You might also like
- Hyper-Pigmentation Of The Skin A Simple Guide To The Condition, Treatment, And Related ConditionsFrom EverandHyper-Pigmentation Of The Skin A Simple Guide To The Condition, Treatment, And Related ConditionsRating: 5 out of 5 stars5/5 (3)
- Drug PDFDocument2 pagesDrug PDFSheryhan Tahir BayleNo ratings yet
- Drug PDFDocument2 pagesDrug PDFSheryhan Tahir BayleNo ratings yet
- DrugStudy - 01 02 24Document3 pagesDrugStudy - 01 02 24Laurente, Patrizja Ysabel B. BSN-2DNo ratings yet
- General Considerations For Topical PreparationsDocument6 pagesGeneral Considerations For Topical PreparationsOccamsRazorNo ratings yet
- OTC Dermatological Products: 1. Dermatitis 2. Sunburn SuntanDocument30 pagesOTC Dermatological Products: 1. Dermatitis 2. Sunburn SuntanEman AlshaikhNo ratings yet
- Metronidazole Drug StudyDocument4 pagesMetronidazole Drug StudyJC LumayaNo ratings yet
- 11 DermatitisDocument39 pages11 DermatitisLQYNo ratings yet
- Metode SOAP 1Document19 pagesMetode SOAP 1rahmaNo ratings yet
- 56-Topical Drugs Used in The Treatment of Skin DisordersDocument13 pages56-Topical Drugs Used in The Treatment of Skin DisordersMujeebNo ratings yet
- 07 DermatologyDocument93 pages07 Dermatologyreuel nareshNo ratings yet
- System Disorder ADDocument1 pageSystem Disorder ADSariahNo ratings yet
- Scabies Simplified CPGDocument3 pagesScabies Simplified CPGAliaSyafiqaNo ratings yet
- Drug StudyDocument8 pagesDrug StudyjeanecalvoNo ratings yet
- Skin NCPDocument3 pagesSkin NCPCay ObejeroNo ratings yet
- Atopic Dermatitis: Aaron Justin D. TingzonDocument23 pagesAtopic Dermatitis: Aaron Justin D. TingzonChi SamaniegoNo ratings yet
- Atopic DermatitisDocument11 pagesAtopic DermatitisBS3091No ratings yet
- Gentamycin Drug StudyDocument2 pagesGentamycin Drug StudyShin Guevara100% (3)
- AONBDocument4 pagesAONBNicole Rachelyn MartinNo ratings yet
- Aseptic Technique: Wound Assessment On A Patient (Open or Closed)Document4 pagesAseptic Technique: Wound Assessment On A Patient (Open or Closed)AbigailNo ratings yet
- ACLOVATE - ACLOMETASONE by SOVON SAMANTADocument7 pagesACLOVATE - ACLOMETASONE by SOVON SAMANTASovon SamantaNo ratings yet
- Scabies: Dr. Atul Jain MD, Dermatology, SR, Santosh Medical College, GhaziabadDocument38 pagesScabies: Dr. Atul Jain MD, Dermatology, SR, Santosh Medical College, GhaziabadMaria GharuNo ratings yet
- Metabolic Regulation Corticosteroid Diabetic and Thyroid Medication CardsDocument5 pagesMetabolic Regulation Corticosteroid Diabetic and Thyroid Medication CardsJamie O.No ratings yet
- Musni Theo Roi Ncm116a - DS MedwardDocument2 pagesMusni Theo Roi Ncm116a - DS Medwardjovert davidNo ratings yet
- Prophylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofDocument10 pagesProphylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofElle RosalesNo ratings yet
- Drug Name Mechanism of Action Indication / Contraindication Adverse Effect Nursing ResponsibilitiesDocument8 pagesDrug Name Mechanism of Action Indication / Contraindication Adverse Effect Nursing ResponsibilitiesSALWANo ratings yet
- Drug Name Mechanism of Action Indication / Contraindication Adverse Effect Nursing ResponsibilitiesDocument8 pagesDrug Name Mechanism of Action Indication / Contraindication Adverse Effect Nursing ResponsibilitiesSALWANo ratings yet
- Thioridazine Drug StudyDocument6 pagesThioridazine Drug Studyshadow gonzalez100% (1)
- DRUGSTUDYDocument8 pagesDRUGSTUDYWinnie Salazar AriolaNo ratings yet
- Antibiotik TopikalDocument55 pagesAntibiotik TopikalMusthafa Afif WardhanaNo ratings yet
- Ncp-Impaired S.i.-NavidasDocument4 pagesNcp-Impaired S.i.-NavidasFran LanNo ratings yet
- Drug Study PrednisoloneDocument2 pagesDrug Study Prednisoloneunnamed personNo ratings yet
- Clortrimazole Drug StudyDocument3 pagesClortrimazole Drug StudyJasmin NatocNo ratings yet
- Budesonide Drug Study WWW RNpedia ComDocument3 pagesBudesonide Drug Study WWW RNpedia ComYuuki Chitose (tai-kun)No ratings yet
- Drugs in Ophthalmic PracticesDocument4 pagesDrugs in Ophthalmic PracticesGireesn M KNo ratings yet
- Medical Ward Drug StudyDocument9 pagesMedical Ward Drug StudygorgeazNo ratings yet
- Initial Management:: First AidDocument6 pagesInitial Management:: First AidxerwaneNo ratings yet
- Covid19-Drug StudyDocument7 pagesCovid19-Drug StudynicoleNo ratings yet
- Drugs Affecting Respiratory SystemDocument19 pagesDrugs Affecting Respiratory SystemRuby Ann DimayugaNo ratings yet
- Pedia Drug StudyDocument3 pagesPedia Drug StudyAnna LaritaNo ratings yet
- Derma ADDocument49 pagesDerma ADFatima Marwa Teo MaghinayNo ratings yet
- Dermatological Pharmacology: Topical Agents: Key PointsDocument3 pagesDermatological Pharmacology: Topical Agents: Key PointsIsmail IbrahimNo ratings yet
- Patient M. G Drug 1 - Ob MaxDocument5 pagesPatient M. G Drug 1 - Ob MaxGrace MellaineNo ratings yet
- Drug NameDocument4 pagesDrug Namecheanne003No ratings yet
- Drug StudyDocument2 pagesDrug StudyJulia Michelle SerranoNo ratings yet
- Maryville NURS 623 ExamDocument14 pagesMaryville NURS 623 ExamWizzardNo ratings yet
- Impaired Skin IntegrityDocument3 pagesImpaired Skin IntegrityNeriz Pineda0% (1)
- Drug Study DexamethasoneDocument4 pagesDrug Study Dexamethasoneamal abdulrahmanNo ratings yet
- Drug Classification Action Indication Contraindication Adverse Effects Nursing Responsibilities Antifungal Agent BeforeDocument4 pagesDrug Classification Action Indication Contraindication Adverse Effects Nursing Responsibilities Antifungal Agent BeforeElizabeth Ivory ChuaNo ratings yet
- Silver Sulfadiazine Drug StudyDocument3 pagesSilver Sulfadiazine Drug StudyKenn Siasar100% (1)
- Topical Corticosteroids: HighlightsDocument3 pagesTopical Corticosteroids: HighlightsNico Handreas TiantoNo ratings yet
- Day 11 Rational Topical Treatment in Dermatology: VignetteDocument2 pagesDay 11 Rational Topical Treatment in Dermatology: VignetteHananya ManroeNo ratings yet
- Patient M. G Drug 1 - Ob MaxDocument5 pagesPatient M. G Drug 1 - Ob MaxGrace MellaineNo ratings yet
- Adiel Joy P. Calsa Drug Study March 9, 2022Document5 pagesAdiel Joy P. Calsa Drug Study March 9, 2022Adiel CalsaNo ratings yet
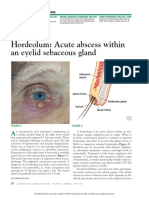
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Dur Sun 2019Document4 pagesDur Sun 2019Dayane GonçalvesNo ratings yet
- Drug StudyDocument9 pagesDrug StudyGenovee Angela FayeNo ratings yet
- Drug CardDocument1 pageDrug CardPaul AlfonsoNo ratings yet
- Insect BiteDocument53 pagesInsect BiteMuhammad AfiefNo ratings yet
- Prime-Hrm Performance Management System Coaching Guide (Grow Model) About The ModelDocument4 pagesPrime-Hrm Performance Management System Coaching Guide (Grow Model) About The Modelcory kurdapyaNo ratings yet
- DOC-2022-137 Add-Corr To DM-170-2022 DivCap IPBTDocument2 pagesDOC-2022-137 Add-Corr To DM-170-2022 DivCap IPBTcory kurdapyaNo ratings yet
- Meeting The Needs of All LearnersDocument2 pagesMeeting The Needs of All Learnerscory kurdapyaNo ratings yet
- PM Day 3Document104 pagesPM Day 3cory kurdapyaNo ratings yet
