You might also like
- CHN 2 1-7 Formative Quiz #2B - NCM 113 - Community Health Nursing Ii - Population Groups andDocument5 pagesCHN 2 1-7 Formative Quiz #2B - NCM 113 - Community Health Nursing Ii - Population Groups andRegine CuntapayNo ratings yet
- CHN 2 1-4 FORMATIVE ASSESSMENT #1 - MCQ 15 Items + 5 Points DBP - Week 3 - NCM 113 - COMMUNITY HEALTH NURSING II - POPULATION GROUPS ANDDocument8 pagesCHN 2 1-4 FORMATIVE ASSESSMENT #1 - MCQ 15 Items + 5 Points DBP - Week 3 - NCM 113 - COMMUNITY HEALTH NURSING II - POPULATION GROUPS ANDRegine CuntapayNo ratings yet
- Chapter 12 Problem From Philosophy PDFDocument7 pagesChapter 12 Problem From Philosophy PDFRegine CuntapayNo ratings yet
- Assessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryDocument8 pagesAssessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryIJAR JOURNALNo ratings yet
- Experience of General Surgery Residents in The Creation of Small Bowel and Colon AnastomosesDocument7 pagesExperience of General Surgery Residents in The Creation of Small Bowel and Colon AnastomosesDiego Andres VasquezNo ratings yet
- The Comparison of Hand-Sewn and Stapled Anastomosis in EsophagectomyDocument4 pagesThe Comparison of Hand-Sewn and Stapled Anastomosis in EsophagectomyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Utilityofimage-Guidance Infrontalsinussurgery: Gretchen M. Oakley,, Henry P. Barham,, Richard J. HarveyDocument14 pagesUtilityofimage-Guidance Infrontalsinussurgery: Gretchen M. Oakley,, Henry P. Barham,, Richard J. HarveyJuan Pablo Mejia BarbosaNo ratings yet
- Fsurg 09 848565Document10 pagesFsurg 09 848565Jairo Farias OrtizNo ratings yet
- Gastrectomía LaparoscópicaDocument7 pagesGastrectomía LaparoscópicaGreyza VelazcoNo ratings yet
- International Journal of Radiology and Imaging Technology Ijrit 5 051Document7 pagesInternational Journal of Radiology and Imaging Technology Ijrit 5 051grace liwantoNo ratings yet
- Alesina Et Al., 2021Document9 pagesAlesina Et Al., 2021NyomantrianaNo ratings yet
- Long-Term Complications of Appendectomy: A Systematic ReviewDocument8 pagesLong-Term Complications of Appendectomy: A Systematic ReviewNurul Mukhlisah IsmailNo ratings yet
- Patient Reported Aesthetic Outcomes of Upper BlephDocument9 pagesPatient Reported Aesthetic Outcomes of Upper BlephRobertoNo ratings yet
- Journal of Clinical Orthopaedics and TraumaDocument5 pagesJournal of Clinical Orthopaedics and TraumaGaetano De BiaseNo ratings yet
- E8gklehwg'oirehtgrbjnag,/s" EIDocument6 pagesE8gklehwg'oirehtgrbjnag,/s" EIvenkayammaNo ratings yet
- Fonc 09 00597Document13 pagesFonc 09 00597Giann PersonaNo ratings yet
- With The Advance in The Techniques of Hemostasis Is It Necessary To Use Drain Routinely in Thyroid Surgery A Comparative StudyDocument8 pagesWith The Advance in The Techniques of Hemostasis Is It Necessary To Use Drain Routinely in Thyroid Surgery A Comparative StudyAthenaeum Scientific PublishersNo ratings yet
- Synthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairDocument9 pagesSynthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairRhuan AntonioNo ratings yet
- Julliard Worse Outcomes EVH 2011Document7 pagesJulliard Worse Outcomes EVH 2011Mary MoraNo ratings yet
- A Comparison of The Cost - Utility of Ultrasound-Guided High-Intensity Focused Ultrasound and Hysterectomy For Adenomyosis: A Retrospective StudyDocument6 pagesA Comparison of The Cost - Utility of Ultrasound-Guided High-Intensity Focused Ultrasound and Hysterectomy For Adenomyosis: A Retrospective StudyAgung SentosaNo ratings yet
- Endoscopically Access YANG - TMJ ProsthesisDocument6 pagesEndoscopically Access YANG - TMJ ProsthesisClínica BMFNo ratings yet
- Laparoscopic Vs Open Distal Pancreatectomy: A Single-Institution Comparative StudyDocument6 pagesLaparoscopic Vs Open Distal Pancreatectomy: A Single-Institution Comparative StudyHana YunikoNo ratings yet
- Single Incision Laparoscopic Appendicectomy Versus Conventional Laparoscopic Appendicectomy-A Prospective StudyDocument6 pagesSingle Incision Laparoscopic Appendicectomy Versus Conventional Laparoscopic Appendicectomy-A Prospective StudySabreen SaniaNo ratings yet
- 1 s2.0 S2405857220300218 MainDocument5 pages1 s2.0 S2405857220300218 MainIkea BalhonNo ratings yet
- Comparison PiezoDocument13 pagesComparison PiezoMiguel ChanNo ratings yet
- Dobnig 2020 Austria Thryoid RFA Guidelines s10354-019-0682-2Document9 pagesDobnig 2020 Austria Thryoid RFA Guidelines s10354-019-0682-2E cNo ratings yet
- Serarslan 2017Document5 pagesSerarslan 2017vistamaniacNo ratings yet
- Demographic Condylar HyperplasiaDocument9 pagesDemographic Condylar HyperplasiaLisdany BecerraNo ratings yet
- Iranjradiol 14 03 21742Document5 pagesIranjradiol 14 03 21742AisahNo ratings yet
- A Comparative Analysis of Total Thyroidectomy and Lobectomy As Surgical Approaches in Patients Undergoing Thyroid SurgeryDocument4 pagesA Comparative Analysis of Total Thyroidectomy and Lobectomy As Surgical Approaches in Patients Undergoing Thyroid SurgeryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Minimally Invasive Cardiac Surgery: A Safe Alternative For Aortic Valve Replacement?Document2 pagesMinimally Invasive Cardiac Surgery: A Safe Alternative For Aortic Valve Replacement?lkulacogluNo ratings yet
- Rajapandian 2018Document5 pagesRajapandian 2018DH SiriruiNo ratings yet
- Surgery For Glaucoma in Patients With Facial Port Wine MarkDocument6 pagesSurgery For Glaucoma in Patients With Facial Port Wine MarkPutri kartiniNo ratings yet
- Degenerative Meniscal Tears (Graaf Et Al 2019)Document7 pagesDegenerative Meniscal Tears (Graaf Et Al 2019)nsboyadzhievNo ratings yet
- 1-S2.0-S0039606022004056-Main 2Document6 pages1-S2.0-S0039606022004056-Main 2alihumoodhasanNo ratings yet
- Biswas2014 PDFDocument7 pagesBiswas2014 PDFDhruv MahajanNo ratings yet
- 10 1016@j Oooo 2020 03 048Document11 pages10 1016@j Oooo 2020 03 048Arthur CésarNo ratings yet
- Advantages and Limitations of Endoscopic Septoplasty Experience of 120 CasesDocument6 pagesAdvantages and Limitations of Endoscopic Septoplasty Experience of 120 CasesInternational Journal of Innovative Science and Research Technology100% (1)
- Advantage and Limitation of Endoscopic SepDocument6 pagesAdvantage and Limitation of Endoscopic SepTareq MohammadNo ratings yet
