You might also like
- A Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealFrom EverandA Beginner's Guide to Disability Insurance Claims in Canada: How to Apply for and Win Payment of Disability Insurance Benefits, Even After a Denial or Unsuccessful AppealNo ratings yet
- Guardian - VSP Choice PPO Plan Summary 2022Document3 pagesGuardian - VSP Choice PPO Plan Summary 2022Jessi ChallagullaNo ratings yet
- Vision Plan Summary: In-Network BenefitsDocument2 pagesVision Plan Summary: In-Network BenefitsKOMATSU SHOVELNo ratings yet
- Vision Highlight Sheet for Bugatchi Group, IncDocument3 pagesVision Highlight Sheet for Bugatchi Group, Incdayron ruizNo ratings yet
- Vision Benefit Summary1-87omkcDocument2 pagesVision Benefit Summary1-87omkcapi-307235383No ratings yet
- Vision Benefits Summary - 2017Document2 pagesVision Benefits Summary - 2017SporkleNo ratings yet
- EyeMed Benefits SummaryDocument2 pagesEyeMed Benefits SummarynikhilNo ratings yet
- Aetna Vision CoreDocument2 pagesAetna Vision CoreBeau PeskaNo ratings yet
- EyeMed SummaryDocument2 pagesEyeMed Summaryyoungstarbuck3606No ratings yet
- Denali One Life VisionDocument3 pagesDenali One Life VisionJohn BerkowitzNo ratings yet
- Life Is Better in Focus.: Consumers'Document2 pagesLife Is Better in Focus.: Consumers'Sakuryu TsukinoNo ratings yet
- Your VSP Vision Benefits Summary: Frequency Copay Description BenefitDocument1 pageYour VSP Vision Benefits Summary: Frequency Copay Description BenefitVictor LepriNo ratings yet
- Vision - Guardian Benefit Summary - VWG - 7.26.22Document5 pagesVision - Guardian Benefit Summary - VWG - 7.26.22Shiendra HalipaNo ratings yet
- PSU Graduate Students Vision Insurance BenefitsDocument3 pagesPSU Graduate Students Vision Insurance BenefitsenzoNo ratings yet
- Fee ScheduleDocument1 pageFee ScheduleTrevor J RajNo ratings yet
- Bluevision Plus: A Plan For Healthy Eyes, Healthy LivesDocument4 pagesBluevision Plus: A Plan For Healthy Eyes, Healthy LivesShumaila ParveenNo ratings yet
- VisionDocument5 pagesVisionCarl WiltNo ratings yet
- Your Davis Vision Premier Plan BenefitsDocument2 pagesYour Davis Vision Premier Plan BenefitsdebreallenNo ratings yet
- UHC Vision Plan SummaryDocument2 pagesUHC Vision Plan SummaryJanet Zimmerman McNicholNo ratings yet
- AARP UHC 2024 Benefit Highlights LA 004P FocusDocument4 pagesAARP UHC 2024 Benefit Highlights LA 004P FocusAlaa ZaidNo ratings yet
- Archie MD VisionDocument3 pagesArchie MD VisionAshutoshNiRanjanNo ratings yet
- SPD 422391812Document2 pagesSPD 422391812David DangNo ratings yet
- 2024 - US Healthcare One PagerDocument14 pages2024 - US Healthcare One PagerAsad AllibhoyNo ratings yet
- 2016 FEP BlueVisionDocument2 pages2016 FEP BlueVisionGopal GopinathNo ratings yet
- US Apple Vision Plan Overview JAN152021 enDocument1 pageUS Apple Vision Plan Overview JAN152021 enCT NguonNo ratings yet
- 2022 Steven Charles BAG - CODocument4 pages2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaNo ratings yet
- KP - Plan Summary Medical - PPODocument3 pagesKP - Plan Summary Medical - PPOshanegbaker51No ratings yet
- Photon Benefits SummaryDocument7 pagesPhoton Benefits SummarysojithesouljaNo ratings yet
- M2A1 US Census Data SearchDocument6 pagesM2A1 US Census Data SearchragcajunNo ratings yet
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Document3 pagesBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherNo ratings yet
- Employee Benefits-Wellness Guide 2023-24Document30 pagesEmployee Benefits-Wellness Guide 2023-24shanzeh2609No ratings yet
- Nce Member Handbook Dental ShieldDocument16 pagesNce Member Handbook Dental Shieldapi-304807209No ratings yet
- 22 23intlinsuranceDocument10 pages22 23intlinsuranceGangineni NareshNo ratings yet
- Wisconsin Specific InformationDocument9 pagesWisconsin Specific InformationLance MNo ratings yet
- Generic Open Enrollment KitDocument22 pagesGeneric Open Enrollment KitSteve BarrowsNo ratings yet
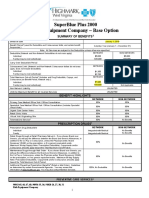
- SuperBlue Plus 2000 Plan Summary Highlights Benefits Deductibles CopaysDocument4 pagesSuperBlue Plus 2000 Plan Summary Highlights Benefits Deductibles CopaysSean MurrayNo ratings yet
- TNS Brochure 2021Document9 pagesTNS Brochure 2021chugn245No ratings yet
- Star Out Patient Care Insurance PolicyV 1.0may2023Document37 pagesStar Out Patient Care Insurance PolicyV 1.0may2023ठाकुर सूरज राणाNo ratings yet
- Unitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageDocument9 pagesUnitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageAdam CliftonNo ratings yet
- S608CHC Blue Choice Silver PPO 024: This Is Only A SummaryDocument8 pagesS608CHC Blue Choice Silver PPO 024: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Final Draft Gig Harbor Enrollment Guide 2024Document24 pagesFinal Draft Gig Harbor Enrollment Guide 2024api-307235383No ratings yet
- Important Questions Answers Why This Matters:: IndividualDocument7 pagesImportant Questions Answers Why This Matters:: Individualsashank varmaNo ratings yet
- G622CHC Blue Choice Gold PPO 022: This Is Only A SummaryDocument8 pagesG622CHC Blue Choice Gold PPO 022: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- Plan Plan Plan Premium: Important Questions Answers Why This MattersDocument9 pagesPlan Plan Plan Premium: Important Questions Answers Why This MattersIvan GrondonaNo ratings yet
- VEBA Plan PresentationDocument19 pagesVEBA Plan PresentationMitchell BigleyNo ratings yet
- This Is Only A Summary.: Important Questions Answers Why This MattersDocument10 pagesThis Is Only A Summary.: Important Questions Answers Why This MattersAnonymous D47ZzQZDtNo ratings yet
- University of Missouri Kansas City International SBC 500499912071900371 FINAL 2Document7 pagesUniversity of Missouri Kansas City International SBC 500499912071900371 FINAL 2maheshm_erpNo ratings yet
- Bec Plan WordDocument11 pagesBec Plan Wordprint1156No ratings yet
- EmblemHealth Benefits 2019Document7 pagesEmblemHealth Benefits 2019Jorge Luis Rivera AgostoNo ratings yet
- WWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesWWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersRohitKumarNo ratings yet
- Pharmacy Insurance BasicsDocument10 pagesPharmacy Insurance BasicsMarquita HunterNo ratings yet
- 2020 Ankura Benefits GuideDocument20 pages2020 Ankura Benefits GuidegpperkNo ratings yet
- B601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryDocument8 pagesB601CHC Blue Choice Bronze PPO 031: This Is Only A SummaryAnonymous nx3VC6zHn2No ratings yet
- 2017 UHC EPO Benefit Summary Muping Health InsuranceDocument16 pages2017 UHC EPO Benefit Summary Muping Health InsurancescartoonNo ratings yet
- SuperBlue Plus 2000 Plan SummaryDocument4 pagesSuperBlue Plus 2000 Plan Summarymichala anthonyNo ratings yet
- Flexi 60: Cover SummaryDocument2 pagesFlexi 60: Cover SummaryJSBTOOLSNo ratings yet
- OSHC Extras cover for dental, optical, physio & moreDocument4 pagesOSHC Extras cover for dental, optical, physio & moreAditya ArnandaNo ratings yet
- Unum Dental Policy ScheduleDocument7 pagesUnum Dental Policy ScheduleAhzan AliNo ratings yet
- Anthem Gold Pathway X HMO 1400 SBC SummaryDocument12 pagesAnthem Gold Pathway X HMO 1400 SBC SummaryscheriNo ratings yet
- 25M AXA HCA Prime 500K (Medical)Document19 pages25M AXA HCA Prime 500K (Medical)Aljes ReyesNo ratings yet
- Sequoia One Peo, LLC: Vision Option 1Document8 pagesSequoia One Peo, LLC: Vision Option 1shawkcontestNo ratings yet
- RW L Parent GuideDocument42 pagesRW L Parent GuideshawkcontestNo ratings yet
- Suzuki Vol. 2 PDFDocument20 pagesSuzuki Vol. 2 PDFAlejandra Reinita Vera Ibarra100% (1)
