You might also like
- Hematology, Immunology & OncologyDocument10 pagesHematology, Immunology & Oncologyjennaaahhh67% (3)
- Necrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric PatientsDocument4 pagesNecrotizing Pneumonitis Caused by Mycoplasma Pneumoniae in Pediatric Patientswawa chenNo ratings yet
- WJG 19 5178Document5 pagesWJG 19 5178aalmadasalazarNo ratings yet
- JCM 11 05684 v2Document13 pagesJCM 11 05684 v2Qwerty AsdfghNo ratings yet
- Neutrophil Dysregulation During SepsisDocument11 pagesNeutrophil Dysregulation During SepsisUntuk DownloadNo ratings yet
- Igg4-Related Hypophysitis Presenting As A Pituitary Adenoma With Systemic DiseaseDocument5 pagesIgg4-Related Hypophysitis Presenting As A Pituitary Adenoma With Systemic DiseasefelipetheNo ratings yet
- Cutaneous Polyarteritis Nodosa in A Child FollowinDocument2 pagesCutaneous Polyarteritis Nodosa in A Child FollowinandresrogersNo ratings yet
- Use Only: Acute Interstitial Nephritis: Etiology, Pathogenesis, Diagnosis, Treatment and PrognosisDocument8 pagesUse Only: Acute Interstitial Nephritis: Etiology, Pathogenesis, Diagnosis, Treatment and Prognosism29hereNo ratings yet
- Eosinophilic Meningitis Due To Angiostrongylus Cantonensis in GermanyDocument3 pagesEosinophilic Meningitis Due To Angiostrongylus Cantonensis in GermanyjohndeereNo ratings yet
- Immunoglobulin A (Iga) Vasculitis in The ElderlyDocument4 pagesImmunoglobulin A (Iga) Vasculitis in The ElderlyAlexis CandoNo ratings yet
- Acute Bacterial ParotitisDocument3 pagesAcute Bacterial ParotitisPatrick JimenezNo ratings yet
- Journal of Orthopaedics, Trauma and Rehabilitation: Case ReportDocument2 pagesJournal of Orthopaedics, Trauma and Rehabilitation: Case ReportStephanie HellenNo ratings yet
- Radiology Case Report - Splenic AbscessDocument6 pagesRadiology Case Report - Splenic AbscessAbeebNo ratings yet
- Immunology of Idiopathic Nephrotic Syndrome: ReviewDocument12 pagesImmunology of Idiopathic Nephrotic Syndrome: ReviewDung TranNo ratings yet
- Art-9-Nk CitometriaDocument19 pagesArt-9-Nk CitometriaKAREN GARZA NEVAREZNo ratings yet
- Primary Psoas Abscess: Alexandru Crisan, Emilia Nicoara, Karina Bota, Doru BordosDocument3 pagesPrimary Psoas Abscess: Alexandru Crisan, Emilia Nicoara, Karina Bota, Doru BordosNataliaMaedyNo ratings yet
- Estenosis Esofagica en LlaDocument3 pagesEstenosis Esofagica en LlaResidencia PediatriaNo ratings yet
- Case Report of Acute and Chronic Interstitial NephritisDocument10 pagesCase Report of Acute and Chronic Interstitial NephritisDoncyNo ratings yet
- Tubercular ScleritisDocument5 pagesTubercular Scleritismutya yulindaNo ratings yet
- Elizabeth King I ADocument3 pagesElizabeth King I AAlba UrbinaNo ratings yet
- Streptokokni Toksični Šok SindromDocument6 pagesStreptokokni Toksični Šok SindromNandor SiliNo ratings yet
- Ofy 038Document5 pagesOfy 038Rosandi AdamNo ratings yet
- Complications of Sepsis in Infant. A Case ReportDocument4 pagesComplications of Sepsis in Infant. A Case ReportIntania RatnaNo ratings yet
- Infectious IleoceicitisDocument2 pagesInfectious IleoceicitisYandiNo ratings yet
- Seminars in Diagnostic Pathology: Jared R. Hassler TDocument5 pagesSeminars in Diagnostic Pathology: Jared R. Hassler TYamil FernandezNo ratings yet
- CorrespndenceDocument1 pageCorrespndenceTajul TajNo ratings yet
- Coxsackie UpdateDocument1 pageCoxsackie UpdateRahmiati LaoNo ratings yet
- A Case of Acute IdiopathicDocument19 pagesA Case of Acute IdiopathicSAIMA BATOOLNo ratings yet
- Toxic Shock SyndromeDocument13 pagesToxic Shock SyndromeSrinivas PingaliNo ratings yet
- Spina BifidaDocument5 pagesSpina BifidaQurratul AiniNo ratings yet
- Different Diagnostic Procedure of Typhoid Fever ADocument8 pagesDifferent Diagnostic Procedure of Typhoid Fever AdjebrutNo ratings yet
