You might also like
- Barbell Medicine Beginner PrescriptionDocument15 pagesBarbell Medicine Beginner PrescriptionColton Tessener100% (3)
- 12 Cranial Nerves and AssessmentDocument10 pages12 Cranial Nerves and Assessmentapollo100% (17)
- How To Grow Dragon FruitDocument2 pagesHow To Grow Dragon FruitWrein B. RabanalNo ratings yet
- Uses of EpidemiologyDocument18 pagesUses of Epidemiologyshipra arora75% (4)
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptAnonymous 34F1q3ZEuaNo ratings yet
- Hutchinson 2010Document10 pagesHutchinson 2010pilarerasoNo ratings yet
- Bailey 2019 Oi 190241Document13 pagesBailey 2019 Oi 190241Risma Ripfandiana SariNo ratings yet
- Vitamin D Intake and Risk of Cardiovascular Disease in US Men and WomenDocument9 pagesVitamin D Intake and Risk of Cardiovascular Disease in US Men and WomenAgafioNo ratings yet
- Dairy Intake Is Not Associated With Improvements.8Document8 pagesDairy Intake Is Not Associated With Improvements.8indiz emotionNo ratings yet
- Nut in Clin Prac - 2023 - Rempel - Effects of The Use of Oral Nutrition Supplements On Clinical Outcomes Among Patients WhoDocument15 pagesNut in Clin Prac - 2023 - Rempel - Effects of The Use of Oral Nutrition Supplements On Clinical Outcomes Among Patients WhoAna RMNo ratings yet
- Ca Próstata & Dieta 2019 ShinDocument11 pagesCa Próstata & Dieta 2019 ShinLuis C Ribon VNo ratings yet
- Carotenoids, Vitamin A, Vitamin C, Vitamin E, and Folate and Risk of Self-Reported Hearing Loss in WomenDocument9 pagesCarotenoids, Vitamin A, Vitamin C, Vitamin E, and Folate and Risk of Self-Reported Hearing Loss in WomenTarisa Zahrah JinanNo ratings yet
- Vitaminsfinal HamrickCountsDocument43 pagesVitaminsfinal HamrickCountsĐặng Huy HoàngNo ratings yet
- Vitamin and Mineral Supplementation During PregnanDocument4 pagesVitamin and Mineral Supplementation During PregnanEvi RachmawatiNo ratings yet
- JACNDocument10 pagesJACNprabhaNo ratings yet
- Calcium Plus Vit D Supplementation and The Risk of FracturesDocument15 pagesCalcium Plus Vit D Supplementation and The Risk of FracturesRobin ScherbatskyNo ratings yet
- Calcium and Vitamin D Not AssociatedDocument7 pagesCalcium and Vitamin D Not AssociatedPia GayyaNo ratings yet
- Vitamin and Mineral Supplements 2018 JAMADocument2 pagesVitamin and Mineral Supplements 2018 JAMAjoao manoel100% (2)
- What Vitamins Should I Be Taking, DoctorDocument6 pagesWhat Vitamins Should I Be Taking, DoctorDiego Bedón AscurraNo ratings yet
- Pi Is 0749379702005718Document9 pagesPi Is 0749379702005718audrey angelicaNo ratings yet
- Evidence Based Recommendations For An Optimal Prenatal Supplement For Women in The US: Vitamins and Related NutrientsDocument37 pagesEvidence Based Recommendations For An Optimal Prenatal Supplement For Women in The US: Vitamins and Related Nutrientsines.queiros.nutricionistaNo ratings yet
- Dietary Protein Intake in Midlife in Relation To Healthy Aging - Results From The Prospective Nurses' Health StudyDocument12 pagesDietary Protein Intake in Midlife in Relation To Healthy Aging - Results From The Prospective Nurses' Health StudyInfo TradersNo ratings yet
- Shan. Association of Low-Carbohydrate and Low-Fat Diets With MortalityDocument20 pagesShan. Association of Low-Carbohydrate and Low-Fat Diets With MortalityMaria Julia Ogna EgeaNo ratings yet
- Safety and Efficacy of Supplements in Pregnancy: Lead ArticleDocument14 pagesSafety and Efficacy of Supplements in Pregnancy: Lead ArticleShahd AmjadNo ratings yet
