You might also like
- Psych 155 Case StudyDocument2 pagesPsych 155 Case Studycoleenllb_usa100% (1)
- Mental Status Examination - Bring To LectureDocument6 pagesMental Status Examination - Bring To LectureJae ChoiNo ratings yet
- Mental Status ExaminationDocument8 pagesMental Status ExaminationRay ReyesNo ratings yet
- Mental Status ExaminationDocument3 pagesMental Status ExaminationjudssalangsangNo ratings yet
- Case Report: Psychotic Disorder Due To EpilepsyDocument8 pagesCase Report: Psychotic Disorder Due To EpilepsyAshraf IlmanNo ratings yet
- The Mental Status ExaminationDocument4 pagesThe Mental Status ExaminationMeow100% (1)
- Mental Status EvaluationDocument7 pagesMental Status Evaluationmunir houseNo ratings yet
- Case Study - Mental Status ExaminationDocument5 pagesCase Study - Mental Status ExaminationSrivathsanNo ratings yet
- Mental Status ExaminationDocument4 pagesMental Status ExaminationavigaeljoieNo ratings yet
- MSE Sample PDFDocument5 pagesMSE Sample PDFSam Raven AndresNo ratings yet
- Mental Status ExaminationDocument10 pagesMental Status Examinationlatasha deshmukhNo ratings yet
- Mental Status ExamDocument2 pagesMental Status Examkristel_nicole18yahoNo ratings yet
- Case Study Jared Tacey Youngstown State UniversityDocument13 pagesCase Study Jared Tacey Youngstown State Universityapi-402076669100% (1)
- Case No 1:-Bio DataDocument8 pagesCase No 1:-Bio DataSarah Saqib Ahmad100% (1)
- Clinical Assessment of A Psychiatric PatientDocument5 pagesClinical Assessment of A Psychiatric PatientAlex AthanNo ratings yet
- Lecture Notes On PsychiatryDocument38 pagesLecture Notes On PsychiatrysrossgellNo ratings yet
- OcdDocument11 pagesOcdNem AlNo ratings yet
- Nursing Care Plan For A Patient With SchizophreniaDocument14 pagesNursing Care Plan For A Patient With SchizophreniaJerilee SoCute WattsNo ratings yet
- Mental Status ExaminationDocument34 pagesMental Status Examinationkimbomd100% (2)
- Case 1 SchizophreniaDocument4 pagesCase 1 Schizophreniabent78100% (1)
- Case Scenario - Anxiety DisordersDocument2 pagesCase Scenario - Anxiety DisordersMary CuevaNo ratings yet
- Mental Status ExaminationDocument8 pagesMental Status ExaminationEmJay BalansagNo ratings yet
- PTSD ReportDocument11 pagesPTSD ReportMusab MohammadNo ratings yet
- Rating ScalesDocument4 pagesRating Scalesnkivc100% (3)
- CAGE Questionnaire For Alcohol MisuseDocument10 pagesCAGE Questionnaire For Alcohol MisuseJeremy BergerNo ratings yet
- Mental Health Case StudyDocument16 pagesMental Health Case Studyapi-472964417No ratings yet
- Final Study Guide Psyc101 Spring 2011Document14 pagesFinal Study Guide Psyc101 Spring 2011FirstLady Williams100% (1)
- Format MSEDocument3 pagesFormat MSESubir Banerjee0% (1)
- Basic Principles of Psychiatric NursingDocument5 pagesBasic Principles of Psychiatric NursingJo C Cuilan100% (1)
- Mental Health Case StudyDocument11 pagesMental Health Case Studyapi-546878677No ratings yet
- MseDocument5 pagesMseYnaffit Alteza UntalNo ratings yet
- 1 Case Formulation - BronDocument4 pages1 Case Formulation - BronallysoncaiNo ratings yet
- Case Study Development and Theoretical ExplanationDocument7 pagesCase Study Development and Theoretical ExplanationAssignmentLab.com100% (1)
- Case Analysis in Psych Bipolar Disorder BYDocument13 pagesCase Analysis in Psych Bipolar Disorder BYSheryl Ann Barit PedinesNo ratings yet
- Marino Case StudyDocument14 pagesMarino Case Studyapi-538721860No ratings yet
- Psych Report of RDA by Ernie GarciaDocument3 pagesPsych Report of RDA by Ernie GarciaLe Ar NieNo ratings yet
- A Psychiatric CaseDocument11 pagesA Psychiatric CaseGokul PoudelNo ratings yet
- GAD Case ReportDocument20 pagesGAD Case ReportZumer HashmiNo ratings yet
- Complex Trauma Screener For PediatriciansDocument7 pagesComplex Trauma Screener For Pediatriciansapi-434196971No ratings yet
- Sample Case Study For DMS-IV-TRDocument6 pagesSample Case Study For DMS-IV-TRohphooeyNo ratings yet
