You might also like
- Chapter 8 - Dry-Mount Fecal CytologyDocument12 pagesChapter 8 - Dry-Mount Fecal CytologyCarlos A. Flores OlivaresNo ratings yet
- Healing Codes: Grigori GrabovoiDocument47 pagesHealing Codes: Grigori GrabovoiPanther MelchizedekNo ratings yet
- L30 - Fpsc-Vrindavan Yojna 121, LGF Sanjar Gold Vrindavan Yojna R B Road LucknowDocument2 pagesL30 - Fpsc-Vrindavan Yojna 121, LGF Sanjar Gold Vrindavan Yojna R B Road LucknowPratap SinghNo ratings yet
- Leyva, Miguel Robert Ople 2151182765Document2 pagesLeyva, Miguel Robert Ople 2151182765Therese LeyvaNo ratings yet
- Z021 PDFDocument2 pagesZ021 PDFAditya RudraNo ratings yet
- Nohailic Dorin 500213dd8146202Document2 pagesNohailic Dorin 500213dd8146202Dorin NohailîcNo ratings yet
- PDFDocument3 pagesPDFJingleDiolaNo ratings yet
- ARMAN: Born: 12/15/1985 (Male 32) Test Date: 4/16/2018 8:39:25 AM Puskesmas KampalaDocument3 pagesARMAN: Born: 12/15/1985 (Male 32) Test Date: 4/16/2018 8:39:25 AM Puskesmas KampalaAkram KastiranNo ratings yet
- Ekg 59106Document3 pagesEkg 59106Eko KrahmadiNo ratings yet
- 13 Moh Eye Test - 20210622 - 0001Document1 page13 Moh Eye Test - 20210622 - 0001Psk Nellikuth100% (1)
- UntitledDocument1 pageUntitledAshish DhokNo ratings yet
- Hba1c (Glycosylated Hemoglobin)Document1 pageHba1c (Glycosylated Hemoglobin)NaeemNo ratings yet
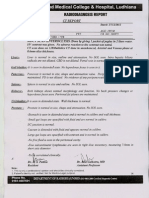
- MDCT Scan Enteroclysis: CT ReportDocument1 pageMDCT Scan Enteroclysis: CT ReportSuraj RautellaNo ratings yet
- Metodologie Mobilitate Pers Did 2016 2017Document2 pagesMetodologie Mobilitate Pers Did 2016 2017lunamirunaNo ratings yet
- Ecg PDFDocument1 pageEcg PDFManvir Singh DhindsaNo ratings yet
- Syne Vo Results 16496113Document4 pagesSyne Vo Results 16496113Nataliia NataliaNo ratings yet
- Lab Report - 040767-2122 - 1Document1 pageLab Report - 040767-2122 - 1Muhammad ImranNo ratings yet
- Blood C/E (Complete, CBC) : Lahore: 07 Jail Road, Main Gulberg - Karachi: Al Khaleej Plaza, Shaheed-e-Millat RoadDocument2 pagesBlood C/E (Complete, CBC) : Lahore: 07 Jail Road, Main Gulberg - Karachi: Al Khaleej Plaza, Shaheed-e-Millat RoadArslan MunawarNo ratings yet
- Complete Blood Count-2023-08-29t00 - 00 - 00Document2 pagesComplete Blood Count-2023-08-29t00 - 00 - 00Michamiel SerratoNo ratings yet
- Laboratory Investigation Report: Kindly Correlate With Clinical FindingsDocument3 pagesLaboratory Investigation Report: Kindly Correlate With Clinical FindingsNaveen 1802406No ratings yet
- Final Result: Patient Order Alters-U. Pflegeheim Gosmergartä Herr Elmar Reinhardt Gosmergasse 1 6463 Bürglen URDocument3 pagesFinal Result: Patient Order Alters-U. Pflegeheim Gosmergartä Herr Elmar Reinhardt Gosmergasse 1 6463 Bürglen URMarija PetrovicNo ratings yet
- WM68Document4 pagesWM68CloudCom TechnologyNo ratings yet
- Investigation Report: Flowcytometry. Carried Out by Sysmex XN-2000 SeriesDocument1 pageInvestigation Report: Flowcytometry. Carried Out by Sysmex XN-2000 SeriesNafis ChowdhuryNo ratings yet
- 8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NDocument3 pages8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NSudha SaravananNo ratings yet
- FMH Clinical Laboratories: Complete Blood CountDocument1 pageFMH Clinical Laboratories: Complete Blood CountZahid AliNo ratings yet
- Buletin de Analize Medicale Nr. 148727: Pagina 1 Din 2Document3 pagesBuletin de Analize Medicale Nr. 148727: Pagina 1 Din 2MadaNeli100% (1)
- Bilan de Santé (Anglais)Document5 pagesBilan de Santé (Anglais)Coralie HoarauNo ratings yet
- Complete Blood Count (CBC)Document2 pagesComplete Blood Count (CBC)educationNo ratings yet
- ( (Qjjoiqnrr) : Ypalytova Elena AleksandrovnaDocument2 pages( (Qjjoiqnrr) : Ypalytova Elena AleksandrovnaЕлена ИпалитоваNo ratings yet
- Bishnu Kumari NormalDocument1 pageBishnu Kumari NormalPrasannaRajGhimireNo ratings yet
- LABORATORY and PATHOLOGY Online Report: Patient InformationDocument3 pagesLABORATORY and PATHOLOGY Online Report: Patient InformationRamcoNo ratings yet