- Comparison of The Short-Term Outcomes of Using DST and PPH Staplers in The Treatment of Grade Iii and Iv HemorrhoidsDocument7 pagesComparison of The Short-Term Outcomes of Using DST and PPH Staplers in The Treatment of Grade Iii and Iv HemorrhoidsdianisaindiraNo ratings yet
- Ejo 1Document11 pagesEjo 1ayisNo ratings yet
- Fabio Febrian JurnalDocument3 pagesFabio Febrian JurnallarasatiNo ratings yet
- RAVARIDocument6 pagesRAVARIGenesis BiceraNo ratings yet
- FVVinObGyn 11 269Document29 pagesFVVinObGyn 11 269Noël ChannetonNo ratings yet
- Review of Surgical Techniques and Guide For Decision Making in The Treatment of Benign Parotid TumorsDocument15 pagesReview of Surgical Techniques and Guide For Decision Making in The Treatment of Benign Parotid Tumors9gps6jw28bNo ratings yet
- Is 9Document9 pagesIs 9intan juitaNo ratings yet
- Single Versus Multi-Incisional Video-Assisted Thoracic Surgery: A Systematic Review and Meta-AnalysisDocument12 pagesSingle Versus Multi-Incisional Video-Assisted Thoracic Surgery: A Systematic Review and Meta-AnalysisHendrikus Surya Adhi PutraNo ratings yet
- Lu 2019Document10 pagesLu 2019CAMILO ANDRÉS SABOGAL ARGUELLONo ratings yet
- International Journal of SurgeryDocument7 pagesInternational Journal of SurgeryJose Manuel Luna VazquezNo ratings yet
- A Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyDocument8 pagesA Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyIJAR JOURNALNo ratings yet
- Efficacy of EUS-RFA in Pancreatic Tumors: Is It Ready For Prime Time? A Systematic Review and Meta-AnalysisDocument9 pagesEfficacy of EUS-RFA in Pancreatic Tumors: Is It Ready For Prime Time? A Systematic Review and Meta-AnalysisRadinal MauludiNo ratings yet
- 107 246 1 PBDocument4 pages107 246 1 PBAnjali ThakurNo ratings yet
- Alganabi2021 Article SurgicalSiteInfectionAfterOpenDocument9 pagesAlganabi2021 Article SurgicalSiteInfectionAfterOpenWahyudhy SajaNo ratings yet
- Hypospadias SurveyDocument6 pagesHypospadias SurveyDevi Humairah IrawanNo ratings yet
- Novel Hemostatic Adhesive Powder For Nonvariceal Upper Gastrointestinal BleedingDocument5 pagesNovel Hemostatic Adhesive Powder For Nonvariceal Upper Gastrointestinal Bleedingrahul krishnanNo ratings yet
- Russell 2017Document6 pagesRussell 2017pancholin_9No ratings yet
- Comparison of Costs and Short-Term Clinical Outcomes of Per-Oral Endoscopic Myotomy and Laparoscopic Heller MyotomyDocument6 pagesComparison of Costs and Short-Term Clinical Outcomes of Per-Oral Endoscopic Myotomy and Laparoscopic Heller MyotomyDavids MarinNo ratings yet
- Medicina 59 01545 v2Document6 pagesMedicina 59 01545 v2materthaiNo ratings yet
- Injury: Kiran C. Mahabier, Lucas M.M. Vogels, Bas J. Punt, Gert R. Roukema, Peter Patka, Esther M.M. Van LieshoutDocument4 pagesInjury: Kiran C. Mahabier, Lucas M.M. Vogels, Bas J. Punt, Gert R. Roukema, Peter Patka, Esther M.M. Van LieshoutGabriel GolesteanuNo ratings yet
- Comparison of Long-Term Surgical Outcomes of Two-Muscle Surgery in Basic-Type Intermittent Exotropia: Bilateral Versus UnilateralDocument9 pagesComparison of Long-Term Surgical Outcomes of Two-Muscle Surgery in Basic-Type Intermittent Exotropia: Bilateral Versus UnilateralerwinNo ratings yet
- 11.1 AP Accuracy of Fine Needle Aspiration Cytology FNAC IDocument7 pages11.1 AP Accuracy of Fine Needle Aspiration Cytology FNAC IdrdivyeshgoswamiNo ratings yet
- TMP 99 BADocument6 pagesTMP 99 BAFrontiersNo ratings yet
- The SAGES Manual of Flexible EndoscopyFrom EverandThe SAGES Manual of Flexible EndoscopyPeter NauNo ratings yet
- Thesis 2 (Word)Document209 pagesThesis 2 (Word)Regine CuntapayNo ratings yet
- Evidence Based ActivityDocument3 pagesEvidence Based ActivityRegine CuntapayNo ratings yet
- Medical DetectivesDocument2 pagesMedical DetectivesRegine CuntapayNo ratings yet
- Critical Appraisal Checklist For Qualitative ResearchDocument4 pagesCritical Appraisal Checklist For Qualitative ResearchRegine CuntapayNo ratings yet
- Reconceptualising Relatedness in Education in Distanced' TimesDocument16 pagesReconceptualising Relatedness in Education in Distanced' TimesRegine CuntapayNo ratings yet
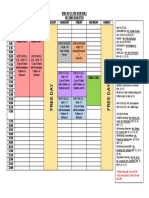
- BSN 303 Class Schedule Second Semester: (CE) - NCM 116 (CE) - NCM 116Document1 pageBSN 303 Class Schedule Second Semester: (CE) - NCM 116 (CE) - NCM 116Regine CuntapayNo ratings yet
- NUR 1218 Maladaptive Patterns of Behaviour LECTURE ONLY 2020 2021 - Dec26 - Ver1.0Document2 pagesNUR 1218 Maladaptive Patterns of Behaviour LECTURE ONLY 2020 2021 - Dec26 - Ver1.0Regine CuntapayNo ratings yet
- Master Rotation Plan of Level Iii (Areas: Geria, Medical Surgical, Psych Nursing)Document5 pagesMaster Rotation Plan of Level Iii (Areas: Geria, Medical Surgical, Psych Nursing)Regine CuntapayNo ratings yet
- Online Learning: A Panacea in The Time of COVID-19 Crisis: Shivangi DhawanDocument18 pagesOnline Learning: A Panacea in The Time of COVID-19 Crisis: Shivangi DhawanRegine CuntapayNo ratings yet
- Journal Pre-Proof: International Journal of Educational Research OpenDocument25 pagesJournal Pre-Proof: International Journal of Educational Research OpenRegine CuntapayNo ratings yet
- Review Articles: Acute AppendicitisDocument10 pagesReview Articles: Acute AppendicitisRegine CuntapayNo ratings yet
- Pedia Module Preschooler PDFDocument11 pagesPedia Module Preschooler PDFRegine CuntapayNo ratings yet
- Journal Pre-Proof: International Journal of Educational Research OpenDocument25 pagesJournal Pre-Proof: International Journal of Educational Research OpenRegine CuntapayNo ratings yet
- Teacher Stress Final Pre-Publication DraftDocument18 pagesTeacher Stress Final Pre-Publication DraftRegine CuntapayNo ratings yet
- Biochemistry ReviewerDocument4 pagesBiochemistry ReviewerRegine CuntapayNo ratings yet
- Delicacies Region 6Document2 pagesDelicacies Region 6Regine CuntapayNo ratings yet
- Traditional Open AppendectomyDocument14 pagesTraditional Open AppendectomyBayu NoviandaNo ratings yet
- Pathology of AppendixDocument26 pagesPathology of Appendixnovitafitri123No ratings yet
- The Surgical Examination of ChildrenDocument315 pagesThe Surgical Examination of ChildrenPatricia Beznea100% (1)
- GI Part 2 2016 StudentDocument131 pagesGI Part 2 2016 StudentDaniel RayNo ratings yet
- Appendicitis - ClinicalKeyDocument38 pagesAppendicitis - ClinicalKeyjpma2197No ratings yet
