You might also like
- Nter, Corporatecenter Entertainment Reimbursement: Total (Three Thousand Four Hundred Fifty Two Rupees Only)Document1 pageNter, Corporatecenter Entertainment Reimbursement: Total (Three Thousand Four Hundred Fifty Two Rupees Only)pukhrajsoniNo ratings yet
- Soa (MRGTWL00100005329581)Document2 pagesSoa (MRGTWL00100005329581)Arjun GNo ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document4 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Rakshit KashyapNo ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document4 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961shilpiNo ratings yet
- Abdfa2602a Q2 2019-20 PDFDocument2 pagesAbdfa2602a Q2 2019-20 PDFTarun AgarwalNo ratings yet
- Loan Account Statement For LACHD00039394344Document4 pagesLoan Account Statement For LACHD00039394344abhishek parasarNo ratings yet
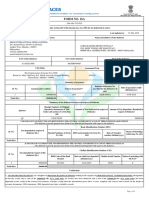
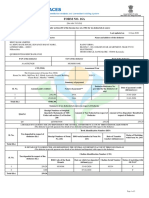
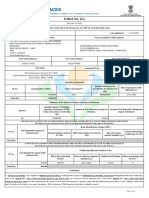
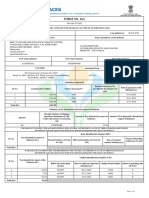
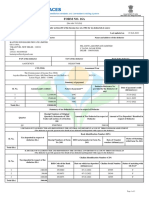
- Form No. 16A: From ToDocument2 pagesForm No. 16A: From ToMurthy KarumuriNo ratings yet
- Form 16A TDS CertificateDocument2 pagesForm 16A TDS CertificateSharad VermaNo ratings yet
- Hamara Pump Q1 Fy 2020-21Document3 pagesHamara Pump Q1 Fy 2020-21Advocate SkitaxNo ratings yet
- Activity 3Document5 pagesActivity 3Keith Joshua GabiasonNo ratings yet
- Ira Shalini M. YbañezDocument5 pagesIra Shalini M. YbañezIra YbanezNo ratings yet
- For Bill Payments, Use Any of The Digital Payment Options:: Name: Tushita MajumdarDocument3 pagesFor Bill Payments, Use Any of The Digital Payment Options:: Name: Tushita MajumdarhamsNo ratings yet
- Form No. 16A: From ToDocument2 pagesForm No. 16A: From ToAkriti JhaNo ratings yet
- Form No. 16A: From ToDocument2 pagesForm No. 16A: From Tosahil choudharyNo ratings yet
- Late Charges Report: Private and ConfidentialDocument3 pagesLate Charges Report: Private and ConfidentialAntonio Arroyo SolanoNo ratings yet
- Hamara Pump Q4 Fy 2019-20Document3 pagesHamara Pump Q4 Fy 2019-20Advocate SkitaxNo ratings yet
- TDS CertificateDocument2 pagesTDS CertificateJyoti MeenaNo ratings yet
- TechnotronicsDocument1 pageTechnotronicsviral patelNo ratings yet
- Anita Gangurde: Account StatementDocument7 pagesAnita Gangurde: Account Statementkiran gangurdeNo ratings yet
- TDS certificate detailsDocument3 pagesTDS certificate detailsVijaya KumariNo ratings yet
- AP #: 1900135531 Request For Payment: 2020-0169733: Status: TransmitDocument1 pageAP #: 1900135531 Request For Payment: 2020-0169733: Status: TransmitIlove music096No ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document4 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Xen Operation DPHNo ratings yet
- House No. 333, Link Road, Narrian Abbottabad, Abbottabad Abbottabad Khawar ShahidDocument4 pagesHouse No. 333, Link Road, Narrian Abbottabad, Abbottabad Abbottabad Khawar ShahidIkramNo ratings yet
- Loan Financial Summary As On 12/08/2020: Component Due (RS.) Receipt (RS.) Overdue (RS.)Document2 pagesLoan Financial Summary As On 12/08/2020: Component Due (RS.) Receipt (RS.) Overdue (RS.)Alexander SNo ratings yet
- Form No. 16A: From ToDocument2 pagesForm No. 16A: From ToDevasyrucNo ratings yet
- AIS Annual FinancialDocument2 pagesAIS Annual FinancialKamalalakshmi NarayananNo ratings yet
- Tax Invoice for Medical SuppliesDocument1 pageTax Invoice for Medical SuppliesPintu ShahNo ratings yet
- Loan Account Statement For 590Rdpgg942245: Component Due (RS.) Receipt (RS.) Overdue (RS.)Document4 pagesLoan Account Statement For 590Rdpgg942245: Component Due (RS.) Receipt (RS.) Overdue (RS.)H GOPAL KRISHNANo ratings yet
- Form No. 16A: From ToDocument2 pagesForm No. 16A: From Tomukti nath guptaNo ratings yet
- Traces: Form No. 16Document5 pagesTraces: Form No. 16blinkfinance7No ratings yet
- 26ASDocument4 pages26ASAnubhav AsatiNo ratings yet
- Form No. 16A: From ToDocument2 pagesForm No. 16A: From ToShankara NarayananNo ratings yet
- Loan Account Statement For LUCHD00037184487Document4 pagesLoan Account Statement For LUCHD00037184487abhishek parasarNo ratings yet
- BBGPV1509K Q2 2019-20 Vandana S PrasadDocument2 pagesBBGPV1509K Q2 2019-20 Vandana S PrasadKapil PandeyNo ratings yet
- Form 16A TDS CertificateDocument2 pagesForm 16A TDS CertificateJAYDIPVDNo ratings yet
- Form16 Till 14 Dec 2019Document11 pagesForm16 Till 14 Dec 2019Aviral SankhyadharNo ratings yet
- Annual Tax StatementDocument4 pagesAnnual Tax StatementATSI InstituteNo ratings yet
- TDS Certificate SummaryDocument2 pagesTDS Certificate SummaryAkriti JhaNo ratings yet
- Toyota Financial Services India Ltd. Account StatementDocument4 pagesToyota Financial Services India Ltd. Account StatementaliNo ratings yet
- Ahhpt7531m 2020-21 PDFDocument2 pagesAhhpt7531m 2020-21 PDFAshish BhartiNo ratings yet
- MD Azhar Badruddin: Account StatementDocument6 pagesMD Azhar Badruddin: Account StatementMD AZHARNo ratings yet
- Form 26AS Annual Tax StatementDocument4 pagesForm 26AS Annual Tax StatementFiroz AminNo ratings yet
- Piramal SoaReportDocument10 pagesPiramal SoaReportVishalNo ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document4 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961NirajNo ratings yet
- Form No. 16A: From ToDocument3 pagesForm No. 16A: From ToMUNNA SKNo ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document8 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Baliram KendreNo ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document7 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961AshishNo ratings yet
- Somya Amritanshu - Arcpa1206b - Q2 - Ay202223Document3 pagesSomya Amritanshu - Arcpa1206b - Q2 - Ay202223Sourabh PunshiNo ratings yet
- Form 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961Document4 pagesForm 26AS: Annual Tax Statement Under Section 203AA of The Income Tax Act, 1961ghss chinniNo ratings yet
- Form No. 16A: From ToDocument3 pagesForm No. 16A: From ToAGE (I) R&D AVADI ChennaiNo ratings yet
- Hamara Punmp Q4 Fy 2021-2022Document3 pagesHamara Punmp Q4 Fy 2021-2022Advocate SkitaxNo ratings yet
- Loan Account Statement For LUCHD00036371505Document5 pagesLoan Account Statement For LUCHD00036371505abhishek parasarNo ratings yet
- Annual Tax Statement Form 26ASDocument4 pagesAnnual Tax Statement Form 26ASMadhukar GuptaNo ratings yet
- Geeta - Form 16 A 2022-23Document2 pagesGeeta - Form 16 A 2022-23Sourabh PunshiNo ratings yet
- Hero Fincorp Ltd. Account Statement Generated On (Date & Time) :29/11/2022 04:27:41Document6 pagesHero Fincorp Ltd. Account Statement Generated On (Date & Time) :29/11/2022 04:27:41Raju BhaiNo ratings yet
- Aadcp9992n Q3 2023-24Document3 pagesAadcp9992n Q3 2023-24Harikrishan BhattNo ratings yet
- A Comparative Analysis of Tax Administration in Asia and the Pacific: Fifth EditionFrom EverandA Comparative Analysis of Tax Administration in Asia and the Pacific: Fifth EditionNo ratings yet
