0% found this document useful (0 votes)
140 views6 pagesCritical Thinking in Nursing Care Evaluation
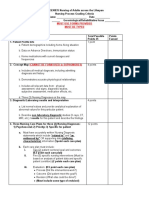
The nurse performed a safety check upon entering the patient's room which included hand hygiene, appropriate PPE, verifying the patient's ID band, and ensuring ergonomic safety. The nurse assessed the patient by taking vital signs, listening to the patient, and examining them. Interventions included administering the correct medications following all rights, adjusting the patient's oxygen as needed, and providing wound care. The nurse educated the patient on their medication, fall precautions, and ensured referrals were made as appropriate.
Uploaded by
yeseniaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
140 views6 pagesCritical Thinking in Nursing Care Evaluation
The nurse performed a safety check upon entering the patient's room which included hand hygiene, appropriate PPE, verifying the patient's ID band, and ensuring ergonomic safety. The nurse assessed the patient by taking vital signs, listening to the patient, and examining them. Interventions included administering the correct medications following all rights, adjusting the patient's oxygen as needed, and providing wound care. The nurse educated the patient on their medication, fall precautions, and ensured referrals were made as appropriate.
Uploaded by
yeseniaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd