpans and UrinalsDocument4 pagesBedpans and UrinalsCham De Leon50% (4)
- Rle MidtermDocument77 pagesRle MidtermTrishaNo ratings yet
- Catheterization GuideDocument28 pagesCatheterization Guidesushma shresthaNo ratings yet
- Indwelling Urinary Catheterization 1Document5 pagesIndwelling Urinary Catheterization 1Mercy Anne EcatNo ratings yet
- CATHETERIZATIONDocument13 pagesCATHETERIZATIONSarah Uy Caronan100% (1)
- CatheterizationDocument22 pagesCatheterizationravizbeea8No ratings yet
- Guide to Urinary Catheterization & Urinalysis TestsDocument28 pagesGuide to Urinary Catheterization & Urinalysis TestsArie AngkiriwangNo ratings yet
- Catheterization Procedure and Care GuidelinesDocument43 pagesCatheterization Procedure and Care GuidelinesJen Tirapan100% (2)
- Bladder Irrigation 4Document23 pagesBladder Irrigation 4Jay Shree100% (2)
- Check List of Urinary Catheterization For EMT LevelDocument12 pagesCheck List of Urinary Catheterization For EMT LevelFikir Ligisinaw AyalkimNo ratings yet
- Urinary Catheterization For PediatricsDocument6 pagesUrinary Catheterization For PediatricsMichael Montinola100% (1)
- Indwelling Catheterization ProcedureDocument5 pagesIndwelling Catheterization ProcedureNiña Jean Tormis AldabaNo ratings yet
- How to Insert and Remove an Indwelling Urinary CatheterDocument21 pagesHow to Insert and Remove an Indwelling Urinary CatheterMarvin ReyesNo ratings yet
- Catheterization: Types, Insertion & ComplicationsDocument21 pagesCatheterization: Types, Insertion & ComplicationsGiFt Wimolratanachaisiri0% (1)
- Urinary CatheterisationDocument24 pagesUrinary CatheterisationmustaphaNo ratings yet
- Catheterization and Perineal Care-PPT-1Document49 pagesCatheterization and Perineal Care-PPT-1AinaB Manalo100% (1)
- Urinary Bladder Irrigation FDocument6 pagesUrinary Bladder Irrigation FDrmirfat AlkashifNo ratings yet
- Urinary Elimination 26Document1 pageUrinary Elimination 26Mitul PeterNo ratings yet
- PARACENTESISDocument15 pagesPARACENTESISSoonh ChannaNo ratings yet
- CATHETERIZATIONDocument3 pagesCATHETERIZATIONanimesh pandaNo ratings yet
- CatheterizationDocument46 pagesCatheterizationJam Maj60% (5)
- Care of Patient With Supra Pubic CatheterDocument8 pagesCare of Patient With Supra Pubic CatheterAnusha VergheseNo ratings yet
- Urinary CatheterDocument13 pagesUrinary CatheterjeorjNo ratings yet
- Urinary CatheterizationDocument41 pagesUrinary CatheterizationSteffiNo ratings yet
- Male CatheterizationDocument37 pagesMale CatheterizationJean Rynne BongaisNo ratings yet
- Urinary Elimination and CatheterizationDocument41 pagesUrinary Elimination and CatheterizationMaria Margarita100% (1)
- Male Fem CathDocument31 pagesMale Fem CathAya AbeciaNo ratings yet
- Urinary CatheterizationDocument5 pagesUrinary CatheterizationRita PokharelNo ratings yet
- Clinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareDocument8 pagesClinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareLeeNo ratings yet
- Male Female Catheterization Rle 30Document95 pagesMale Female Catheterization Rle 30HoneylouAzOpondaNo ratings yet
- Retdem Week 8Document9 pagesRetdem Week 8Iris FrancheNo ratings yet
- NCM - CatheterizationDocument3 pagesNCM - CatheterizationYanna Habib-MangotaraNo ratings yet
- CatheterizationDocument32 pagesCatheterizationJohn Dave V. VillarmenteNo ratings yet
- Fundamentals ofDocument23 pagesFundamentals ofSUSPANo ratings yet
- Checklist RLE IFCDocument2 pagesChecklist RLE IFCハンスー アグバヤにNo ratings yet
- CystoclysisDocument29 pagesCystoclysisKate PedzNo ratings yet