- A Comparative Analysis of Tax Administration in Asia and the Pacific—Sixth EditionFrom EverandA Comparative Analysis of Tax Administration in Asia and the Pacific—Sixth EditionNo ratings yet
- Capital Structure and Profitability: S&P 500 Enterprises in the Light of the 2008 Financial CrisisFrom EverandCapital Structure and Profitability: S&P 500 Enterprises in the Light of the 2008 Financial CrisisNo ratings yet
- J.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineFrom EverandJ.K. Lasser's Small Business Taxes 2021: Your Complete Guide to a Better Bottom LineNo ratings yet
- Document No. 1-102 Rev. No. 0 Date 3-Sep-20 Sub-Vendor List & Categorization Plan For Chlorine Di-Oxide Plant PackageDocument1 pageDocument No. 1-102 Rev. No. 0 Date 3-Sep-20 Sub-Vendor List & Categorization Plan For Chlorine Di-Oxide Plant PackagepukhrajsoniNo ratings yet
- India Conveyors Drive Schedule R&M ProjectDocument1 pageIndia Conveyors Drive Schedule R&M ProjectpukhrajsoniNo ratings yet
- Parameter ComparisonDocument3 pagesParameter ComparisonpukhrajsoniNo ratings yet
- CCC-06 Po4500003421Document1 pageCCC-06 Po4500003421pukhrajsoniNo ratings yet
- N T Climited: IssueDocument4 pagesN T Climited: IssuepukhrajsoniNo ratings yet
- Awwa M45 PDFDocument2 pagesAwwa M45 PDFKoray Kaan Özdemir0% (7)
- Car Adv Interest RepaymentDocument1 pageCar Adv Interest RepaymentpukhrajsoniNo ratings yet
- N T Climited: IssueDocument4 pagesN T Climited: IssuepukhrajsoniNo ratings yet
- Nter, Corporatecenter Entertainment Reimbursement: Total (Three Thousand Four Hundred Fifty Two Rupees Only)Document1 pageNter, Corporatecenter Entertainment Reimbursement: Total (Three Thousand Four Hundred Fifty Two Rupees Only)pukhrajsoniNo ratings yet
- N T Climited: IssueDocument4 pagesN T Climited: IssuepukhrajsoniNo ratings yet
- Awwa M45 PDFDocument2 pagesAwwa M45 PDFKoray Kaan Özdemir0% (7)
- Car Adv Iyment PDFDocument1 pageCar Adv Iyment PDFpukhrajsoniNo ratings yet
- NSPCL Comments Response Sheet for Coal Conveying System R&M ProjectDocument2 pagesNSPCL Comments Response Sheet for Coal Conveying System R&M ProjectpukhrajsoniNo ratings yet
- JVVNL Payment Receipt Copy for K Number 2104130003340Document1 pageJVVNL Payment Receipt Copy for K Number 2104130003340pukhrajsoniNo ratings yet
- Engineering Progress Report As On 08-07-2020Document3 pagesEngineering Progress Report As On 08-07-2020pukhrajsoniNo ratings yet
- RFC87Document6 pagesRFC87pukhrajsoniNo ratings yet
- Catogarization Plan For Chlorination System-C&IDocument1 pageCatogarization Plan For Chlorination System-C&IpukhrajsoniNo ratings yet
- BHEL Reply To BHEL Queries DT: 06.08.2019 As BelowDocument2 pagesBHEL Reply To BHEL Queries DT: 06.08.2019 As BelowpukhrajsoniNo ratings yet
- PaintDocument1 pagePaintpukhrajsoniNo ratings yet
- CRS - GA of APH GAD Notes PDFDocument1 pageCRS - GA of APH GAD Notes PDFpukhrajsoniNo ratings yet
- PulleysDocument2 pagesPulleyspukhrajsoniNo ratings yet
- PipelineDocument1 pagePipelinepukhrajsoniNo ratings yet
- New Text DocumentDocument1 pageNew Text DocumentpukhrajsoniNo ratings yet
- NTPC tender for combustion modification workDocument14 pagesNTPC tender for combustion modification workpukhrajsoniNo ratings yet
- DBR of Ventilation System 162Document10 pagesDBR of Ventilation System 162pukhrajsoniNo ratings yet
- People Who Help UsDocument2 pagesPeople Who Help UspukhrajsoniNo ratings yet
- NSSMC - Sulfuric Acid Dew Resistant CS Tube PDFDocument3 pagesNSSMC - Sulfuric Acid Dew Resistant CS Tube PDFaseNo ratings yet
- Motor and Inertia LoadDocument4 pagesMotor and Inertia LoadKiran Kumar K TNo ratings yet