0% found this document useful (0 votes)
297 views2 pagesFocus Charting Is Intended To Make Client and Client Concerns and Strengths The Focus of Care. 3 Columns
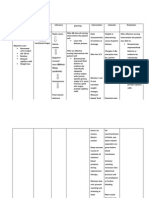
Focus charting organizes client information into three columns: date/time, focus of care (e.g., condition, symptom), and progress notes using a DAR (data, action, response) structure. The focus can be a medical concern, nursing diagnosis, behavior, or strength. Progress notes provide holistic client data to guide the nursing process. An example chart documents a client's fever, hypotension, surgical wound, and decreased appetite over time with nursing assessments and interventions.
Uploaded by
Jan Federick BantayCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
297 views2 pagesFocus Charting Is Intended To Make Client and Client Concerns and Strengths The Focus of Care. 3 Columns
Focus charting organizes client information into three columns: date/time, focus of care (e.g., condition, symptom), and progress notes using a DAR (data, action, response) structure. The focus can be a medical concern, nursing diagnosis, behavior, or strength. Progress notes provide holistic client data to guide the nursing process. An example chart documents a client's fever, hypotension, surgical wound, and decreased appetite over time with nursing assessments and interventions.
Uploaded by
Jan Federick BantayCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd