You might also like
- Antinanginal DrugsDocument43 pagesAntinanginal DrugsHUZAIFA YAMAANNo ratings yet
- 6 AntianginalDocument38 pages6 AntianginalAyush GuptaNo ratings yet
- Antianginal ClassDocument32 pagesAntianginal ClassAnonymous whcvnPBeQNo ratings yet
- Anti-Angina Drugs for Chest Pain ReliefDocument60 pagesAnti-Angina Drugs for Chest Pain ReliefPranish SawantNo ratings yet
- Anti Angina (Hany)Document51 pagesAnti Angina (Hany)Angga AhadiyatNo ratings yet
- Angina NursingDocument62 pagesAngina NursingNikita JangraNo ratings yet
- Pharmacology Assignment 3Document31 pagesPharmacology Assignment 3Tujiyye kooNo ratings yet
- Cardio CHF Angina Drugs MegDocument3 pagesCardio CHF Angina Drugs MegJhonny pingolNo ratings yet
- Antianginal 171115034620Document34 pagesAntianginal 171115034620benny christantoNo ratings yet
- Vasodilators and Drugs Used in The Treatment of Angina PectorisDocument52 pagesVasodilators and Drugs Used in The Treatment of Angina PectorisAbdiweli AbubakarNo ratings yet
- Chapter 12 Vasodilators and Angina PectorisDocument7 pagesChapter 12 Vasodilators and Angina PectorisChristine Annmarie TapawanNo ratings yet
- 0 - Presentation Pharma Samra ShoukatDocument18 pages0 - Presentation Pharma Samra ShoukatMohib Ur RehmanNo ratings yet
- Drugs For Ischemic Heart DiseaseDocument44 pagesDrugs For Ischemic Heart DiseaseMbah GapinbissiNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisAyu PurbaNo ratings yet
- 2.drugsusedforthetreatmentofmi 121112230936 Phpapp02Document38 pages2.drugsusedforthetreatmentofmi 121112230936 Phpapp02omar khanNo ratings yet
- 3. Antianginal drugsDocument36 pages3. Antianginal drugscreativejoburgNo ratings yet
- Angina PectorisDocument24 pagesAngina PectorisAshwin Raghav SankarNo ratings yet
- Inotropic Agents.Document38 pagesInotropic Agents.Engy AdelNo ratings yet
- Anti Anginal DrugsDocument33 pagesAnti Anginal DrugsMuhammad AhmadNo ratings yet
- Antianginal and Antiischemic DrugsDocument18 pagesAntianginal and Antiischemic DrugsNaveen KumarNo ratings yet
- Pharmacology of Ischemic Heart DiseaseDocument51 pagesPharmacology of Ischemic Heart DiseaseabenezergebrekirstosNo ratings yet
- Pharmacology of Antianginal Drugs: Tri Widyawati M. IchwanDocument43 pagesPharmacology of Antianginal Drugs: Tri Widyawati M. IchwanYohanna SinuhajiNo ratings yet
- Anti-Anginal Drugs PharmacologyDocument24 pagesAnti-Anginal Drugs PharmacologyDharun RanganathanNo ratings yet
- Calcium Channel Blocker (CCB)Document36 pagesCalcium Channel Blocker (CCB)Nafisa TasnimNo ratings yet
- Lecture 7 Antianginal DrugsDocument28 pagesLecture 7 Antianginal DrugsjawadNo ratings yet
- Vasoactive PeptidesDocument35 pagesVasoactive PeptidesKetan patilNo ratings yet
- 9 Drugs Affecting Angina PectorisDocument3 pages9 Drugs Affecting Angina PectoristiaraNo ratings yet
- Angina Pectoris & Anti Anginal DrugsDocument46 pagesAngina Pectoris & Anti Anginal DrugsMohammad AliNo ratings yet
- Vasodil - Ischemic Heart DiseaseDocument52 pagesVasodil - Ischemic Heart DiseaseNorms YoramNo ratings yet
- Anti Anginal DrugsDocument26 pagesAnti Anginal DrugsAtharva PuranikNo ratings yet
- Antianginal Drugs.. Prof. Dr. Adeeb Al-ZubaidyDocument19 pagesAntianginal Drugs.. Prof. Dr. Adeeb Al-ZubaidySara AbbasNo ratings yet
- Antianginal DrugsDocument38 pagesAntianginal Drugslemmademe204No ratings yet
- Regional and Local VasodilatorsDocument29 pagesRegional and Local VasodilatorsNadejda DoroseviciNo ratings yet
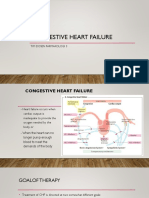
- CONGESTIVE HEART FAILURE - New-1Document32 pagesCONGESTIVE HEART FAILURE - New-1Agus SuprionoNo ratings yet
