You might also like
- Kavanaugh, Stephen P. - Rafferty, Kevin D - Geothermal Heating and Cooling - Design of Ground-Source Heat Pump Systems (2014, ASHRAE) PDFDocument442 pagesKavanaugh, Stephen P. - Rafferty, Kevin D - Geothermal Heating and Cooling - Design of Ground-Source Heat Pump Systems (2014, ASHRAE) PDFramchanduri100% (1)
- Digital SAT Preview: What to Expect + Tips and StrategiesFrom EverandDigital SAT Preview: What to Expect + Tips and StrategiesRating: 5 out of 5 stars5/5 (3)
- Lead and Manage Team EffectivenessDocument52 pagesLead and Manage Team EffectivenessSamina AkhtarNo ratings yet
- Assignment 1Document2 pagesAssignment 1ramchanduriNo ratings yet
- Assignment 1Document2 pagesAssignment 1ramchanduriNo ratings yet
- Lead and Manage Effective Workplace RelationshipDocument43 pagesLead and Manage Effective Workplace RelationshipSamina Akhtar100% (1)
- FEA TheoryDocument49 pagesFEA Theoryof_switzerlandNo ratings yet
- MEXT Research 2016Document18 pagesMEXT Research 2016bea garciaNo ratings yet
- Registration Forms Course Substitute Request enDocument2 pagesRegistration Forms Course Substitute Request enFarhan DanyNo ratings yet
- Corrected Quiz and Exam Distribution SheetDocument1 pageCorrected Quiz and Exam Distribution SheetKristin ManaigNo ratings yet
- Federal Public Service Commission: Aga Khan Road, Sector F-5/ 1, ISLAMABADDocument3 pagesFederal Public Service Commission: Aga Khan Road, Sector F-5/ 1, ISLAMABADshahid hussainNo ratings yet
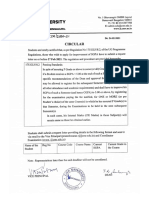
- Circular: This Is A Computer System (Digital File) Generated Letter. Hence There Is No Need For A Physical SignatureDocument3 pagesCircular: This Is A Computer System (Digital File) Generated Letter. Hence There Is No Need For A Physical SignatureRahul S.KumarNo ratings yet
- LLB Paper PatternDocument6 pagesLLB Paper PatternRutuparna SonawaneNo ratings yet
- Eee 423 50D EeeDocument21 pagesEee 423 50D EeeForhadi TechNo ratings yet
- PHD Vacancy 2018-19Document13 pagesPHD Vacancy 2018-19FaheemNo ratings yet
- Electrical Engineering Program: Aims and Scope of The Graduate ProgramDocument14 pagesElectrical Engineering Program: Aims and Scope of The Graduate ProgramAth SydNo ratings yet
- Facilitate Continuous ImprovementDocument58 pagesFacilitate Continuous ImprovementSamina AkhtarNo ratings yet
- Instant Notification 09-02-2023Document1 pageInstant Notification 09-02-2023amarnadhattiliNo ratings yet
- Regulations Governing The Degree of Bachelor of Engineering / TechnologyDocument7 pagesRegulations Governing The Degree of Bachelor of Engineering / TechnologyKhushboo ChaudharyNo ratings yet
- APJ Abdul Kalam Technological University Thiruvananthapuram: Academic SectionDocument4 pagesAPJ Abdul Kalam Technological University Thiruvananthapuram: Academic SectionkayyurNo ratings yet
- TENTATIVE LOAD FORM-online - CABIAZA-ChEDocument2 pagesTENTATIVE LOAD FORM-online - CABIAZA-ChEMa Theresa CabiazaNo ratings yet
- Guidelines 2021Document2 pagesGuidelines 2021RehaanNo ratings yet
- Pre-Enrolment Evaluation / Study Load Form 2 Sem SY 2020-2021Document2 pagesPre-Enrolment Evaluation / Study Load Form 2 Sem SY 2020-2021Kent Benedict CabucosNo ratings yet
- You Are BabeDocument6 pagesYou Are BabeAM OfficialNo ratings yet
- Brochure MSC 2017Document2 pagesBrochure MSC 2017Chiranjaya HulangamuwaNo ratings yet
- WWW - Fpsc.gov - PK FPSC@FPSC - Gov.pk: Computer ScienceDocument3 pagesWWW - Fpsc.gov - PK FPSC@FPSC - Gov.pk: Computer ScienceJawaid Ali MangnejoNo ratings yet