- Risks and Benefits of Vegan and Vegetarian Diets in ChildrenDocument6 pagesRisks and Benefits of Vegan and Vegetarian Diets in ChildrenMostafa McheikNo ratings yet
- Vit & Miner SupplementationDocument5 pagesVit & Miner Supplementationbragaru.vladNo ratings yet
- Essentials of Healthy Eating: A Guide: Journal of Midwifery and Women?s Health November 2010Document18 pagesEssentials of Healthy Eating: A Guide: Journal of Midwifery and Women?s Health November 2010Shathish JaiNo ratings yet
- JNCI J Natl Cancer Inst 2008 Speers 1562 4Document3 pagesJNCI J Natl Cancer Inst 2008 Speers 1562 4Ramy Abo SamraNo ratings yet
- Role of Selected Vitamins in Women With Polycystic Ovarian Syndrome - Thi-Qar Governorate - IraqDocument7 pagesRole of Selected Vitamins in Women With Polycystic Ovarian Syndrome - Thi-Qar Governorate - IraqCentral Asian StudiesNo ratings yet
- Suplementacion Con Vit DDocument31 pagesSuplementacion Con Vit Dyanet guzman aybarNo ratings yet
- Jama Jia 2022 Ed 220043 1655316061.73925Document2 pagesJama Jia 2022 Ed 220043 1655316061.73925Michaell GabrielNo ratings yet
- J Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultDocument30 pagesJ Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultPabloNo ratings yet
- Artículo Tomer AvnonE-2Document6 pagesArtículo Tomer AvnonE-2S. M.No ratings yet
- Dietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner PDocument8 pagesDietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner Ppaulobrasil.ortopedistaNo ratings yet
- Nuab 044Document14 pagesNuab 044pablo.s4672No ratings yet
- Knowledge, Attitude and Practice Study Regarding Anemia in Antenatal WomenDocument3 pagesKnowledge, Attitude and Practice Study Regarding Anemia in Antenatal WomenanggiNo ratings yet
- Safety of High-Dose Vitamin D Supplementation Among Children Aged 0 To 6 Years A Systematic Review and Meta-AnalysisDocument14 pagesSafety of High-Dose Vitamin D Supplementation Among Children Aged 0 To 6 Years A Systematic Review and Meta-AnalysisErisha Mae BalagbaganNo ratings yet
- Rickets: Not A Disease of The Past: American Family Physician September 2006Document9 pagesRickets: Not A Disease of The Past: American Family Physician September 2006mutmainnahNo ratings yet
- Vitamin DDocument11 pagesVitamin DCastiglianoNo ratings yet
- ASPEN - Suplemental Parenteral Nutrition - Review of The Literature and Current Nutriton GuidelinesDocument11 pagesASPEN - Suplemental Parenteral Nutrition - Review of The Literature and Current Nutriton GuidelinesRoberto Cárdenas GarcíaNo ratings yet
- Vitamin D ViewpointDocument2 pagesVitamin D ViewpointRenan Lopez ViañaNo ratings yet
- Malnutrition and Associated Disorders Among Pregnant Women in Keranigonj, BangladeshDocument10 pagesMalnutrition and Associated Disorders Among Pregnant Women in Keranigonj, BangladeshAlejandra SalcedoNo ratings yet
- Vitamin D Supplementation and Incident Preeclampsia: A Systematic Review and Meta-Analysis of Randomized Clinical TrialsDocument11 pagesVitamin D Supplementation and Incident Preeclampsia: A Systematic Review and Meta-Analysis of Randomized Clinical TrialsHeidy R. SabaterNo ratings yet
- Health Effects of Vegan DietsDocument8 pagesHealth Effects of Vegan DietsJean-François AsselinNo ratings yet
- Nutrients 15 03239 v2Document15 pagesNutrients 15 03239 v2arina fatharaniNo ratings yet
- The Benefits and Concerns Related To Vitamin A SupplementationDocument4 pagesThe Benefits and Concerns Related To Vitamin A SupplementationAfla BahirahNo ratings yet
- Nutrition Assessment, Counseling, and Support Interventions To Improve Health-Related Outcomes in People Living With HIV/AIDS: A Systematic Review of The LiteratureDocument10 pagesNutrition Assessment, Counseling, and Support Interventions To Improve Health-Related Outcomes in People Living With HIV/AIDS: A Systematic Review of The LiteratureAken LarasatiNo ratings yet
- Update On Vegetarian and Vegan Athletes: A ReviewDocument11 pagesUpdate On Vegetarian and Vegan Athletes: A ReviewAlejandra AstorgaNo ratings yet
- Low-Fat or Low-Carb Diet: Does It Make A Difference?Document17 pagesLow-Fat or Low-Carb Diet: Does It Make A Difference?lapistoleroNo ratings yet
- PIIS2589790X23003232Document10 pagesPIIS2589790X23003232tomniucNo ratings yet
- Anemia Ebsco6Document14 pagesAnemia Ebsco6tantriNo ratings yet
- Am J Clin Nutr 1999 Feskanich 74 9 Vitamin KDocument6 pagesAm J Clin Nutr 1999 Feskanich 74 9 Vitamin KSeLpI NoFianINo ratings yet
- A Prospective Study of Carotenoid and Vitamin A Intakes and Risk of Cataract Extraction in US WomenDocument8 pagesA Prospective Study of Carotenoid and Vitamin A Intakes and Risk of Cataract Extraction in US WomenAfla BahirahNo ratings yet
- Ea 51 Pustaka Tamb 7 Anwar Karbohidrat Nihms285117Document16 pagesEa 51 Pustaka Tamb 7 Anwar Karbohidrat Nihms285117fathimzahroNo ratings yet
- Term Paper Elc550Document21 pagesTerm Paper Elc550Aina SofiaNo ratings yet
- 2022 - The Importance of Nutrition in Pregnancy and Lactation - Lifelong ConsequencesDocument26 pages2022 - The Importance of Nutrition in Pregnancy and Lactation - Lifelong ConsequencesjacquelineNo ratings yet
- Original Communication: Diet During Pregnancy in Relation To Maternal Weight Gain and Birth SizeDocument7 pagesOriginal Communication: Diet During Pregnancy in Relation To Maternal Weight Gain and Birth SizeMuhKalenggoNo ratings yet
- Guía Integradora 4Document3 pagesGuía Integradora 4Constanza GarcíaNo ratings yet
- Dietary Fat and Risk of Renal Cell Carcinoma in The Usa A Casecontrol StudyDocument11 pagesDietary Fat and Risk of Renal Cell Carcinoma in The Usa A Casecontrol StudyMarko Sanja StikovicNo ratings yet
- Asam FolatDocument8 pagesAsam FolatWanda AprilliaNo ratings yet
- Assessment of Pregnant Women's Knowledge, Attitude, and Practice Regarding Pregnancy Nutrition at A Tertiary Care HospitalDocument6 pagesAssessment of Pregnant Women's Knowledge, Attitude, and Practice Regarding Pregnancy Nutrition at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Article Relationship Between Dietary Vitamin D and Stroke and Coronary DiseaseDocument4 pagesArticle Relationship Between Dietary Vitamin D and Stroke and Coronary DiseaseJuan A. RodriguezNo ratings yet
- Vitamin A Deficiency in Human Immunodeficiency Virus Type-1 Infected and Un-Infected Pregnant Women in KPK, PakistanDocument7 pagesVitamin A Deficiency in Human Immunodeficiency Virus Type-1 Infected and Un-Infected Pregnant Women in KPK, PakistanOpenaccess Research paperNo ratings yet
- Gastrointestinal and Liver Disorders in Women’s Health: A Point of Care Clinical GuideFrom EverandGastrointestinal and Liver Disorders in Women’s Health: A Point of Care Clinical GuidePoonam Beniwal-PatelNo ratings yet
- Review ArticleDocument20 pagesReview Articleaeroforce20No ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: Sciencedirectaeroforce20No ratings yet
- Journal Pre-Proof: Medicine in Novel Technology and DevicesDocument40 pagesJournal Pre-Proof: Medicine in Novel Technology and Devicesaeroforce20No ratings yet
- Bone Reports: A A B C C B CDocument9 pagesBone Reports: A A B C C B Caeroforce20No ratings yet
- First Aid Level 1 Learner Guide 2014Document94 pagesFirst Aid Level 1 Learner Guide 2014Ndaba ZamsNo ratings yet
- Retinal Diseases George Pile, MD: RetinaDocument5 pagesRetinal Diseases George Pile, MD: RetinaPrincess Cate MercadoNo ratings yet
- Case of InfertilityDocument4 pagesCase of InfertilityVirag PatilNo ratings yet
- Neonatal Tooth With Riga-Fide Disease Affecting Breastfeeding: A Case ReportDocument4 pagesNeonatal Tooth With Riga-Fide Disease Affecting Breastfeeding: A Case ReportbanyubiruNo ratings yet
- Task 2Document8 pagesTask 2Chin Jia YiNo ratings yet
- Measures of Diagnostic Accuracy: Basic Definitions: Ana-Maria ŠimundićDocument9 pagesMeasures of Diagnostic Accuracy: Basic Definitions: Ana-Maria ŠimundićgangjothelancerNo ratings yet
- Acute Scrotal Swelling & Pain in ChildrenDocument58 pagesAcute Scrotal Swelling & Pain in ChildrenalaaNo ratings yet
- Health Problems Common in ToddlersDocument4 pagesHealth Problems Common in ToddlersKim_b_Serac_6246No ratings yet
- CHCAGE001 PPSlides V1.0Document86 pagesCHCAGE001 PPSlides V1.0Leanne EvansNo ratings yet
- Reading Section The Following Text Is For Questions No AnnouncementDocument9 pagesReading Section The Following Text Is For Questions No AnnouncementcutamaNo ratings yet
- Case Digest No. 2 PDFDocument2 pagesCase Digest No. 2 PDFAngel Khaille SagubanNo ratings yet
- Group 5 (HIV&AIDS - BPA1A)Document23 pagesGroup 5 (HIV&AIDS - BPA1A)CindyNo ratings yet
- Semiology Study AidDocument87 pagesSemiology Study AidForró Anna-BíborkaNo ratings yet
- Dissertation Topics in Rajiv Gandhi University of Health SciencesDocument7 pagesDissertation Topics in Rajiv Gandhi University of Health SciencesWhereCanIFindSomeoneToWriteMyPaperNewarkNo ratings yet
- Slow Deep BreathingDocument17 pagesSlow Deep BreathingpluigiaNo ratings yet
- Alexis - Protector-Retractor PlagaDocument8 pagesAlexis - Protector-Retractor PlagaMarius NenciuNo ratings yet
- 10.7556 Jaoa.2015.022Document5 pages10.7556 Jaoa.2015.022CarolinaNo ratings yet
- Cervical Cancer Differential DiagnosesDocument8 pagesCervical Cancer Differential DiagnosesDebi SumarliNo ratings yet
- Physical Education 10 - Learning MaterialDocument54 pagesPhysical Education 10 - Learning MaterialAnngela Arevalo BarcenasNo ratings yet
- Mid A AssignmentDocument24 pagesMid A AssignmentTHE HOWDAY COMPANYNo ratings yet
- Marie Curie: Facts & BiographyDocument2 pagesMarie Curie: Facts & BiographyMaría Del A. VargasNo ratings yet
- Perianesthetic ArrhythmiasDocument10 pagesPerianesthetic Arrhythmiastaner_soysurenNo ratings yet
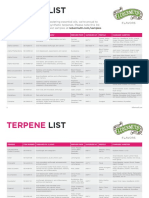
- Lebermuth Terpenes List 2019Document4 pagesLebermuth Terpenes List 2019EdoardoNo ratings yet
- Biology Investigatory ProjectDocument19 pagesBiology Investigatory ProjectSenthil KumarNo ratings yet
- Chapter 024wong S Essentials of Pediatrics Test BankDocument21 pagesChapter 024wong S Essentials of Pediatrics Test BankLLLJJJNo ratings yet
- 02-05-15 EditionDocument28 pages02-05-15 EditionSan Mateo Daily JournalNo ratings yet