- Ssumangarg@gmail - Com 20220825193722Document13 pagesSsumangarg@gmail - Com 20220825193722Suman GargNo ratings yet
- Laboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleDocument2 pagesLaboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleumaNo ratings yet
- Shailendra Tamanekar 06102022 Report-1Document2 pagesShailendra Tamanekar 06102022 Report-1Shailendra TamanekarNo ratings yet
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703Document3 pagesD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703Rahul YadavNo ratings yet
- Urine Eaxmintaion ReportDocument7 pagesUrine Eaxmintaion Reportapi-3745021No ratings yet
- Hematology Test Name (Methodology) Result Flag Units Biological Reference IntervalDocument2 pagesHematology Test Name (Methodology) Result Flag Units Biological Reference IntervalMonu SahotaNo ratings yet
- Haematology: DR - Abhilash Kumar JainDocument1 pageHaematology: DR - Abhilash Kumar Jainseds5anuragNo ratings yet
- Covid19 920101369Document2 pagesCovid19 920101369Chirvasiu MihaiNo ratings yet
- S.Karthikeyan:::: Patient Age / Sex 33 Y / Male BranchDocument5 pagesS.Karthikeyan:::: Patient Age / Sex 33 Y / Male BranchkarthikeyanNo ratings yet
- CBC, Esr Total Count: Laboratory ServicesDocument1 pageCBC, Esr Total Count: Laboratory ServicesIslam FarhanaNo ratings yet
- Examination Results: Parent MaximeDocument1 pageExamination Results: Parent MaximeHenry HarendNo ratings yet
- Report 831a66a7 PDFDocument23 pagesReport 831a66a7 PDFViral PatelNo ratings yet
- Report Geeti PaulDocument22 pagesReport Geeti PaulSAIKAT PAULNo ratings yet
- MadhavDocument1 pageMadhavmadhav maheshwariNo ratings yet
- Report 33edcab8Document5 pagesReport 33edcab8sujithm435489No ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument3 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. Intervalaf dNo ratings yet
- Department of Hematology: Blood C/E (Complete, CBC)Document1 pageDepartment of Hematology: Blood C/E (Complete, CBC)Ahmed HannanNo ratings yet
- Report B6cc7e5bDocument3 pagesReport B6cc7e5bArchana SinghNo ratings yet
- 1-Diabetes Screening - PO1580805721-424Document4 pages1-Diabetes Screening - PO1580805721-424Ekta Anshul JainNo ratings yet
- Sikund Diagnostic CentreDocument3 pagesSikund Diagnostic CentreAnuja GairolaNo ratings yet
- 1-Senior Citizen Basic Package - PO3248534977-432Document16 pages1-Senior Citizen Basic Package - PO3248534977-432Krishna Nand RaiNo ratings yet
- Date 15/feb/2024 12:05PM 31/jul/23 11:10AM Unit Bio Ref IntervalDocument4 pagesDate 15/feb/2024 12:05PM 31/jul/23 11:10AM Unit Bio Ref IntervalrajorajisunnyNo ratings yet
- Date 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument12 pagesDate 28/mar/2023 10:09AM Unit Bio Ref Interval: Laboratory Investigation ReportChauhanNo ratings yet
- Laboratory For Medical Tests: Test ReportDocument2 pagesLaboratory For Medical Tests: Test ReportThornblad33No ratings yet
- Department of Molecular Biology. The Automotive Reasearch India - Covid 19 RT PCR - Pune - Fy2122 Test Name Result Unit Bio. Ref. Range MethodDocument2 pagesDepartment of Molecular Biology. The Automotive Reasearch India - Covid 19 RT PCR - Pune - Fy2122 Test Name Result Unit Bio. Ref. Range MethodanilsgaikwadNo ratings yet
- Complete Blood Count: Name DR Chetanbhai MojidaraDocument2 pagesComplete Blood Count: Name DR Chetanbhai Mojidarachetan mojidraNo ratings yet
- Date 30/nov/2021 02:37AM 29/nov/21 07:51PM Unit Bio Ref IntervalDocument2 pagesDate 30/nov/2021 02:37AM 29/nov/21 07:51PM Unit Bio Ref IntervalSaurabh PuriNo ratings yet
- L34 - Kota Lab Home Visit, 1-B-32 Talwandi, RHB, Near Talwandi CIRCLE, KOTA 324 006, RAJ KotaDocument2 pagesL34 - Kota Lab Home Visit, 1-B-32 Talwandi, RHB, Near Talwandi CIRCLE, KOTA 324 006, RAJ KotaAnupama MeenaNo ratings yet
- Medical Forms & Marshall Islands Certificate 7.12.18Document6 pagesMedical Forms & Marshall Islands Certificate 7.12.18EdgarRouNo ratings yet
