You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Nutritional Assessment StagesDocument6 pagesNutritional Assessment StagesVinz Khyl G. CastillonNo ratings yet
- Factory Act Gujarat PDFDocument2 pagesFactory Act Gujarat PDFKeith100% (1)
- Disorders of The EyeDocument15 pagesDisorders of The EyeVinz Khyl G. Castillon100% (2)
- Rosie Revere Teaching GuideDocument5 pagesRosie Revere Teaching GuideAbrams Books100% (1)
- Comey Memo To FBI EmployeesDocument2 pagesComey Memo To FBI EmployeesLaw&Crime100% (2)
- Salbutamol Drug StudyDocument2 pagesSalbutamol Drug StudyVinz Khyl G. CastillonNo ratings yet
- Generic Name (Brand Name) Methergine (Methylergonovine Maleate)Document3 pagesGeneric Name (Brand Name) Methergine (Methylergonovine Maleate)jennix_030883% (6)
- TCS-60 WebDocument94 pagesTCS-60 WebNasrul Salman100% (1)
- Staff Augmentation Agreement FormDocument11 pagesStaff Augmentation Agreement FormNijo JosephNo ratings yet
- Computer Systems Servicing NC II CGDocument238 pagesComputer Systems Servicing NC II CGRickyJeciel100% (2)
- Nipcib 000036Document273 pagesNipcib 000036AlfoFS0% (1)
- Assessment Task 2 2Document10 pagesAssessment Task 2 2Pratistha GautamNo ratings yet
- PEL 20161201 Dec 2016Document76 pagesPEL 20161201 Dec 2016RémiNo ratings yet
- Role and ResponsibilitiesDocument1 pageRole and ResponsibilitiesVinz Khyl G. CastillonNo ratings yet
- Indwelling Urinary Catheter FemaleDocument9 pagesIndwelling Urinary Catheter FemaleVinz Khyl G. CastillonNo ratings yet
- WEEK 7 8 STS and The Human Condition Part 1 1Document30 pagesWEEK 7 8 STS and The Human Condition Part 1 1Vinz Khyl G. CastillonNo ratings yet
- Group 1 Infratech Enterprise Business PlanDocument78 pagesGroup 1 Infratech Enterprise Business PlanVinz Khyl G. CastillonNo ratings yet
- STS Module Week 7 8 ST and The Human FlourishingDocument8 pagesSTS Module Week 7 8 ST and The Human FlourishingVinz Khyl G. CastillonNo ratings yet
- 12 Lead ECGDocument9 pages12 Lead ECGVinz Khyl G. CastillonNo ratings yet
- NQS - August2020 (Phase2) - FinalDocument5 pagesNQS - August2020 (Phase2) - FinalVinz Khyl G. CastillonNo ratings yet
- Notes On Global Media CulturesDocument4 pagesNotes On Global Media CulturesPrincessNo ratings yet
- EhDocument123 pagesEhRed TanNo ratings yet
- Disorders of The EarDocument8 pagesDisorders of The EarVinz Khyl G. CastillonNo ratings yet
- Phenylephrine Hydrochloride PDFDocument5 pagesPhenylephrine Hydrochloride PDFVinz Khyl G. CastillonNo ratings yet
- Gone Girl Monologue Amy PDFDocument2 pagesGone Girl Monologue Amy PDFVinz Khyl G. CastillonNo ratings yet
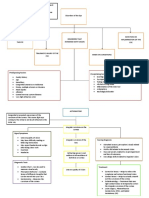
- Concept MapDocument2 pagesConcept MapVinz Khyl G. CastillonNo ratings yet
- Case PresentationDocument4 pagesCase PresentationVinz Khyl G. CastillonNo ratings yet
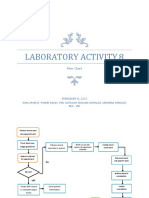
- Activity 8Document2 pagesActivity 8Vinz Khyl G. CastillonNo ratings yet
- Howell, Martha and Walter PrevenierDocument1 pageHowell, Martha and Walter PrevenierVinz Khyl G. CastillonNo ratings yet