- 13 CatheterizationDocument39 pages13 CatheterizationKelfala Hassan DawohNo ratings yet
- Safetey BundlesDocument34 pagesSafetey BundlesshafinaNo ratings yet
- Male Catheterization (Indwelling)Document43 pagesMale Catheterization (Indwelling)Dan Floyd FernandezNo ratings yet
- Abdominal ParacentesisDocument4 pagesAbdominal Paracentesisgurneet kourNo ratings yet
- Urinary CatheterizattionDocument85 pagesUrinary Catheterizattionbajaoc100% (6)
- Role and ResponsibilitiesDocument1 pageRole and ResponsibilitiesVinz Khyl G. CastillonNo ratings yet
- STS Module on Science, Tech and the Human ConditionDocument8 pagesSTS Module on Science, Tech and the Human ConditionVinz Khyl G. CastillonNo ratings yet
- NQS - August2020 (Phase2) - FinalDocument5 pagesNQS - August2020 (Phase2) - FinalVinz Khyl G. CastillonNo ratings yet
- GeoWave Earthquake Detector Business PlanDocument78 pagesGeoWave Earthquake Detector Business PlanVinz Khyl G. CastillonNo ratings yet
- STS Course: Aristotle's Views on Human FlourishingDocument30 pagesSTS Course: Aristotle's Views on Human FlourishingVinz Khyl G. CastillonNo ratings yet
- Indwelling Urinary Catheter - MaleDocument9 pagesIndwelling Urinary Catheter - MaleVinz Khyl G. CastillonNo ratings yet
- 12 Lead ECGDocument9 pages12 Lead ECGVinz Khyl G. CastillonNo ratings yet
- Disorders of The EyeDocument15 pagesDisorders of The EyeVinz Khyl G. Castillon100% (2)
- Gone Girl Monologue Amy PDFDocument2 pagesGone Girl Monologue Amy PDFVinz Khyl G. CastillonNo ratings yet
- Phenylephrine Hydrochloride PDFDocument5 pagesPhenylephrine Hydrochloride PDFVinz Khyl G. CastillonNo ratings yet
- Controlling asthma with AlbuterolDocument2 pagesControlling asthma with AlbuterolVinz Khyl G. CastillonNo ratings yet
- Notes On Global Media CulturesDocument4 pagesNotes On Global Media CulturesPrincessNo ratings yet
- EhDocument123 pagesEhRed TanNo ratings yet
- Ear Disorders ExplainedDocument8 pagesEar Disorders ExplainedVinz Khyl G. CastillonNo ratings yet
- Howell, Martha and Walter PrevenierDocument1 pageHowell, Martha and Walter PrevenierVinz Khyl G. CastillonNo ratings yet
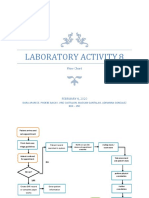
- Activity 8Document2 pagesActivity 8Vinz Khyl G. CastillonNo ratings yet
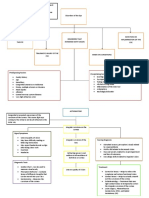
- Concept MapDocument2 pagesConcept MapVinz Khyl G. CastillonNo ratings yet
- Reflection RubricDocument1 pageReflection RubricVinz Khyl G. CastillonNo ratings yet
- English 7 NC Timetable THF 10:30 Date Lessons/Tasks/ActivitiesDocument2 pagesEnglish 7 NC Timetable THF 10:30 Date Lessons/Tasks/ActivitiesVinz Khyl G. CastillonNo ratings yet
- Infectious and Inflammatory Disorders of Bones and JointsDocument5 pagesInfectious and Inflammatory Disorders of Bones and JointsVinz Khyl G. CastillonNo ratings yet
- Case PresentationDocument4 pagesCase PresentationVinz Khyl G. CastillonNo ratings yet
- Generic Name (Brand Name) Methergine (Methylergonovine Maleate)Document3 pagesGeneric Name (Brand Name) Methergine (Methylergonovine Maleate)jennix_030883% (6)
- Nutritional Assessment StagesDocument6 pagesNutritional Assessment StagesVinz Khyl G. CastillonNo ratings yet
- The Growing Fetus During The Second TrimesterDocument5 pagesThe Growing Fetus During The Second TrimesterVinz Khyl G. CastillonNo ratings yet
- Pediatric Nursing. PPDocument4 pagesPediatric Nursing. PPVinz Khyl G. CastillonNo ratings yet
- Corporate Level Strategies ExplainedDocument30 pagesCorporate Level Strategies ExplainedNazir AnsariNo ratings yet