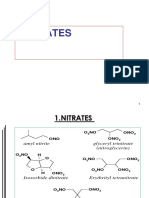
- NITRATESDocument21 pagesNITRATESFrancisNo ratings yet
- Hypotensive AgentsDocument48 pagesHypotensive AgentsFaizan Ahmad AliNo ratings yet
- Obat-Obat Untuk Angina PectorisDocument31 pagesObat-Obat Untuk Angina PectorisChie ZhumieNo ratings yet
- Drugs Used in The Treatment of Angina PectorisDocument5 pagesDrugs Used in The Treatment of Angina PectorisPadmanabha T SNo ratings yet
- Inotropic Agents for Congestive Heart Failure (CHFDocument38 pagesInotropic Agents for Congestive Heart Failure (CHFbenny christantoNo ratings yet
- Risk Factors and Diagnostic Tests for AnginaDocument3 pagesRisk Factors and Diagnostic Tests for AnginaRAMOS, Khristine JoesellNo ratings yet
- Nitrates: Agents Formulations Long-Vs. Short - Acting Onset of Action Duration of ActionDocument23 pagesNitrates: Agents Formulations Long-Vs. Short - Acting Onset of Action Duration of ActionIndra SucahyoNo ratings yet
- Anti Anginal Drugs - ArDocument9 pagesAnti Anginal Drugs - ArAnuj panditNo ratings yet
- Pharmacology AnginaDocument28 pagesPharmacology AnginaalijanmarwatNo ratings yet
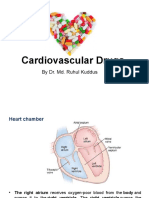
- Cardiovascular Drugs: by Dr. Md. Ruhul KuddusDocument56 pagesCardiovascular Drugs: by Dr. Md. Ruhul Kuddus53-Deepankar SutradharNo ratings yet
- Angina Pectoris: Chest Pain Due To Ischemia of Heart MusclesDocument27 pagesAngina Pectoris: Chest Pain Due To Ischemia of Heart MusclesJavar SodicNo ratings yet
- Antianginal DrugsDocument23 pagesAntianginal DrugsLA TSHTTNo ratings yet
- Farmakologi ANTIANGINADocument36 pagesFarmakologi ANTIANGINANovaNo ratings yet
- CVS 2 ParamedDocument39 pagesCVS 2 ParamedManikanta GupthaNo ratings yet
- Cardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerDocument131 pagesCardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerNiala AlmarioNo ratings yet
- Ischemic Cardiac Disease: Causes, Symptoms, Diagnosis and TreatmentDocument34 pagesIschemic Cardiac Disease: Causes, Symptoms, Diagnosis and TreatmentGopala HariNo ratings yet
- Congestive Cardiac Failure (1)Document27 pagesCongestive Cardiac Failure (1)Krupasagar Pn PalegarNo ratings yet
- Antianginal DrugsDocument25 pagesAntianginal DrugsTamta BokoveliNo ratings yet
- OBAT-OBATAN YANG MEMPENGARUHI SISTEM KARDIOVASKULERDocument51 pagesOBAT-OBATAN YANG MEMPENGARUHI SISTEM KARDIOVASKULERQuswah MaharaniNo ratings yet
- 4 Drugs of Congestive Heart FailureDocument5 pages4 Drugs of Congestive Heart FailureArfat AlmualladNo ratings yet
- Ischemic Heart DiseaseDocument31 pagesIschemic Heart DiseaseRohit SahNo ratings yet
- Post Operative Management of On-Pump and Off PumpDocument23 pagesPost Operative Management of On-Pump and Off Pumpamoeba418No ratings yet
- Anti Anginal DrugsDocument18 pagesAnti Anginal DrugsJuwairia tariqNo ratings yet
- Radiation ProtectionDocument85 pagesRadiation ProtectionASHUTOSH KHADANGANo ratings yet
- M.D. General Medicine Case Proforma for Central Nervous SystemDocument10 pagesM.D. General Medicine Case Proforma for Central Nervous SystemASHUTOSH KHADANGANo ratings yet
- Clinical Posting-2Document1 pageClinical Posting-2ASHUTOSH KHADANGANo ratings yet
- Antihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarDocument52 pagesAntihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarASHUTOSH KHADANGANo ratings yet
- Acid-Fast Stain (Ziehl-Neelsen Stain)Document15 pagesAcid-Fast Stain (Ziehl-Neelsen Stain)ASHUTOSH KHADANGANo ratings yet
- Antihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarDocument52 pagesAntihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarASHUTOSH KHADANGANo ratings yet