- Clinical Psych NotesDocument9 pagesClinical Psych Notesky knmt100% (1)
- Hamilton Rating Scale For Depression (HAM-D)Document4 pagesHamilton Rating Scale For Depression (HAM-D)Sana SajidNo ratings yet
- Stages of Psychotherapy Process: Zsolt UnokaDocument15 pagesStages of Psychotherapy Process: Zsolt UnokaNeil Retiza AbayNo ratings yet
- Structured Format For History and MSEDocument22 pagesStructured Format For History and MSEfizNo ratings yet
- Case Study - Mental HealthDocument9 pagesCase Study - Mental Healthapi-380891151No ratings yet
- Psychiatric Case StudyDocument12 pagesPsychiatric Case Studyapi-353526506100% (1)
- Case Presentation Bipolar 1 Manic TypeDocument18 pagesCase Presentation Bipolar 1 Manic Typenailed_heart0% (1)
- Varun Kumar, 2017 - Getting Started in PsychiatryDocument148 pagesVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- 13.6factitious Disorder: Simulate, Induce, or Aggravate Illness To Receive Medical Attention, RegardlessDocument5 pages13.6factitious Disorder: Simulate, Induce, or Aggravate Illness To Receive Medical Attention, Regardlessleeperlhan2000No ratings yet
- Process Recording Doument 1Document2 pagesProcess Recording Doument 1Susan Bloomquist DavisNo ratings yet
- Risk For ViolenceDocument5 pagesRisk For Violencemikaela_pascuaNo ratings yet
- A Case of DepressionDocument11 pagesA Case of DepressionKabilan R100% (2)
- Case StudyDocument17 pagesCase Studyapi-508597583No ratings yet
- Comprehensive Case StudyDocument10 pagesComprehensive Case Studyapi-545708059No ratings yet
- Early Onset Psychotic DisordersDocument51 pagesEarly Onset Psychotic Disordersdrkadiyala2100% (1)
- Case Study of Social PhobiaDocument1 pageCase Study of Social PhobiaSarah KhairinaNo ratings yet
- Case Study of ParanoiaDocument2 pagesCase Study of ParanoiaNsengimana Eric MaxigyNo ratings yet
- Summary of Andrew J. Wakefield's Waging War On The Autistic ChildFrom EverandSummary of Andrew J. Wakefield's Waging War On The Autistic ChildNo ratings yet
- Comprehensive Handbook of Psychological Assessment, Volume 1: Intellectual and Neuropsychological AssessmentFrom EverandComprehensive Handbook of Psychological Assessment, Volume 1: Intellectual and Neuropsychological AssessmentNo ratings yet
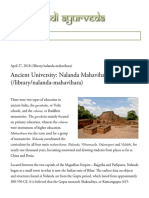
- Ancient University: Nalanda Mahavihara (/library/nalanda-Mahavihara)Document6 pagesAncient University: Nalanda Mahavihara (/library/nalanda-Mahavihara)Freddy Jr PerezNo ratings yet
- Gente Indígena Del MundoDocument3 pagesGente Indígena Del MundoFreddy Jr PerezNo ratings yet
- American CommercialsDocument5 pagesAmerican CommercialsFreddy Jr PerezNo ratings yet
- The Financial Management Behavior ScaleDocument17 pagesThe Financial Management Behavior ScaleFreddy Jr PerezNo ratings yet
- 0638 08F WTFDocument4 pages0638 08F WTFFreddy Jr PerezNo ratings yet
- F R7:y :RR G: " Bif 6," Ur#t"rtrc/e 3.t H (Uj Au6Document5 pagesF R7:y :RR G: " Bif 6," Ur#t"rtrc/e 3.t H (Uj Au6Freddy Jr PerezNo ratings yet
- Fotografía Del MundoDocument26 pagesFotografía Del MundoFreddy Jr PerezNo ratings yet
- Adm de PreciosDocument6 pagesAdm de PreciosFreddy Jr PerezNo ratings yet
- 0643 Corel Main CatDocument10 pages0643 Corel Main CatFreddy Jr PerezNo ratings yet
- 0644 Corel Sep CatDocument13 pages0644 Corel Sep CatFreddy Jr PerezNo ratings yet
- 0642 2008 21stC ProfessoriateDocument6 pages0642 2008 21stC ProfessoriateFreddy Jr PerezNo ratings yet
- 0641 2008 Case4ProfessionalizingDocument4 pages0641 2008 Case4ProfessionalizingFreddy Jr PerezNo ratings yet
- The Future of German in American Education: Summary Report, July 1996 Heidi Byrnes, Georgetown UniversityDocument6 pagesThe Future of German in American Education: Summary Report, July 1996 Heidi Byrnes, Georgetown UniversityFreddy Jr PerezNo ratings yet
- 0628 ADFL TeachingTAsDocument4 pages0628 ADFL TeachingTAsFreddy Jr PerezNo ratings yet
- 0631 Adfl91 Ny ArticDocument6 pages0631 Adfl91 Ny ArticFreddy Jr PerezNo ratings yet