- 3090 2023 KtuDocument2 pages3090 2023 KtuRoshiya FathimaNo ratings yet
- Be ExtcDocument132 pagesBe ExtcShailaja UdtewarNo ratings yet
- Master of Structural Engineering and ConstructionDocument4 pagesMaster of Structural Engineering and ConstructionalfrobiwongytNo ratings yet
- New FDP Under Cbcs System - Amendment-Exclude Attendance in CE - 2020UODocument3 pagesNew FDP Under Cbcs System - Amendment-Exclude Attendance in CE - 2020UOvishnuNo ratings yet
- Adobe Scan 06-Mar-2022Document1 pageAdobe Scan 06-Mar-2022Tushar DasNo ratings yet
- Course No.: Students (Yr/Course/Sec) : Term: - Sem, SY 20 - 20 - , Summer - Course Description: Type of Class (Lec/Lab) : Day/Time: RoomDocument52 pagesCourse No.: Students (Yr/Course/Sec) : Term: - Sem, SY 20 - 20 - , Summer - Course Description: Type of Class (Lec/Lab) : Day/Time: RoomJohn Mark Fernandez DanlagNo ratings yet
- Class Record - Kim NEWDocument52 pagesClass Record - Kim NEWJohn Mark Fernandez DanlagNo ratings yet
- B. A. Economics and Mathematics (149) 2. B. Sc. Mathematics and Computer ApplicationDocument5 pagesB. A. Economics and Mathematics (149) 2. B. Sc. Mathematics and Computer ApplicationSonia SabuNo ratings yet
- PG II Semester NotificationDocument2 pagesPG II Semester NotificationsureshNo ratings yet
- Drugs Used in AnimalsDocument1 pageDrugs Used in AnimalsM.Aleem khanNo ratings yet
- UG Semester-VI (Regular - Backlog) Semester-II & IV (Backlog) Examination Notification May-2022Document3 pagesUG Semester-VI (Regular - Backlog) Semester-II & IV (Backlog) Examination Notification May-2022Haseeb RahmanNo ratings yet
- 66 - Kakinada Inst. of Engg. & Tech - IIDocument3 pages66 - Kakinada Inst. of Engg. & Tech - IIMogili sivaNo ratings yet
- Unit 5 Im Module in ConstructionDocument45 pagesUnit 5 Im Module in ConstructionHasmien Porpayas SangcoNo ratings yet
- Assignment Cover Page - 2Document1 pageAssignment Cover Page - 2Lutfi RaziqNo ratings yet
- CE of KTU Updated RulesDocument3 pagesCE of KTU Updated RulesbinzbinzNo ratings yet
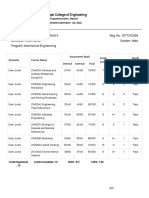
- Print Sem Result 1Document2 pagesPrint Sem Result 1Krissh KrisshNo ratings yet
- Print Sem 3Document2 pagesPrint Sem 3Krissh KrisshNo ratings yet
- Notice 2021 03 24 102844Document134 pagesNotice 2021 03 24 102844Aditya SinghNo ratings yet
- APJ Abdul Kalam Technological University Thiruvananthapuram: Academic SectionDocument2 pagesAPJ Abdul Kalam Technological University Thiruvananthapuram: Academic SectionAthira RaghavanNo ratings yet
- Shri Vaishnav Vidyapeeth Vishwavidyalaya, Indore: Name of Program: B.TECH (Textile Engineering)Document1 pageShri Vaishnav Vidyapeeth Vishwavidyalaya, Indore: Name of Program: B.TECH (Textile Engineering)Daddy PapaNo ratings yet
- Registration in Vancouver CoursesDocument1 pageRegistration in Vancouver CoursesramchanduriNo ratings yet
- KSRMCE Registration-Form-NPTEL R20UG - OEDocument2 pagesKSRMCE Registration-Form-NPTEL R20UG - OEVenkata Subbaiah Mamilla CNo ratings yet
- Federal Public Service Commission: Aga Khan Road, Sector F-5/1, ISLAMABADDocument3 pagesFederal Public Service Commission: Aga Khan Road, Sector F-5/1, ISLAMABADKashif NiaziNo ratings yet
- Sandeep AicteDocument13 pagesSandeep AictePunit RonadNo ratings yet
- Screenshot 2021-02-27 at 3.52.11 PMDocument1 pageScreenshot 2021-02-27 at 3.52.11 PMM NIKHIL SAI 17BBLB026No ratings yet
- Gogte Institute of Technology: Karnatak Law Society'SDocument27 pagesGogte Institute of Technology: Karnatak Law Society'Samit malaghanNo ratings yet