- The Beauty of MathematicsDocument12 pagesThe Beauty of Mathematicsconnling100% (1)
- ASA - Fall Workshop 11 FlyerDocument3 pagesASA - Fall Workshop 11 FlyershawkcontestNo ratings yet
- Germany Health Benefits SummaryDocument6 pagesGermany Health Benefits Summarytracy leeNo ratings yet
- Eligibility Review: WWW - Dshs.wa - GovDocument7 pagesEligibility Review: WWW - Dshs.wa - GovJosh CopelandNo ratings yet
- Business Environment Health-Care Industry: Submitted ToDocument5 pagesBusiness Environment Health-Care Industry: Submitted ToNandan ChoudharyNo ratings yet
- Change Plan for Medical Aid SchemeDocument16 pagesChange Plan for Medical Aid SchemetinoNo ratings yet
- OD4954 Medical Couriers Industry ReportDocument30 pagesOD4954 Medical Couriers Industry ReportAlexandra Chevalier100% (1)
- Lean Manajemen, Health Insurance Claim. CasemixDocument12 pagesLean Manajemen, Health Insurance Claim. Casemixsun flowerNo ratings yet
- A Comparative Analysis of Australia-S Healthcare SystemDocument37 pagesA Comparative Analysis of Australia-S Healthcare SystemShafia Akter RanuNo ratings yet
- PNCA Student Handbook 2018Document85 pagesPNCA Student Handbook 2018gilmastorgNo ratings yet
- Employer FlyerDocument1 pageEmployer Flyercnikmard1No ratings yet
- Welcome To CanadaDocument89 pagesWelcome To Canadaapi-3761095No ratings yet
- Health Service ProvidersDocument5 pagesHealth Service ProvidersNica MonrealNo ratings yet
- (Ebook - Health) Guide To Health InsuranceDocument28 pages(Ebook - Health) Guide To Health InsuranceAndrei CarlanNo ratings yet
- KPS Summary WebDocument24 pagesKPS Summary WebjosephlordNo ratings yet
- Handbook guides heirs through successionDocument84 pagesHandbook guides heirs through successionVenugopalan Srinivasan100% (1)
- Five (5) Fiscal Major Problems of Philippine Health Insurance Corporation (Philhealth)Document7 pagesFive (5) Fiscal Major Problems of Philippine Health Insurance Corporation (Philhealth)drei0% (2)
- Consumer Awareness About InsuranceDocument12 pagesConsumer Awareness About InsuranceEr Vishal RatheeNo ratings yet
- The Health Care Handbook - A Clear and Concise Guide To The United States Health Care System, 2nd EditionDocument321 pagesThe Health Care Handbook - A Clear and Concise Guide To The United States Health Care System, 2nd EditionSOUFIANE RACHID78% (9)
- Offer Letter - 3-Apr-2023 - 03 - 27 - 27Document17 pagesOffer Letter - 3-Apr-2023 - 03 - 27 - 27TechnetNo ratings yet
- Santerre Neun - Chapter 5Document65 pagesSanterre Neun - Chapter 5rotat2348No ratings yet
- Medicaid Waiver Guide 3-2013 - CDocument39 pagesMedicaid Waiver Guide 3-2013 - CMelissa Simpson HouseNo ratings yet
- Insurance Japan Long TermDocument9 pagesInsurance Japan Long TermutisariNo ratings yet
- Medical Laws, Ethics and Bioethics For The Health ProfessionalsDocument20 pagesMedical Laws, Ethics and Bioethics For The Health ProfessionalsilomurtalaNo ratings yet
- Sample North Carolina Auto Insurance PolicyDocument25 pagesSample North Carolina Auto Insurance PolicyrnfvieecNo ratings yet
- Objective 7.01 Key TermsDocument3 pagesObjective 7.01 Key TermsHeather CovingtonNo ratings yet
- Poilcy Guidelines & Help ManualDocument32 pagesPoilcy Guidelines & Help ManualHarshad PaigudeNo ratings yet
- Community Needs AssessmentDocument59 pagesCommunity Needs AssessmentJill Stowe100% (1)
- Medical Insurance PolicyDocument1 pageMedical Insurance Policypetersotocepeda123No ratings yet
- Unit 1 - Introduction To Health SystemsDocument29 pagesUnit 1 - Introduction To Health SystemsChikezie NwankworNo ratings yet
- Health Recharge - Single SheeterDocument2 pagesHealth Recharge - Single SheeterRavi JoshiNo ratings yet
- Student Health Insurance: San José State UniversityDocument20 pagesStudent Health Insurance: San José State UniversityDeni ZenNo ratings yet