- Hartmann OT Catalogue WebDocument71 pagesHartmann OT Catalogue WebisabelNo ratings yet
- Meds Made EasyDocument40 pagesMeds Made EasyAreeba ShahidNo ratings yet
- ElvisDocument85 pagesElvisPaul SimoneNo ratings yet
- Mbbs Freshers ResumeDocument9 pagesMbbs Freshers ResumeTalha Noorani50% (2)
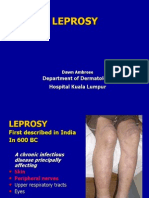
- 10 LeprosyDocument27 pages10 LeprosyMakWohWeiNo ratings yet
- Kong Research Paper DraftDocument4 pagesKong Research Paper Draftapi-463719483No ratings yet
- Orthotics For Beginners'!: or How Not To Fail Your FRCS Questions in OrthoticsDocument26 pagesOrthotics For Beginners'!: or How Not To Fail Your FRCS Questions in OrthoticsRudiyantoNo ratings yet
- Transes Tra-FundaDocument33 pagesTranses Tra-FundaJoshua DelantarNo ratings yet
- Oral Biotin 5MG Once DayDocument3 pagesOral Biotin 5MG Once Daylakshay kumarNo ratings yet
- CHARTINGDocument7 pagesCHARTINGGEN COLLANTESNo ratings yet
- Epidemics and PandemicsDocument36 pagesEpidemics and PandemicsRusu CristianaNo ratings yet
- Case ReportDocument18 pagesCase ReportWisnu WardanaNo ratings yet
- ALGORITHMDocument9 pagesALGORITHMNathalie DeebNo ratings yet
- Integrated Care Applying Theory To PracticeDocument429 pagesIntegrated Care Applying Theory To PracticeMyriam Hernández Núñez100% (1)
- An Introduction to Internal Medicine PropaedeuticsDocument46 pagesAn Introduction to Internal Medicine PropaedeuticsBraithwaite UmentaNo ratings yet
- e-CHECK (XS) HELPDocument3 pagese-CHECK (XS) HELPImas NurhayatiNo ratings yet
- N-acetylcysteine generic and brand names, dosage, mechanism of action, indications, contraindications, side effects and nursing implicationsDocument2 pagesN-acetylcysteine generic and brand names, dosage, mechanism of action, indications, contraindications, side effects and nursing implicationsAmira Paguyo QuilapioNo ratings yet
- MRSA BookDocument228 pagesMRSA BookIgd Pondok TjandraNo ratings yet
- Medical Device Risk Classification GuidanceDocument36 pagesMedical Device Risk Classification GuidanceGina ArcNo ratings yet
- Malaria in ChildrenDocument19 pagesMalaria in ChildrenAngel Ellene MarcialNo ratings yet
- Wound Dressing Checklist SKL 112 FINAL EDITDocument5 pagesWound Dressing Checklist SKL 112 FINAL EDITCamille GuintoNo ratings yet
- Comprehensive Hospital Strategic Plan ExampleDocument28 pagesComprehensive Hospital Strategic Plan ExampleEsteban R. Langlois100% (1)
- Ene 14885Document12 pagesEne 14885mikeNo ratings yet
- IQ4I Research & Consultancy Published A New Report On "Active Pharmaceutical Ingredient (API) Global Market - Forecast To 2027"Document7 pagesIQ4I Research & Consultancy Published A New Report On "Active Pharmaceutical Ingredient (API) Global Market - Forecast To 2027"VinayNo ratings yet
- Managing Clinical IncidentsDocument20 pagesManaging Clinical IncidentsAhmed HannoNo ratings yet
- Ayushman Bharat YojanaDocument28 pagesAyushman Bharat YojanaParth VasaveNo ratings yet
- Clinical Massage Therapy: Assessment and Treatment of Orthopedic MassageDocument35 pagesClinical Massage Therapy: Assessment and Treatment of Orthopedic MassagemassagekevinNo ratings yet
- Preventive Aspect of Vyayama (Physical Exercise) : January 2015Document8 pagesPreventive Aspect of Vyayama (Physical Exercise) : January 2015priyanka sharmaNo ratings yet
- InjectableDocument26 pagesInjectableAan KurniawanNo ratings yet
- Complementary therapy for reducing pain in gastritis patientsDocument28 pagesComplementary therapy for reducing pain in gastritis patientsYendy AftirandiNo ratings yet