- Foreign Language Testing, Part 2: Its Depth: Johnw. Ullcr, JRDocument9 pagesForeign Language Testing, Part 2: Its Depth: Johnw. Ullcr, JRFreddy Jr PerezNo ratings yet
- Managing A Zoo: Department: The Total Foreign LanguageDocument6 pagesManaging A Zoo: Department: The Total Foreign LanguageFreddy Jr PerezNo ratings yet
- An Alternative To The Current Literature Research Model OFDocument4 pagesAn Alternative To The Current Literature Research Model OFFreddy Jr PerezNo ratings yet
- 0625 ADFL Smith Need Grad TchrEdDocument3 pages0625 ADFL Smith Need Grad TchrEdFreddy Jr PerezNo ratings yet
- 0622 ADFL Guntermann Lang BusDocument4 pages0622 ADFL Guntermann Lang BusFreddy Jr PerezNo ratings yet
- Usage and Attitude (U&A) SurveyDocument3 pagesUsage and Attitude (U&A) SurveyNamit DuaNo ratings yet
- Ielts Speaking TipsDocument20 pagesIelts Speaking TipsМолдабекова Айсулу100% (1)
- Lembar Tugas Proyek - Descriptive TextDocument4 pagesLembar Tugas Proyek - Descriptive TextKusnadi Asnali100% (3)
- Pogoy Module 1Document5 pagesPogoy Module 1Nica PogoyNo ratings yet
- CURS.2 Limba - EnglezaDocument5 pagesCURS.2 Limba - EnglezaGrigoras Laura IoanaNo ratings yet
- DLL (Childrens Right 1)Document5 pagesDLL (Childrens Right 1)Eunice PlataNo ratings yet
- 24th European Congress of Psychiatry / European Psychiatry 33S (2016) S114-S289 S129Document1 page24th European Congress of Psychiatry / European Psychiatry 33S (2016) S114-S289 S129elouchNo ratings yet
- Reflection On Harry and Rosemary WongDocument3 pagesReflection On Harry and Rosemary Wongapi-264464926100% (1)
- Japanese GrammarDocument69 pagesJapanese GrammarRaulRujoi0% (1)
- M1CHAP1Document18 pagesM1CHAP1Eilla Marie GomosNo ratings yet
- Kassidy Dezutter PD Reference LetterDocument2 pagesKassidy Dezutter PD Reference Letterapi-379348658No ratings yet
- Literary Colloquial StyleDocument1 pageLiterary Colloquial Styleliza lyubetskayaNo ratings yet
- 5010 Unit 3 Writing AssignmentDocument4 pages5010 Unit 3 Writing AssignmentPrasastiNo ratings yet
- Interpersonal RelationshipDocument13 pagesInterpersonal RelationshiprashmiNo ratings yet
- Organizational Theory and Behavior - Portfolio Activity Unit 3Document4 pagesOrganizational Theory and Behavior - Portfolio Activity Unit 3Mohammad HamzaNo ratings yet
- Activity 3 (Final)Document2 pagesActivity 3 (Final)Debelyn CascayoNo ratings yet
- Opening of The MawDocument5 pagesOpening of The MawNegi SpringfieldNo ratings yet
- Heisenberg and The Transformation of Kantian PhilosophyDocument18 pagesHeisenberg and The Transformation of Kantian PhilosophyOswaldo ToledanoNo ratings yet
- Normative Symbol Digit Modalities Test Performance in A Community-Based SampleDocument6 pagesNormative Symbol Digit Modalities Test Performance in A Community-Based SamplePamGarcíaNo ratings yet
- Hildegard. E. Peplau: Theory of Interpersonal RelationsDocument16 pagesHildegard. E. Peplau: Theory of Interpersonal Relationsim. Elias100% (1)
- Action Research ProcessDocument48 pagesAction Research ProcessGlobal internetNo ratings yet
- What Is Discourse Analysis?Document17 pagesWhat Is Discourse Analysis?sabaNo ratings yet
- What Does Self-Regulation Means?Document2 pagesWhat Does Self-Regulation Means?Shahadath Hossain HimelNo ratings yet
- UntitledDocument127 pagesUntitledwilbert mark100% (2)
- "What Have I Ever Done To You" by Phoebe June Mcdonald ConlonDocument3 pages"What Have I Ever Done To You" by Phoebe June Mcdonald ConlonRosenda N. GulaneNo ratings yet
- I Beam WritingDocument2 pagesI Beam WritingDaniel KimNo ratings yet
- 8 EL 104 - Language in Education Policies in Southeast AsiaDocument2 pages8 EL 104 - Language in Education Policies in Southeast AsiaAngel Rodriguez100% (1)
- English 7 Q3 WK1Document50 pagesEnglish 7 Q3 WK1Cherry De PacenaNo ratings yet
- MetacogntionDocument18 pagesMetacogntionLouis SpencerNo ratings yet
- Case Study - Definition and Types in SociologyDocument9 pagesCase Study - Definition and Types in SociologyzahooorbhatNo ratings yet