- September/News/Septiembre 2013: P.O. Box 44 WWW - Hecatomberecords.esDocument7 pagesSeptember/News/Septiembre 2013: P.O. Box 44 WWW - Hecatomberecords.eshecatomberecordsNo ratings yet
- Revised SCOPE OF WORK and SCCDocument363 pagesRevised SCOPE OF WORK and SCCZia KhanNo ratings yet
- 5187 0103Document141 pages5187 0103Aravind ArjunanNo ratings yet
- Introduction 130407092142 Phpapp01Document69 pagesIntroduction 130407092142 Phpapp01Pari Savla100% (1)
- Hangnails and HomoeopathyDocument7 pagesHangnails and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- PDF Penstock Manual DLDocument160 pagesPDF Penstock Manual DLWilmer Fernando DuarteNo ratings yet
- ProComp 2 Service Manual SM7008P-01Document22 pagesProComp 2 Service Manual SM7008P-01cobramcNo ratings yet
- Laws On Banks-A4Document16 pagesLaws On Banks-A4Steven OrtizNo ratings yet
- Greetings To EveryoneDocument2 pagesGreetings To EveryoneLouella MedinaNo ratings yet
- Dynamics: What Is A Force?Document13 pagesDynamics: What Is A Force?TorettoNo ratings yet
- Pas 220Document71 pagesPas 220JuwitaNo ratings yet
- Seniors Playing Record Nov 20 To Dec 2021 New SystemDocument6 pagesSeniors Playing Record Nov 20 To Dec 2021 New Systemapi-313355217No ratings yet
- Paths To Mastery Lesson 17 Speaking Tips From Dale Carnegie The Quick and Easy Way To Effective SpeakingDocument10 pagesPaths To Mastery Lesson 17 Speaking Tips From Dale Carnegie The Quick and Easy Way To Effective SpeakingZelic NguyenNo ratings yet
- Multimedia ExerciseDocument1 pageMultimedia ExercisemskgghNo ratings yet
- 1.1.5.a Elisa-3Document3 pages1.1.5.a Elisa-3Zainab DioufNo ratings yet
- ICT4D - Richard Heeks (2305843009216382716)Document307 pagesICT4D - Richard Heeks (2305843009216382716)Jeff GeoffNo ratings yet
- Trauma-Informed CounselingDocument1 pageTrauma-Informed Counselingapi-492010604No ratings yet
- Forming Plurals of NounsDocument5 pagesForming Plurals of NounsCathy GalNo ratings yet
- Royalstone ReadmeDocument2 pagesRoyalstone ReadmeAdnan BrianNo ratings yet
- GJ ScriptDocument83 pagesGJ ScriptKim LawrenceNo ratings yet
- Foreign Interests Shaped the War of the PacificDocument24 pagesForeign Interests Shaped the War of the PacificcustionesNo ratings yet
- MTSC QuestionsDocument8 pagesMTSC QuestionsAbhi RamNo ratings yet
- Underwater Cutting and Welding Equipment - 89250054 - AbDocument38 pagesUnderwater Cutting and Welding Equipment - 89250054 - AbAhmed Adel100% (1)
- Democracy Against Domination PDFDocument257 pagesDemocracy Against Domination PDFvmcosNo ratings yet
- MSDS TriacetinDocument4 pagesMSDS TriacetinshishirchemNo ratings yet
- Remove Head IsmDocument67 pagesRemove Head IsmjeremyNo ratings yet
- Everyman A Structural Analysis Thomas F. Van LaanDocument12 pagesEveryman A Structural Analysis Thomas F. Van LaanRodrigoCarrilloLopezNo ratings yet
- Vistara News and Tie UpDocument4 pagesVistara News and Tie UpDimple RathodNo ratings yet
- Mathematics Engagement in An Australian Lower Secondary SchoolDocument23 pagesMathematics Engagement in An Australian Lower Secondary SchoolDane SinclairNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1455)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipFrom EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipRating: 4.5 out of 5 stars4.5/5 (1135)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!From EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Rating: 4.5 out of 5 stars4.5/5 (10)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingFrom EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingRating: 4.5 out of 5 stars4.5/5 (103)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)