- RCL Form A 2020Document4 pagesRCL Form A 2020michael enriquezNo ratings yet
- Parasitology Question and AnswersDocument22 pagesParasitology Question and AnswersofficialmwalusambaNo ratings yet
- Substance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryDocument43 pagesSubstance-Related Disorders: Professor DR Sirwan K Ali Department of PsychiatryAlan AhmadNo ratings yet
- Lecture 10 Antibiotics & Antiinfectives-1Document39 pagesLecture 10 Antibiotics & Antiinfectives-1Dr Haris AwanNo ratings yet
- Han Book of Signs in Clinical DermatologyDocument180 pagesHan Book of Signs in Clinical DermatologyLumière Cosmetología integralNo ratings yet
- Thyroid and Antithyroid DrugsDocument2 pagesThyroid and Antithyroid DrugsVidamazing 123No ratings yet
- C2L1 Activity by Charles MagpiliDocument4 pagesC2L1 Activity by Charles MagpiliCharles MagpiliNo ratings yet
- DR Sutap Yadav: Seronegative SpondyloarthropathiesDocument45 pagesDR Sutap Yadav: Seronegative SpondyloarthropathiesAyush PaudelNo ratings yet
- Trends in Pediatrics and Child Health-Unit IDocument35 pagesTrends in Pediatrics and Child Health-Unit IraghumscnNo ratings yet
- Clinical Effectiveness of Conservative ManagementDocument77 pagesClinical Effectiveness of Conservative ManagementD2S In'tl Business SolutionNo ratings yet
- Biliary System and Pancreatic DisorderDocument59 pagesBiliary System and Pancreatic DisorderAlda AdeliaNo ratings yet
- Sy 2021 2022 Science 2 q4 w3 Full Sped GTDocument3 pagesSy 2021 2022 Science 2 q4 w3 Full Sped GTJUNILLE B. YALUNG100% (1)
- Catalogue Web Envirolyte-LastDocument32 pagesCatalogue Web Envirolyte-LastalquimiaNo ratings yet
- Mahmud RAHMAN - Edexcel - Biology - Health, Disease and The Development of Medicines - KnowIT - GCSE 2Document49 pagesMahmud RAHMAN - Edexcel - Biology - Health, Disease and The Development of Medicines - KnowIT - GCSE 2Mahmud RahmanNo ratings yet
- F2 - Chapter 1 - 7Document23 pagesF2 - Chapter 1 - 7Andy LeungNo ratings yet
- 10 53424-Balikesirsbd 1146243-2548313Document4 pages10 53424-Balikesirsbd 1146243-2548313obenimNo ratings yet
- Symptomatic Apical Periodontitis Et Ology: Diagnosis and TreatmentDocument3 pagesSymptomatic Apical Periodontitis Et Ology: Diagnosis and TreatmentPrince AmiryNo ratings yet
- Human Diseases 6th Edition 2023_240401_210418Document610 pagesHuman Diseases 6th Edition 2023_240401_210418sc749518No ratings yet
- Igorot-Eng 003 PDFDocument103 pagesIgorot-Eng 003 PDFCatherine VillanuevaNo ratings yet
- Pathology of Bone - DADocument95 pagesPathology of Bone - DAabdillahNo ratings yet
- Venous Thromboembolic DiseaseDocument27 pagesVenous Thromboembolic DiseaseAndra BauerNo ratings yet
- The Sustained Impact of Tension Induced by Covid On The Food Service Industry Employees Gilles DraftDocument79 pagesThe Sustained Impact of Tension Induced by Covid On The Food Service Industry Employees Gilles DraftIbeanu ChimaNo ratings yet
- Dengue Duo Engue ns1 Ag Igg Igm SD BiolineDocument4 pagesDengue Duo Engue ns1 Ag Igg Igm SD Biolinersmbgss575No ratings yet
- Chapter IiDocument11 pagesChapter IiKadek IstaNo ratings yet
- Management of Dengue 2023Document10 pagesManagement of Dengue 2023Charlie CharcapeNo ratings yet
- BarakoDocument3 pagesBarakomhyckNo ratings yet
- 04 - ADHD Diagnosis and Testing Guide - ADD Symptom EvaluationsDocument7 pages04 - ADHD Diagnosis and Testing Guide - ADD Symptom EvaluationstenahernanNo ratings yet
- Colposcopy: Cervical Cancer Is Cancer of The Cervix (Lowermost Opening of The Uterus in TheDocument4 pagesColposcopy: Cervical Cancer Is Cancer of The Cervix (Lowermost Opening of The Uterus in TheMayuri SwamiNo ratings yet
- Testicular Examination OSCE GuideDocument9 pagesTesticular Examination OSCE Guidecharlyn206No ratings yet
- Investigation of Outbreak 2Document54 pagesInvestigation of Outbreak 2Evan Permana PutraNo ratings yet