- Individual Development Plan: Strength Development Needs Action Plan Timeline Resources NeededDocument1 pageIndividual Development Plan: Strength Development Needs Action Plan Timeline Resources Neededcory kurdapyaNo ratings yet
- DOC-2022-120 DivCapBuild IPBT Implementation (DM-0170-2022)Document4 pagesDOC-2022-120 DivCapBuild IPBT Implementation (DM-0170-2022)cory kurdapyaNo ratings yet
- DOC-2022-136 DA Date and Venue of IPBT DivCap (DA-93-2022)Document1 pageDOC-2022-136 DA Date and Venue of IPBT DivCap (DA-93-2022)cory kurdapyaNo ratings yet
- ST - English 3 - Q1Document1 pageST - English 3 - Q1cory kurdapyaNo ratings yet
- Written Work No. 1 Quarter 1: Math 3Document4 pagesWritten Work No. 1 Quarter 1: Math 3Jazzele LongnoNo ratings yet
- The Latest Trends in Leadership Innovation I K-12 EducationDocument3 pagesThe Latest Trends in Leadership Innovation I K-12 Educationcory kurdapyaNo ratings yet
- Choose The Letter of The Best AnswerDocument3 pagesChoose The Letter of The Best AnswerRovieda ButacNo ratings yet
- 1.4 Integration of Trigonometric FunctionsDocument2 pages1.4 Integration of Trigonometric Functionscory kurdapyaNo ratings yet
- Grade 3 SumTest Answer Keys in All Subjets Modules 1-3Document8 pagesGrade 3 SumTest Answer Keys in All Subjets Modules 1-3cory kurdapyaNo ratings yet
- Math6 ST3 Q1Document2 pagesMath6 ST3 Q1cory kurdapyaNo ratings yet
- 9.2 The Chemistry of Natural WatersDocument3 pages9.2 The Chemistry of Natural Waterscory kurdapyaNo ratings yet
- 10.1 Properties of SoilDocument6 pages10.1 Properties of Soilcory kurdapyaNo ratings yet
- Chapter 6 - PolymersDocument123 pagesChapter 6 - Polymerscory kurdapyaNo ratings yet
- Unit 3 - The Chemistry of Engineering Materials Basic Concepts of Crystal StructuresDocument17 pagesUnit 3 - The Chemistry of Engineering Materials Basic Concepts of Crystal StructuresNiña Viaña BinayNo ratings yet
- LESSON 3: Air Pollution, Sources and Effects: Chapter 8: Chemistry of The AtmosphereDocument6 pagesLESSON 3: Air Pollution, Sources and Effects: Chapter 8: Chemistry of The Atmospherecory kurdapyaNo ratings yet
- 5.4 Solving Linear ODE Using TransformsDocument4 pages5.4 Solving Linear ODE Using Transformscory kurdapyaNo ratings yet
- CHAPTER 8: The Chemistry of The AtmosphereDocument2 pagesCHAPTER 8: The Chemistry of The Atmospherecory kurdapyaNo ratings yet
- CHAPTER 5: Metals: Main Group Al, Ga, In, SN, TL, PB, Bi, PoDocument5 pagesCHAPTER 5: Metals: Main Group Al, Ga, In, SN, TL, PB, Bi, Pocory kurdapyaNo ratings yet
- 1.2.1 Definitions in Nuclear ChemistryDocument2 pages1.2.1 Definitions in Nuclear Chemistrycory kurdapyaNo ratings yet
- 2.4 Basic Concepts of Crystal StructureDocument7 pages2.4 Basic Concepts of Crystal Structurecory kurdapyaNo ratings yet
- 2.4 Basic Concepts of Crystal StructureDocument7 pages2.4 Basic Concepts of Crystal Structurecory kurdapyaNo ratings yet
- Section 1: Definitions in Nuclear ChemistryDocument2 pagesSection 1: Definitions in Nuclear Chemistrycory kurdapyaNo ratings yet
- ST 2 Gr.6 Arts With TosDocument5 pagesST 2 Gr.6 Arts With Toshazel dileNo ratings yet
- Lesson 2: Understanding The World of Thermodynamics: Module 1: Energy Chapter 1: FuelsDocument4 pagesLesson 2: Understanding The World of Thermodynamics: Module 1: Energy Chapter 1: Fuelscory kurdapyaNo ratings yet
- 1.2.2 Types of Nuclear DecayDocument4 pages1.2.2 Types of Nuclear Decaycory kurdapyaNo ratings yet
- Objectives Code Percenta Ge No. of Items Item Placement: Guro Ako ChannelDocument3 pagesObjectives Code Percenta Ge No. of Items Item Placement: Guro Ako Channelcory kurdapyaNo ratings yet
- BIOLOGY Form 5 Chapter 1 TransportDocument42 pagesBIOLOGY Form 5 Chapter 1 TransportShephard Png91% (95)
- Paranoia Research PaperDocument50 pagesParanoia Research PaperNaina SinghNo ratings yet
- Benefits of Prana Mudra and How To Do It by Dr. Himani Bisht - PharmEasy BlogDocument7 pagesBenefits of Prana Mudra and How To Do It by Dr. Himani Bisht - PharmEasy BlogDanaNo ratings yet
- Dog BitesDocument14 pagesDog BitesNdor BariboloNo ratings yet
- PhysioFlow Non Invasive Hemodynamic Monitoring GeneralDocument28 pagesPhysioFlow Non Invasive Hemodynamic Monitoring GeneralPritam HiraNo ratings yet
- NICE Guidance On-Pre-Eclampsia VB2020Document40 pagesNICE Guidance On-Pre-Eclampsia VB2020nazem photocopyNo ratings yet
- 2 Chapter20 Pregnant With Preexisting IllnessDocument80 pages2 Chapter20 Pregnant With Preexisting IllnessElgen B. AgravanteNo ratings yet
- Project Proposal in P.E - Cheska ManiquisDocument11 pagesProject Proposal in P.E - Cheska ManiquisCheska MANIQUIS0% (1)
- 1307 Chest Tube Placement Procedure NoteDocument1 page1307 Chest Tube Placement Procedure NoteRumela Ganguly ChakrabortyNo ratings yet
- Biometry..Iol CalculationDocument86 pagesBiometry..Iol CalculationSristi Thakur0% (1)
- Antibacterial Mechanism of Lactic Acid On Physiological andDocument6 pagesAntibacterial Mechanism of Lactic Acid On Physiological andlox standardNo ratings yet
- Covid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaDocument6 pagesCovid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaIJAR JOURNALNo ratings yet
- CPG On AID PPT PresentationDocument83 pagesCPG On AID PPT Presentationsharmaine peroNo ratings yet
- TEACHERS' WORKPLACE - Physical Activity and Sedentary BehaviorDocument194 pagesTEACHERS' WORKPLACE - Physical Activity and Sedentary Behaviorhon jia shengNo ratings yet
- EMT Course NotesDocument88 pagesEMT Course NotesHunter RobertsNo ratings yet
- Nonsyndromic Delayed EruptionDocument3 pagesNonsyndromic Delayed EruptionRista LewiyonahNo ratings yet
- Psychiatric Tool FILIPINO VERSIOnDocument3 pagesPsychiatric Tool FILIPINO VERSIOnTeanu Jose Gabrillo TamayoNo ratings yet
- GHR Health and Nutrition Capacity Statement 2023Document5 pagesGHR Health and Nutrition Capacity Statement 2023Andre TorresNo ratings yet
- FLG 332 Renal Physiology-2 (2019)Document27 pagesFLG 332 Renal Physiology-2 (2019)Huzaifa KhanNo ratings yet
- Allergy and Oral Mucosal Disease: Shiona Rachel Rees B.D.S. F.D.S. R.C.P.SDocument440 pagesAllergy and Oral Mucosal Disease: Shiona Rachel Rees B.D.S. F.D.S. R.C.P.Sarya nugrahaNo ratings yet
- Sample Test Questions: Krok 2Document41 pagesSample Test Questions: Krok 2kjkNo ratings yet
- Chronic Pain SyndromeDocument1 pageChronic Pain SyndromeAdvance Pain CareNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritikBobby Fildian Siswanto100% (3)
- Fluids and Electrolytes2Document8 pagesFluids and Electrolytes2Potchiee PfizerNo ratings yet
- Reflective Paper SampleDocument1 pageReflective Paper SampleNur BilqisNo ratings yet
- 106 FinalsDocument27 pages106 FinalsCreciabullecerNo ratings yet
- Medicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgeryDocument70 pagesMedicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgerySTEPHANIE TANNo ratings yet
- Application of Eye Patch, Eye Shield and Pressure Dressing To The EyeDocument2 pagesApplication of Eye Patch, Eye Shield and Pressure Dressing To The EyeissaiahnicolleNo ratings yet
- Psoriasis in UnaniDocument15 pagesPsoriasis in UnaniAbdul Jalil HridoyNo ratings yet
- Introduction To Medical Virology 2023Document86 pagesIntroduction To Medical Virology 2023Samuel fikaduNo ratings yet