- Angiogenesis in PterygiumDocument7 pagesAngiogenesis in Pterygiumtest2012No ratings yet
- International Journal of Recent Scientific ResearchDocument5 pagesInternational Journal of Recent Scientific ResearchifahInayahNo ratings yet
- OsteomyelitisDocument32 pagesOsteomyelitisAndi Wija Indrawan PangerangNo ratings yet
- Osteomyelitis: Acute & ChronicDocument35 pagesOsteomyelitis: Acute & ChronicrainakenovNo ratings yet
- Acute Poststreptococcal Glomerulonephritis (Apsgn) in ChildrenDocument22 pagesAcute Poststreptococcal Glomerulonephritis (Apsgn) in ChildrenOlivia PutriNo ratings yet
- Acute Osteomyelitis in Choldren PathogenesisDocument8 pagesAcute Osteomyelitis in Choldren PathogenesisNurfitria Rahman PipitNo ratings yet
- Acute Epiglottitis in The Immunocompromised Host: Case Report and Review of The LiteratureDocument5 pagesAcute Epiglottitis in The Immunocompromised Host: Case Report and Review of The Literaturerosandi sabollaNo ratings yet
- Generalized Tetanus in A 4-Year Old Boy Presenting With Dysphagia and Trismus: A Case ReportDocument4 pagesGeneralized Tetanus in A 4-Year Old Boy Presenting With Dysphagia and Trismus: A Case Reportzul090No ratings yet
- Staphy 2Document5 pagesStaphy 2Alexandra MariaNo ratings yet
- Journal ToksoplasmosisDocument5 pagesJournal ToksoplasmosissibNo ratings yet
- Nepharites Lesson PlanDocument21 pagesNepharites Lesson Plansaritha Oruganti100% (1)
- Different Roles of Staphylococcus Aureus Enterotoxin in Different Subtypes of Nasal PolypsDocument6 pagesDifferent Roles of Staphylococcus Aureus Enterotoxin in Different Subtypes of Nasal PolypsSiq Febri SmnjtkNo ratings yet
- Management of HemophagocyticDocument10 pagesManagement of HemophagocyticAlexander CanoNo ratings yet
- Dafpus LiverDocument2 pagesDafpus LiverMenda JangWooyoung SooyoungsterNo ratings yet
- Acute Appendicitis in A Patient With Systemic Lupus ErythematosusDocument4 pagesAcute Appendicitis in A Patient With Systemic Lupus ErythematosusJessicaNo ratings yet
- Generalized Tetanus: Clinical Case Report and Review of The LiteratureDocument5 pagesGeneralized Tetanus: Clinical Case Report and Review of The LiteratureSebastian Orlando MedinaNo ratings yet
- Neonatal Tetanus After Home Delivery 2019Document4 pagesNeonatal Tetanus After Home Delivery 2019astutikNo ratings yet
- Juvenile Generalized Pustular Psoriasis: Ting XIAO, Bo LI, Chun-Di HE, Hong-Duo CHENDocument4 pagesJuvenile Generalized Pustular Psoriasis: Ting XIAO, Bo LI, Chun-Di HE, Hong-Duo CHENArya PambudiNo ratings yet
- Ovadia 2007Document7 pagesOvadia 2007uditNo ratings yet
- International Journal of Infectious DiseasesDocument3 pagesInternational Journal of Infectious DiseasesAnonymous sZFEEfNo ratings yet
- 1 s2.0 S1607551X09702748 MainDocument6 pages1 s2.0 S1607551X09702748 MainAbdul RaufNo ratings yet
- JurnalDocument9 pagesJurnalMelita Amalia AyubaNo ratings yet
- Understanding The Inflammatory Cytokine Response in Pneumonia and SepsisDocument9 pagesUnderstanding The Inflammatory Cytokine Response in Pneumonia and SepsisDennyNo ratings yet
- Short CommunicationDocument2 pagesShort CommunicationmarissapuenteshernandezNo ratings yet
- Zoster Sine HerpeteDocument7 pagesZoster Sine HerpeteLalo RCNo ratings yet
- Lee Et Al 2001 Case Report Meningococcal MeningitisDocument3 pagesLee Et Al 2001 Case Report Meningococcal MeningitisAsmae OuissadenNo ratings yet
- Pustular Psoriasis Complicated With Acute Generalized Exanthematous Pustulosis.Document4 pagesPustular Psoriasis Complicated With Acute Generalized Exanthematous Pustulosis.pancholarpancholarNo ratings yet
- AsdaDocument17 pagesAsdaRafif Abdurrahman WijisaksonoNo ratings yet
- A Compilation of Cellular and Tissue Xenotransplantation Studies (1838-2022): A Promising Approach for the Treatment of DiseasesFrom EverandA Compilation of Cellular and Tissue Xenotransplantation Studies (1838-2022): A Promising Approach for the Treatment of DiseasesNo ratings yet
- 16 Network Analysis McNally-2016-BRATDocument10 pages16 Network Analysis McNally-2016-BRATCeciliaNo ratings yet
- Hernia HiatalDocument4 pagesHernia HiatalFabrizioSanchezZegarraNo ratings yet
- Lateralizantes en Temporal PDFDocument5 pagesLateralizantes en Temporal PDFViviana Torres BallesterosNo ratings yet
- 9) Medical Complications of Drug TakingDocument44 pages9) Medical Complications of Drug TakingDr. Zirwa AsimNo ratings yet
- FR MaxillaDocument5 pagesFR MaxillaJeane SuyantoNo ratings yet
- AsssignmentDocument13 pagesAsssignmentMujahidNo ratings yet
- Onyx IFUDocument48 pagesOnyx IFUMamdooh AlqathamiNo ratings yet
- Architectural Design V: BY CHANCHAL SONI (00106142019) PALAK VERMA (02306142019) KAJAL PRAJAPATI (03406142019)Document11 pagesArchitectural Design V: BY CHANCHAL SONI (00106142019) PALAK VERMA (02306142019) KAJAL PRAJAPATI (03406142019)Chanchal SoniNo ratings yet
- Working at Height Rescue PlanDocument1 pageWorking at Height Rescue PlanAbbas AsadNo ratings yet
- Guillain Barre Syndrome: Molebatsi TheletsaneDocument16 pagesGuillain Barre Syndrome: Molebatsi TheletsaneSri KombongNo ratings yet
- Diabetic NephropathyDocument6 pagesDiabetic NephropathyZulfadliZulfadliNo ratings yet
- Hematology Sop (Revise 2023)Document8 pagesHematology Sop (Revise 2023)Jeffrey GaliciaNo ratings yet
- NN Drip ObatDocument7 pagesNN Drip ObatDioniivanNo ratings yet
- Jadwal Atls Online 12 Juni 21, JKTDocument3 pagesJadwal Atls Online 12 Juni 21, JKTTedja PrakosoNo ratings yet
- Hepar Sulph - The Homeopathic AntibioticDocument54 pagesHepar Sulph - The Homeopathic AntibioticGer DersenNo ratings yet
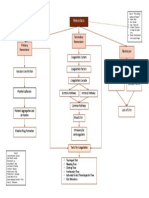
- B4M1 Case 2 My Concept MapDocument1 pageB4M1 Case 2 My Concept MapMabuhigh ErnieNo ratings yet
- A Time and A Place: What People Want Atthe End of LifeDocument52 pagesA Time and A Place: What People Want Atthe End of LifeSue RyderNo ratings yet
- Telerehab in Covid and CopdDocument13 pagesTelerehab in Covid and CopdNelson LoboNo ratings yet
- Sindroma KlinefelterDocument27 pagesSindroma KlinefelterSamuelRexyNo ratings yet
- Interview Questions AutosavedDocument8 pagesInterview Questions Autosavedapi-296945889No ratings yet
- Early and Late Preeclamsia Are Characterized by High Cardiac Output, But in The Presence of Fetal Growth Restriction, Cardiac Output Is Low Insights From A Prospective Study PDFDocument12 pagesEarly and Late Preeclamsia Are Characterized by High Cardiac Output, But in The Presence of Fetal Growth Restriction, Cardiac Output Is Low Insights From A Prospective Study PDFJustiawan NazwanNo ratings yet
- Edna K.huffman - Health Information Managemen 1994Document36 pagesEdna K.huffman - Health Information Managemen 1994gspot967% (6)
- Book Mark Livre À La PageDocument1 pageBook Mark Livre À La PageAashish G. ShresthaNo ratings yet
- Bipolar DepressionDocument22 pagesBipolar DepressionAdairon Luvanor SuárezNo ratings yet
- Schedule y PPT EDITTED ONEDocument38 pagesSchedule y PPT EDITTED ONEKesetha100% (2)
- IGCS 2020 Final Program Book 9.10.20 IXDocument52 pagesIGCS 2020 Final Program Book 9.10.20 IXFeli FelNo ratings yet
- Tentative Program: World Mental Health CongressDocument5 pagesTentative Program: World Mental Health CongressAdamNo ratings yet
- Oral Ondansetron For Paediatric Gastroenteritis in Primary Care A Randomised Controlled TrialDocument8 pagesOral Ondansetron For Paediatric Gastroenteritis in Primary Care A Randomised Controlled TrialAssyifa LunaNo ratings yet
- Roles of Physiotherappist in ResuscitationDocument57 pagesRoles of Physiotherappist in Resuscitationabisinuola8No ratings yet