- Infectious and Inflammatory Disorders of Bones and JointsDocument5 pagesInfectious and Inflammatory Disorders of Bones and JointsVinz Khyl G. CastillonNo ratings yet
- Reflection RubricDocument1 pageReflection RubricVinz Khyl G. CastillonNo ratings yet
- English 7 NC Timetable THF 10:30 Date Lessons/Tasks/ActivitiesDocument2 pagesEnglish 7 NC Timetable THF 10:30 Date Lessons/Tasks/ActivitiesVinz Khyl G. CastillonNo ratings yet
- Pediatric Nursing. PPDocument4 pagesPediatric Nursing. PPVinz Khyl G. CastillonNo ratings yet
- The Growing Fetus During The Second TrimesterDocument5 pagesThe Growing Fetus During The Second TrimesterVinz Khyl G. CastillonNo ratings yet
- Fruit and Vegetable Wash TdsDocument1 pageFruit and Vegetable Wash TdsEsheshNo ratings yet
- Summer Internship Project On: "Basics of PHP"Document45 pagesSummer Internship Project On: "Basics of PHP"its me Deepak yadav100% (1)
- 7 - 8 CSS - WK 3 Ergonomic Guidelines For Computer Workstations - Jesucrtina NimenzoDocument6 pages7 - 8 CSS - WK 3 Ergonomic Guidelines For Computer Workstations - Jesucrtina NimenzoEdelmar BenosaNo ratings yet
- 7diesel 2016Document118 pages7diesel 2016JoãoCarlosDaSilvaBrancoNo ratings yet
- Pre Int Work Book Unit 9Document8 pagesPre Int Work Book Unit 9Maria Andreina Diaz SantanaNo ratings yet
- User Access Guide PDFDocument3 pagesUser Access Guide PDFbaldo yellow4No ratings yet
- Sexual Hazartment of Women at OfficeDocument3 pagesSexual Hazartment of Women at OfficeMohandas PeriyasamyNo ratings yet
- Fundamental of HDD Technology (3) : OutlineDocument8 pagesFundamental of HDD Technology (3) : OutlineJoseMNo ratings yet
- List of Circulating Currencies by CountryDocument8 pagesList of Circulating Currencies by CountryVivek SinghNo ratings yet
- Aegps Manual Fluxpower Hpi Installation enDocument44 pagesAegps Manual Fluxpower Hpi Installation enAbdus SalamNo ratings yet
- Tutorial 3Document2 pagesTutorial 3AmrinaAkmal0% (1)
- Assignment 1technoDocument3 pagesAssignment 1technonadiyaxxNo ratings yet
- CFP The 17th International Computer Science and Engineering Conference (ICSEC 2013)Document1 pageCFP The 17th International Computer Science and Engineering Conference (ICSEC 2013)Davy SornNo ratings yet
- LT32567 PDFDocument4 pagesLT32567 PDFNikolayNo ratings yet
- Expansion Junction 1Document1 pageExpansion Junction 1kojjasNo ratings yet
- Module 1 Ethernet and VLAN: Lab 1-1 Ethernet Interface and Link Configuration Learning ObjectivesDocument15 pagesModule 1 Ethernet and VLAN: Lab 1-1 Ethernet Interface and Link Configuration Learning ObjectivesChaima BelhediNo ratings yet
- 6LoWPAN TutorialDocument45 pages6LoWPAN TutorialEdita LatifiNo ratings yet
- DWC Ordering InformationDocument15 pagesDWC Ordering InformationbalaNo ratings yet
- Casio fx-82MSDocument49 pagesCasio fx-82MSPéter GedeNo ratings yet
- Laser Ignition ReportDocument26 pagesLaser Ignition ReportRaHul100% (2)
- How The CBO Works: Jonathan Lewis WWW - Jlcomp.demon - Co.ukDocument37 pagesHow The CBO Works: Jonathan Lewis WWW - Jlcomp.demon - Co.ukomeratisNo ratings yet