You might also like
- Nclex Review Uworld (6515)Document137 pagesNclex Review Uworld (6515)whereswaldo007yahooc88% (8)
- PaclitaxelDocument3 pagesPaclitaxelMavy CantonNo ratings yet
- Bianca Mascorro Introductory Calligraphy GuideDocument4 pagesBianca Mascorro Introductory Calligraphy GuideArianneJulienaCervaniaAndrada50% (6)
- Community Health NursingDocument8 pagesCommunity Health NursingLloyd rafael100% (2)
- Case History, MSE and Rating Scales - in Psychological AssessmentDocument29 pagesCase History, MSE and Rating Scales - in Psychological Assessmentsu84No ratings yet
- Peptic UlcerDocument17 pagesPeptic UlcerAbdirahman HajiNo ratings yet
- AR - 09 13 - Guimaraes Quencer Part01Document7 pagesAR - 09 13 - Guimaraes Quencer Part01Fernando VerdeNo ratings yet
- NCM 112 MSN Prelim Topic 3 Care of Clients With Gastrointestinal DisordersDocument2 pagesNCM 112 MSN Prelim Topic 3 Care of Clients With Gastrointestinal DisordersKim Erida QuezonNo ratings yet
- Dysphagia Marking SchemeDocument5 pagesDysphagia Marking SchemeibmreadywriterNo ratings yet
- Surgery BCA Pancreas Stomach Mar 2020Document5 pagesSurgery BCA Pancreas Stomach Mar 2020Jojo MendozaNo ratings yet
- Lower GI System Infants: Caoili, Maria EstrelaDocument21 pagesLower GI System Infants: Caoili, Maria EstrelaanreilegardeNo ratings yet
- Peritoneal Reflection: AnatomyDocument27 pagesPeritoneal Reflection: AnatomySHINMEN TAKEZONo ratings yet
- Gi SurgDocument42 pagesGi Surgbob marleyNo ratings yet
- Fluoroscopic Investigations of The Gastrointestinal Tract: Pharynx, Oesophagus and StomachDocument36 pagesFluoroscopic Investigations of The Gastrointestinal Tract: Pharynx, Oesophagus and StomachSatish PaswanNo ratings yet
- Esophagus - 1Document27 pagesEsophagus - 1hussain AltaherNo ratings yet
- MBBS4 EXAM MSAT OSCE Preparation - Gold, Answers To Past ExamsDocument70 pagesMBBS4 EXAM MSAT OSCE Preparation - Gold, Answers To Past ExamsqmmuvsarhvjmfmrximNo ratings yet
- 1.76 (Surgery) Esophageal Atresia - GI ObstructionDocument13 pages1.76 (Surgery) Esophageal Atresia - GI ObstructionLeo Mari Go LimNo ratings yet
- Radiology of The AbdomenDocument19 pagesRadiology of The AbdomenShaktisila FatrahadyNo ratings yet
- Short Written Mock 2021 Mn1 - AnsweredDocument20 pagesShort Written Mock 2021 Mn1 - AnsweredMatthew NgNo ratings yet
- Barium StudyDocument34 pagesBarium StudyJahanavi JaluNo ratings yet
- Bowel OcclusionDocument4 pagesBowel OcclusionAndra BauerNo ratings yet
- UgiDocument61 pagesUgiandisibaNo ratings yet
- 1.39 (Surgery) Surgical Diseases of The EsophagusDocument8 pages1.39 (Surgery) Surgical Diseases of The EsophagusLeo Mari Go LimNo ratings yet
- A UGI (Blue Keyword Pyq)Document3 pagesA UGI (Blue Keyword Pyq)Irsyad SiddeeqNo ratings yet
- Presentacion GastrointestinalDocument228 pagesPresentacion GastrointestinalNb + XB = AVNo ratings yet
- 155 - B3 Sesi 1 Asisten 2015Document91 pages155 - B3 Sesi 1 Asisten 2015Luthfi AnshoriNo ratings yet
- TBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahDocument84 pagesTBL 3: Dysphagia: By: Anis, Aishah, Nubla, Hanafi, HidayahNadia RahimNo ratings yet
- من جامعة الأردن PDFDocument266 pagesمن جامعة الأردن PDFyousefNo ratings yet
- Surgery PancreasDocument11 pagesSurgery PancreasMATTHEW EARL MALUMAYNo ratings yet
- DI Abdomen P 102 189 PART 1 SEC 2Document88 pagesDI Abdomen P 102 189 PART 1 SEC 2tudoranluciana1No ratings yet
- Oesophagus - Lecture (1 & 2) SurgeryDocument27 pagesOesophagus - Lecture (1 & 2) Surgeryhussain AltaherNo ratings yet
- Sunday, 30 August 2020 1:54 PM: Whitcomb-D-NEJM-2006 PDFDocument2 pagesSunday, 30 August 2020 1:54 PM: Whitcomb-D-NEJM-2006 PDFMichelle De FreitasNo ratings yet
- CABITAC Histology (Digestive) FinalDocument9 pagesCABITAC Histology (Digestive) FinalZhon CabitacNo ratings yet
- Radiography of The Pharnyx & Esophagus: Film CritiqueDocument30 pagesRadiography of The Pharnyx & Esophagus: Film CritiqueRika WulandariNo ratings yet
- MED Diseases of The EsophagusDocument4 pagesMED Diseases of The EsophagusJulie Anne AciertoNo ratings yet
- Surgery Osce StationsDocument37 pagesSurgery Osce Stationsmj4957No ratings yet
- Long Case DysphagiaDocument3 pagesLong Case DysphagiaNadia SalwaniNo ratings yet
- Trichobezoars: Case Reports and Review of LiteratureDocument4 pagesTrichobezoars: Case Reports and Review of LiteratureSajag GuptaNo ratings yet
- Small Intestines and Appendix - AnnoDocument97 pagesSmall Intestines and Appendix - AnnoJuan Lorenzo RequironNo ratings yet
- Med Surg 2 - 2 Diagnostic Examinations For Gastrointestinal SystemDocument18 pagesMed Surg 2 - 2 Diagnostic Examinations For Gastrointestinal SystemMaxinne RoseñoNo ratings yet
- Data Interpretation: Additional Resources: Section1: Interpreting Abdominal Radiographs Systematic ApproachDocument17 pagesData Interpretation: Additional Resources: Section1: Interpreting Abdominal Radiographs Systematic ApproachRaju NiraulaNo ratings yet
- 02 General SurgeryDocument34 pages02 General SurgerySarathi IrisNo ratings yet
- Esophagus Symptoms and InvestigationDocument7 pagesEsophagus Symptoms and InvestigationJinNo ratings yet
- Etal Angina  ": Does Rupture of The Aorta Occur?Document45 pagesEtal Angina  ": Does Rupture of The Aorta Occur?winston1234No ratings yet
- 1-5 BedahDocument9 pages1-5 BedahHalwia SiruaNo ratings yet
- Med Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Document7 pagesMed Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Maxinne RoseñoNo ratings yet
- ENG An.6 GI-imagingDocument45 pagesENG An.6 GI-imagingSimina ÎntunericNo ratings yet
- Esophagial DiseasDocument83 pagesEsophagial Diseasnajib.atif17No ratings yet
- RCPD Karagama 2021Document5 pagesRCPD Karagama 2021DEVNo ratings yet
- Gastro-Intestinal System Diagnostic TestsDocument11 pagesGastro-Intestinal System Diagnostic TestsFev BanataoNo ratings yet
- Gastrointestional IDocument45 pagesGastrointestional IDoc On CallNo ratings yet
- Chapter 1 Physical Examination 2002 Manual of Equine GastroenterologyDocument6 pagesChapter 1 Physical Examination 2002 Manual of Equine GastroenterologyJavier CeseñaNo ratings yet
- MATERI SESI 4.1 - MAR DR - HeryDocument9 pagesMATERI SESI 4.1 - MAR DR - HerydewiswahyuNo ratings yet
- Achalasia: Department of MedicineDocument21 pagesAchalasia: Department of Medicinekyliever100% (1)
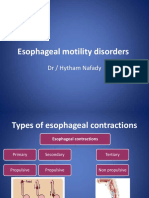
- Esophageal Motility Disorders: DR / Hytham NafadyDocument31 pagesEsophageal Motility Disorders: DR / Hytham NafadyRabie MeramNo ratings yet
- Esophagus Lecture Fatima NEW 2015Document31 pagesEsophagus Lecture Fatima NEW 2015Aileen EmyNo ratings yet
- Gastric Volvulus: Bang Chau, Susan DufelDocument2 pagesGastric Volvulus: Bang Chau, Susan DufelmustikaarumNo ratings yet
- (Surgery) Midterms PediatricsDocument5 pages(Surgery) Midterms Pediatricsalmira.s.mercadoNo ratings yet
- 116 - Alterations in GI EliminationDocument12 pages116 - Alterations in GI EliminationGino-o, KyleNo ratings yet