- Gogte Institute of Technology: Karnatak Law Society'SDocument27 pagesGogte Institute of Technology: Karnatak Law Society'ShiriyiNo ratings yet
- BCA Part-II (Semester III & IV)Document24 pagesBCA Part-II (Semester III & IV)Sukhwinder singhNo ratings yet
- 3 Years LLB and 5 Years B.A. LLB. I Semester Notification PDFDocument1 page3 Years LLB and 5 Years B.A. LLB. I Semester Notification PDFbharath palacharlaNo ratings yet
- 3 Years LLB and 5 Years B.A. LLB. I Semester NotificationDocument1 page3 Years LLB and 5 Years B.A. LLB. I Semester Notificationbharath palacharlaNo ratings yet
- Faculty of Engineering Department of Civil Engineering Course OutlineDocument4 pagesFaculty of Engineering Department of Civil Engineering Course OutlineUcchash AzizNo ratings yet
- Malpractice Committee ResolutionsDocument6 pagesMalpractice Committee Resolutionsrahinbegum9440No ratings yet
- TENTATIVE LOAD FORM-onlineDocument3 pagesTENTATIVE LOAD FORM-onlineKent Benedict CabucosNo ratings yet
- University of Kerala University of KeralaDocument2 pagesUniversity of Kerala University of Keralamaneesh sNo ratings yet
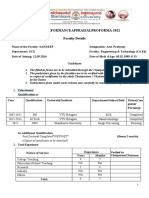
- Zuhaib-Faculty Course Review ReportDocument2 pagesZuhaib-Faculty Course Review ReportMohammad Zohaib Khan Kamboh50% (2)
- All ECE Syllabus FinalDocument124 pagesAll ECE Syllabus FinalKrishna Chaitanya TNo ratings yet
- Kingdom of Saudi Arabia:: Jazan University: Final Examinations, May 2014Document12 pagesKingdom of Saudi Arabia:: Jazan University: Final Examinations, May 2014HIDAYAH IGCSENo ratings yet
- What Every Successful Physics Graduate Student Should KnowFrom EverandWhat Every Successful Physics Graduate Student Should KnowRating: 4 out of 5 stars4/5 (3)
- Registration in Vancouver CoursesDocument1 pageRegistration in Vancouver CoursesramchanduriNo ratings yet
- LogicDesign PDFDocument23 pagesLogicDesign PDFJhoanie Marie Cauan0% (1)
- Lect 1 Intro - 2020Document63 pagesLect 1 Intro - 2020ramchanduriNo ratings yet
- Balance Outstanding 0.00: Meter Reading Information Meter Number: 6074294Document1 pageBalance Outstanding 0.00: Meter Reading Information Meter Number: 6074294ramchanduriNo ratings yet
- Lecture 14 StudentDocument3 pagesLecture 14 StudentRama Kant ChandravanshiNo ratings yet
- PSET 3 MOS Logic Gates - QDocument4 pagesPSET 3 MOS Logic Gates - QramchanduriNo ratings yet
- MFF AssignemntDocument5 pagesMFF AssignemntramchanduriNo ratings yet
- The Enormous Potential For Hot Dry Rock Geothermal EnergyDocument25 pagesThe Enormous Potential For Hot Dry Rock Geothermal Energyandri julianNo ratings yet
- Lecture02 ConductionB 1d 2d Numerics PDFDocument23 pagesLecture02 ConductionB 1d 2d Numerics PDFramchanduriNo ratings yet
- 0.05 (3 Files Merged)Document3 pages0.05 (3 Files Merged)ramchanduriNo ratings yet
- Shell-And-Tube Heat Exchangers: Standard Series and Customer Oriented SolutionsDocument24 pagesShell-And-Tube Heat Exchangers: Standard Series and Customer Oriented SolutionsZewdu TsegayeNo ratings yet
- Kitegen: A Hope For The FutureDocument17 pagesKitegen: A Hope For The FutureramchanduriNo ratings yet
- Aerodynamics in CarsDocument20 pagesAerodynamics in CarsSagar KnNo ratings yet
- ParagraphsDocument1 pageParagraphsSolange CardonaNo ratings yet
- Chapter 4 Thesis Presentation and Analysis of DataDocument7 pagesChapter 4 Thesis Presentation and Analysis of Datavetepuwej1z3100% (2)
- Fenis, Dandy B. Eboña, Jerald D. de Los Santos, Benmar C. Despuig, Jerald C. Garbiles, Bornz Hemer TDocument13 pagesFenis, Dandy B. Eboña, Jerald D. de Los Santos, Benmar C. Despuig, Jerald C. Garbiles, Bornz Hemer TJasper Rex RamirezNo ratings yet
- Applied & Engineering Physics: Ph.D. Handbook 2012-2013Document11 pagesApplied & Engineering Physics: Ph.D. Handbook 2012-2013andrewsiby63No ratings yet
- The Most Efficient and Effective Ways To Address New Literacies FDocument61 pagesThe Most Efficient and Effective Ways To Address New Literacies FAlpha MoontonNo ratings yet
- Prospective ChemistryDocument10 pagesProspective ChemistryAdolfNo ratings yet
- In Aerospace Systems Navigation and Telecommunications MSC As-NatDocument2 pagesIn Aerospace Systems Navigation and Telecommunications MSC As-Natfunny_boyNo ratings yet
- Discovery For The HSC ExamDocument36 pagesDiscovery For The HSC ExamEren SevinceNo ratings yet
- Thesis Draft: THE DAMAGE CAUSED BY MANDATORY SENTENCINGDocument55 pagesThesis Draft: THE DAMAGE CAUSED BY MANDATORY SENTENCINGAlma CurrierNo ratings yet
- Student Thesis Proposal GuidelinesDocument6 pagesStudent Thesis Proposal GuidelineslublinerNo ratings yet
- #Sponsored - The Emergence of Influencer MarketingDocument26 pages#Sponsored - The Emergence of Influencer MarketingMiruna MihăilăNo ratings yet
- Department of Metallurgical and Materials Engineering Notice For M.Tech StudentsDocument2 pagesDepartment of Metallurgical and Materials Engineering Notice For M.Tech StudentsAmit Ranjan KumarNo ratings yet
- Table of ContentsDocument5 pagesTable of Contentsrachelmarasigan092701No ratings yet
- Check List While Submitting Thesis: (For Scrutiny)Document4 pagesCheck List While Submitting Thesis: (For Scrutiny)Sangeetha TharmarNo ratings yet
- War of Words and Music - Veterans Remember Tokyo RoseDocument217 pagesWar of Words and Music - Veterans Remember Tokyo RoseRON CHRISTIAN TE�ALANo ratings yet
- Thesis Writing GuideDocument8 pagesThesis Writing GuideMay Ann ToyokenNo ratings yet
- Marketing Research Question Papers MbaDocument6 pagesMarketing Research Question Papers Mbajicbmhrif100% (1)
- 12-CAD-CAM Modified by MR - Sanjay Kumar-11.9.2013 PDFDocument58 pages12-CAD-CAM Modified by MR - Sanjay Kumar-11.9.2013 PDFRajaReddyNo ratings yet
- Asmerom Tekle .Document296 pagesAsmerom Tekle .hana fentaNo ratings yet
- 06 ESKAS Will You Be My Supervisor 2024-2025 eDocument2 pages06 ESKAS Will You Be My Supervisor 2024-2025 eSufyanNo ratings yet
- MSC Human Resource Management PDFDocument8 pagesMSC Human Resource Management PDFAji AikutNo ratings yet
- HEC Approved Supervisor-DiscontinuedDocument6 pagesHEC Approved Supervisor-DiscontinuedAftab AhmadNo ratings yet
- MUET Scheme of WorkDocument8 pagesMUET Scheme of WorksharonsmkbbNo ratings yet
- TUMA Research Manual: Tumaini University MakumiraDocument50 pagesTUMA Research Manual: Tumaini University MakumiraEmmanuel Joseph KundaelNo ratings yet
- Final MBA 2019 Bylaws 21.10.19Document156 pagesFinal MBA 2019 Bylaws 21.10.19Faraz SiddiquiNo ratings yet
- Thesis Generator 1.0 University of PhoenixDocument8 pagesThesis Generator 1.0 University of Phoenixbk1xaf0p100% (1)
- Ornamentation of Italian Vocal Music of The Eighteenth Century AcDocument79 pagesOrnamentation of Italian Vocal Music of The Eighteenth Century AcCaio CesarNo ratings yet
- Roof Garden ThesisDocument8 pagesRoof Garden Thesisgj9ggjry100% (1)
- Spiritual Practices As A Strategic Management Approach Towards Holistic Success in Corporate WorldDocument258 pagesSpiritual Practices As A Strategic Management Approach Towards Holistic Success in Corporate WorldMarthaNo ratings yet