- AppendicitisDocument36 pagesAppendicitisPetro MyronovNo ratings yet
- Acute AppendicitisDocument1 pageAcute AppendicitisAllen AykayNo ratings yet
- 26 Sri Rahayu Oktaviani PDFDocument117 pages26 Sri Rahayu Oktaviani PDFReizhaeNo ratings yet
- PEROTONITISDocument68 pagesPEROTONITISChloie Marie RosalejosNo ratings yet
- Alinsangao, Nashwa N. BSN 3B - SIC (Pathogenesis & Life Threatening Pathways)Document5 pagesAlinsangao, Nashwa N. BSN 3B - SIC (Pathogenesis & Life Threatening Pathways)NASHWA NASLUN. ALINSANGAONo ratings yet
- Imaging in Acute Appendicitis: A Review: RK Jain, M Jain, CL Rajak, S Mukherjee, PP Bhattacharyya, MR ShahDocument10 pagesImaging in Acute Appendicitis: A Review: RK Jain, M Jain, CL Rajak, S Mukherjee, PP Bhattacharyya, MR ShahVidini Kusuma AjiNo ratings yet
- Legal Medicine CasesDocument138 pagesLegal Medicine Casesmuton20No ratings yet
- Abdominal Pains in Children Under 12Document5 pagesAbdominal Pains in Children Under 12clubsanatateNo ratings yet
- IcdDocument21 pagesIcdVicky AprizanoNo ratings yet
- Acute Appendicitis in Adults Diagnostic EvaluationDocument13 pagesAcute Appendicitis in Adults Diagnostic EvaluationjimdioNo ratings yet
- Managing Acute Abdominal Pain in Pediatric Patients: Current PerspectivesDocument9 pagesManaging Acute Abdominal Pain in Pediatric Patients: Current PerspectivesAnonymous h4SCPPayNo ratings yet
- Gastrointestinal PathologyDocument59 pagesGastrointestinal PathologybonadnadineNo ratings yet
- Appendicitis & Appendectomy: Jenny Juniora AjocDocument31 pagesAppendicitis & Appendectomy: Jenny Juniora AjocJenny AjocNo ratings yet
- Test 7: Appendicitis Definition and FactsDocument21 pagesTest 7: Appendicitis Definition and FactsRuhi RuhiNo ratings yet
- Approach To Abdominal PainDocument22 pagesApproach To Abdominal PainOmar AbdillahiNo ratings yet
- Acute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and ManagementDocument11 pagesAcute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and ManagementMishel Rodriguez GuzmanNo ratings yet
- Appendicitis ManuscriptDocument4 pagesAppendicitis Manuscriptkint manlangitNo ratings yet
- Diagnosis and Management of Acute AppendicitisDocument23 pagesDiagnosis and Management of Acute AppendicitisFadhilla R. MeutiaNo ratings yet
- Appendectomy Appendicitis Case Study1Document18 pagesAppendectomy Appendicitis Case Study1Los Devio100% (1)
- Unit - I AuditDocument12 pagesUnit - I AuditNirav BunhaNo ratings yet
- Williams Gynecology PDFDriveDocument25 pagesWilliams Gynecology PDFDriveKawaii Rjen-chanNo ratings yet
- Acute Perforated AppendicitisDocument7 pagesAcute Perforated AppendicitisS3V4_9154No ratings yet
- 3rd Year OSCE StationsDocument6 pages3rd Year OSCE StationsrutendonormamapurisaNo ratings yet
- Medical Surgical Nursing Exams BoardDocument36 pagesMedical Surgical Nursing Exams BoardCINDY� BELMESNo ratings yet
- Görker Sel - Practical Guide To Oral Exams in Obstetrics and Gynecology - Questions & Answers-Springer International Publishing (2020) PDFDocument318 pagesGörker Sel - Practical Guide To Oral Exams in Obstetrics and Gynecology - Questions & Answers-Springer International Publishing (2020) PDFMohammed Khaleeq100% (2)