- By Subramaniyam Sabesan 4 Year Grodno State Medical UniversityDocument80 pagesBy Subramaniyam Sabesan 4 Year Grodno State Medical UniversitySam SabesNo ratings yet
- 445 CMED 222 Pathology of The Pancreas PDFDocument12 pages445 CMED 222 Pathology of The Pancreas PDFGepher CanoyNo ratings yet
- Medical-Surgical NCLEX Practice QUIZ Flashcards - QuizletDocument9 pagesMedical-Surgical NCLEX Practice QUIZ Flashcards - QuizletErika Bacarro100% (1)
- Fake Protagonist (Eng)Document1 pageFake Protagonist (Eng)ArianneJulienaCervaniaAndradaNo ratings yet
- TTS OST LyricsDocument1 pageTTS OST LyricsArianneJulienaCervaniaAndradaNo ratings yet
- Surgery II Schedule 2020-21 PDFDocument2 pagesSurgery II Schedule 2020-21 PDFArianneJulienaCervaniaAndradaNo ratings yet
- Dgms Circular 2015 & 2016Document104 pagesDgms Circular 2015 & 2016Ajeet KumarNo ratings yet
- Parent Consent (Youth Camp)Document3 pagesParent Consent (Youth Camp)Kim Kevin AveriaNo ratings yet
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- History & PEDocument45 pagesHistory & PESiddhant KotaNo ratings yet
- CD QuizDocument8 pagesCD QuizfilescrocsNo ratings yet
- Complete Biology 12 PDFDocument69 pagesComplete Biology 12 PDFAbdul Baseer50% (2)
- Case 41-2020: A 62-Year-Old Man With Memory Loss and Odd BehaviorDocument10 pagesCase 41-2020: A 62-Year-Old Man With Memory Loss and Odd BehaviorEzequiel BollatiNo ratings yet
- Healthy People 2020 AssignmentDocument4 pagesHealthy People 2020 Assignmentapi-242358046No ratings yet
- Anti Parkinson DrugsDocument20 pagesAnti Parkinson DrugsIrene Zae MwandotoNo ratings yet
- Frithiof's Saga PDFDocument252 pagesFrithiof's Saga PDFEsteban ArangoNo ratings yet
- Morning Report: Physician in ChargeDocument3 pagesMorning Report: Physician in ChargeDoctoRides 46No ratings yet
- EsomeprazoleDocument2 pagesEsomeprazolekpanggat100% (2)
- Setaria Palmifolia (J. Koenig) Stapf Sinonim Panicum Palmifolium WilldDocument5 pagesSetaria Palmifolia (J. Koenig) Stapf Sinonim Panicum Palmifolium WilldgianpriyaNo ratings yet
- Mood Stabilisers: PsychopharmacologyDocument50 pagesMood Stabilisers: Psychopharmacologymeno321No ratings yet
- Dwnload Full Excellence in Business Communication 11th Edition Thill Solutions Manual PDFDocument36 pagesDwnload Full Excellence in Business Communication 11th Edition Thill Solutions Manual PDFtarragon.cypraeavjblp100% (15)
- RCH PALS Study Guide - Web-121514Document5 pagesRCH PALS Study Guide - Web-121514Ryan N Brandy CooperNo ratings yet
- The Giant First YearDocument1,234 pagesThe Giant First YearEthan DyerNo ratings yet
- BÜHLMANN Laboratories AG Receives FDA Clearance For Its fCAL® Turbo Automated, Random Access Calprotectin TestDocument3 pagesBÜHLMANN Laboratories AG Receives FDA Clearance For Its fCAL® Turbo Automated, Random Access Calprotectin TestPR.comNo ratings yet
- PULPITISDocument35 pagesPULPITISapi-19916399No ratings yet
- Case Study DMDocument48 pagesCase Study DMBenj Villanueva100% (1)
- Peme NCLHDocument4 pagesPeme NCLHbaokhanh56No ratings yet
- End Stage Renal Disease (ESRD)Document21 pagesEnd Stage Renal Disease (ESRD)Dani DanyNo ratings yet
- Health Education and Contagious Diseases Group 1Document32 pagesHealth Education and Contagious Diseases Group 1Jason CamaNo ratings yet
- Drug Study2Document8 pagesDrug Study2zbestgurlNo ratings yet
- Sleep Disorder Screening Questionnaire PDFDocument2 pagesSleep Disorder Screening Questionnaire PDFSuci RahmayeniNo ratings yet
- Concept of Akhlat Arba (Four Humors)Document4 pagesConcept of Akhlat Arba (Four Humors)Joko RinantoNo ratings yet